中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 赵彬, 刘东, ZHAO Bin, LIU Dong
, 赵彬, 刘东, ZHAO Bin, LIU Dong目的 探讨临床药师在妊娠剧吐患者营养支持治疗中的作用。方法 临床药师积极参与1例妊娠剧吐患者营养支持的过程,结合患者疾病特点、药物不良反应,建议医生选择脂肪乳并进行营养支持处方的调整,提供个体化的药学服务。结果 通过临床药师参与药学监护,及时发现和处理患者营养支持治疗中潜在的问题,预防不良结局的发生。结论 药师参与妊娠剧吐患者营养支持治疗,可提高患者营养支持的有效性和安全性,促进药物的合理使用。
Objective To explore the role of clinical pharmacists in nutrition support therapy in the patients with hyperemesis gravidarum. Methods The clinical pharmacist played a positive role in nutrition support care of a patient with hyperemesis gravidarum by analysising disease characteristics and adverse drug reactions, providing suggestion on the selection of fat emulsion and offering an individualized pharmaceutical care.Results The clinical pharmacist recognized the potential risk in nutrition support plan, took modifications timely, and prevented the occurrence of unfavorable clinical outcomes. Conclusion The participation of clinical pharmacists in nutrition support therapy of the patients with hyperemesis gravidarum is beneficial to improve the efficacy and safety of nutrition support and promote the rational use of drugs.
高达91%的妊娠妇女在孕期会出现不同程度的恶心呕吐,严重的呕吐导致脱水、体质量减轻和酮症、电解质紊乱,从而进展为妊娠剧吐(hyperemesis gravidarum),其发生率为0.3%~3.6% [1]。迅速升高的雌激素或β人绒毛膜促性腺激素水平以及精神因素(如矛盾心理、焦虑)是诱发呕吐的可能因素[1]。对于因妊娠剧吐而无法经口进食的患者,营养支持不仅是满足能量代谢需求、避免营养不良的重要途径,也是影响妊娠剧吐患者预后的重要因素之一。脂肪乳作为肠外营养支持重要的组成部分,主要用于能量和必需脂肪酸的补充。妊娠期妇女在脂肪乳的选择上尤其重要。笔者通过参与1例妊娠剧吐患者营养支持的药学监护实践,阐述临床药师在患者营养支持治疗中的作用。
患者,女,40岁,身高160 cm,体质量60 kg,体重指数 25.8 kg·(m2)-1。因“宫内孕11+3周,呕吐1个月,加重5 d”入院。自述1个月前开始呕吐,尚能忍受,半个月前自述呕吐物中伴有血块,同时伴有尿量减少。5 d前无法进食进水,补液治疗后未见明显好转,收入华中科技大学同济医学院附属同济医院。体格检查: 体温36.5 ℃,脉搏65次·min-1,呼吸17次·min-1,血压143/95 mmHg (1 mmHg=0.133 kPa),血常规:白细胞(WBC)7.99×109·L-1,中性粒细胞百分比(the percentage of neutrophil,NE)72.2%。血小板(PLT)211×109·L-1,血红蛋白(HGB)139 g·L-1。肝肾功能:白蛋白(Alb)41 g·L-1,丙氨酸氨基转移酶(ALT)27 U·L-1,总胆红素12.1 μmol·L-1,直接胆红素3.8 μmol·L-1,血钾3.4 mmol·L-1,血尿素4.11 mmol·L-1,肌酐50 μmol·L-1,血糖3.8 mmol·L-1,血磷1.29 mmol·L-1,前白蛋白(prealbumin, PA )203 mg·L-1。尿常规:尿酮体(urine ketone,KET)≥7.8 mmol·L-1,尿胆原(urobilinogen,UGB) 33 μmol·L-1,尿蛋白(urine protein, PRO) 0.3 g·L-1,pH 7.0,尿相对密度(urine specific gravity, SG) 1.020,尿量200 mL·d-1。既往患高血压1年,规律治疗血压控制良好。1个月前就诊产科门诊,给予拉贝洛尔50 mg ,bid,口服,因呕吐严重已停药10 d。患者无药物、食物过敏史。入院诊断:孕11+3周、体外受精-胚胎移植妊娠、双胎妊娠、高龄初产、妊娠剧吐、高血压、酸中毒。
患者入院后予维生素B6 200 mg, qd,止吐治疗。因妊娠剧吐不能进食,于入院第3天起予肠外营养(total parenteral nutrition,TPN),初始治疗方案见
表1 初始肠外营养配方
Tab. 1 Formulas of the initial parenteral nutrition
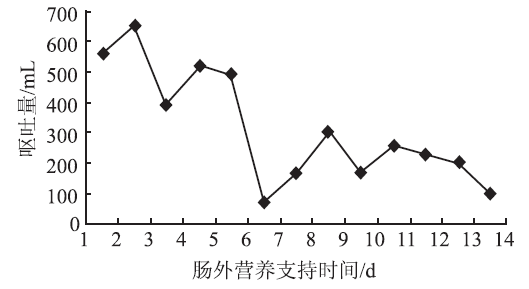
患者于第5天诉静脉输入营养液后呕吐明显严重,伴心慌、大汗等不适,停液后症状缓解。患者次日停用TPN,将其中的氨基酸、脂肪乳等分别输注。输注20%中长链脂肪乳(MCT/LCT)后,患者仍诉恶心呕吐明显,于第7天停用脂肪乳,其他的输液不变。患者呕吐较前好转,当日呕吐量为70 mL,较前一日明显减少(
为避免必需脂肪酸缺乏,于第8天改为20%长链脂肪乳(LCT)。同时考虑到患者ALT持续升高(14~51 U·L -1),药师建议将氨基酸换为富含支链氨基酸的肝用型氨基酸20AA,并开始口服护肝药多烯磷脂酰胆碱胶囊228 mg,tid。其后ALT缓慢下降。
药师在查房时发现患者肠外营养处方中维生素补充不足,建议医生在肠外营养处方中添加维生素。患者于第10天输入LCT脂肪乳后仍有恶心、呕吐加重情况,输注其他药物时无不适。自第11天起停用脂肪乳及其他营养补充制剂,未出现恶心呕吐加剧。随着患者病情的好转,医生和药师鼓励患者经口进食。第13天患者进食少量半流食后未见恶心呕吐加重,第16天能耐受正常饮食,未出现恶心呕吐,于第18天出院。出院时可正常饮食未见恶心呕吐,尿酮体、血钾、ALT及其他生化指标正常。
妊娠剧吐患者可尝试鼻饲管进行肠内营养,但往往妊娠剧吐患者无法耐受鼻饲管,且严重呕吐可增加吸入性肺炎的危险性。该患者入院时,病情加重不能进食饮水5 d,伴尿量减少,患者拒绝鼻饲喂养,因此选择肠外营养支持。初始肠外营养治疗方案处方中提供能量756 kJ;糖脂比为50.5%/49.5%;氨基酸42.5 g (0.76 g·kg-1),非蛋白能量∶氮148∶1。患者目前禁食禁水,每日756 kJ难以满足其生理需要,但考虑患者1周未进食,为避免再喂养综合征,因此初次营养支持只需提供目标能量的60%。患者多次输注肠外营养液及单独输注脂肪乳后恶心呕吐加重,停用后好转,考虑与脂肪乳相关性较大。恶心呕吐是酸中毒常见的临床表现,妊娠剧吐会限制能量尤其是碳水化合物的摄入,脂肪分解代谢增加,引起脂肪中间代谢产物β-羟基丁酸、乙酰乙酸和丙酮的生成和堆积,从而引起酸中毒[2]。患者出现恶心呕吐加剧时,其尿酮体已转阴,因此可排除酸中毒引起恶心呕吐加重。此外,多烯磷脂酰胆碱说明书中未提及恶心、呕吐不良反应。拉贝洛尔的不良反应中,恶心发生率14%,呕吐发生率<1%。但患者自述长期服用该药物未出现上述不良反应,排除合并用药不耐受引起的恶心呕吐加重。因此患者恶心呕吐加剧可能由脂肪乳引起。
有关脂肪乳过敏引起的不良反应报道较少,包括荨麻疹、面红、呼吸困难、心动过速、低血压、过敏性休克等。这些患者都对鸡蛋或大豆类食物过敏,脂肪乳中的磷脂和大豆蛋白被认为是过敏原[3-5]。而该患者无食物药物过敏史。通常脂肪乳相关的不良事件受输注速率、日剂量及使用时间长短的影响,脂肪乳最大清除率为3.8 g·kg-1·d-1,输注速率>2.5 g·kg-1·d-1会引起脂肪超载综合征[6]。该患者不存在上述风险因素。
采用不良反应判断标准对患者输注脂肪乳后出现不良反应进行关联性评价,具体如下:①在正常剂量合理的输注速率下,该患者静脉输入20%MCT/LCT和20%LCT后呕吐明显严重,伴心慌、大汗等不适,停液后症状缓解,再次使用又出现恶心呕吐加剧,用药与不良反应的出现有合理时间关系;②脂肪乳恶心呕吐发生率为2%~10%,反应符合脂肪乳已知的不良反应类型;③患者停用脂肪乳后呕吐较前减少,反应较前减轻;④患者恶心呕吐加重后,医生为其更换了脂肪乳的品种,有关再次使用可疑药品是否再次出现同样反应,无法确定;⑤患者恶心呕吐反应不能用患者合并用药及病情进展解释。综上所述,该患者恶心呕吐加剧症状为很可能为脂肪乳的不良反应。
妊娠剧吐是妊娠结局的独立风险因素,孕期全肠外营养支持能降低围产期胎儿发病率[7]。在脂肪乳的选择上,中长链脂肪乳因代谢功能较快且对免疫系统影响小,在临床上应用较长链脂肪乳普遍。但对于妊娠期患者,由于缺乏循证医学证据应避免使用。其说明书中也指出“应避免用于妊娠妇女或遵医嘱”。长链脂肪乳富含亚油酸和亚麻酸等必需脂肪酸,其中以亚油酸为主(ω-6/ω-3比值为6.5∶1),这对于胎儿神经系统的发育是必要的。其说明书上标明可安全用于妊娠患者。临床药师建议医生选择长链脂肪乳注射液。
患者经口进食减少,消化道缺乏食物刺激,影响胆汁分泌,导致胆汁酸和肝肠循环障碍,进而导致其ALT升高。因此药师建议肠外营养处方中改用肝用型氨基酸。此外,肠外营养中需给予常规剂量的水溶性维生素和多种微量元素,避免维生素缺乏引起的并发症。如维生素B1缺乏可引起Wernicke’s脑病,可通过每日肌内注射补充维生素B1 100 mg·d-1治疗[8]。维生素K的缺乏可引起胎儿凝血功能障碍,也有文献报道妊娠剧吐引起维生素K的缺乏导致胎儿出现了鼻骨发育不全[9]。长期禁食后给予营养支持需防止再喂养综合征,在营养治疗开始前应检查血、尿电解质,纠正水、电解质紊乱;经验性补充磷、钾、镁、维生素B1、复合维生素B;适当增加热量供应中脂肪的比例,因脂质代谢不会直接引起高胰岛素血症,不需消耗磷。妊娠期对某些维生素和微量元素的需求增加,如叶酸、烟酸、维生素B12、维生素B1、维生素B6、铬、铁、碘、锌等。
该患者在肠外营养支持过程中出现脂肪乳不耐受,临床药师根据制剂特点并结合患者生理特点建议选择合适的脂肪乳。但患者依然无法耐受。综合分析脂肪乳不良反应、疾病因素及合并用药不良反应,最后确定引起患者恶心呕吐加剧的原因很可能为脂肪乳不良反应。另外患者在营养支持的过程中出现转氨酶的轻微升高,药师建议选择肝用型氨基酸,减小肝脏负担。在药学查房时药师发现肠外营养处方中未添加维生素,建议添加以避免维生素缺乏引起的并发症。通过临床药师参与药学监护,及时发现和处理患者营养支持治疗中潜在的问题,有利于预防不良结局的发生,有利于提高患者营养支持的有效性和安全性,有利于促进药物的合理使用。
The authors have declared that no competing interests exist.

{kind=link}
{kind=link}