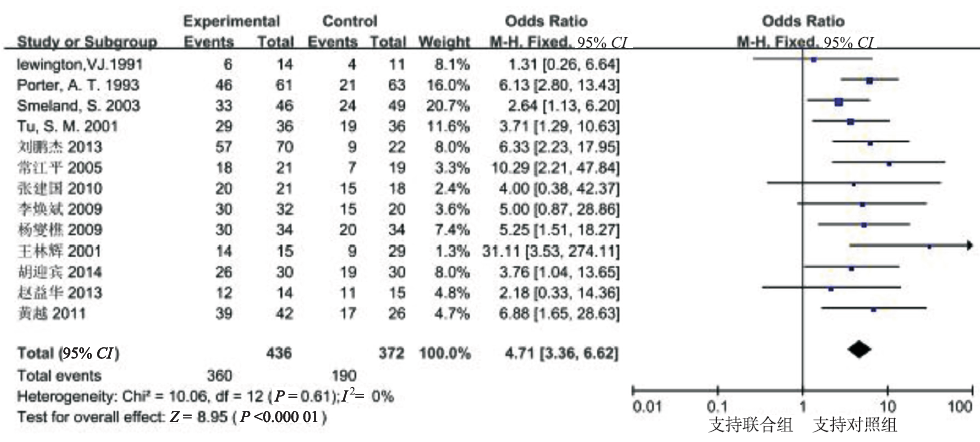
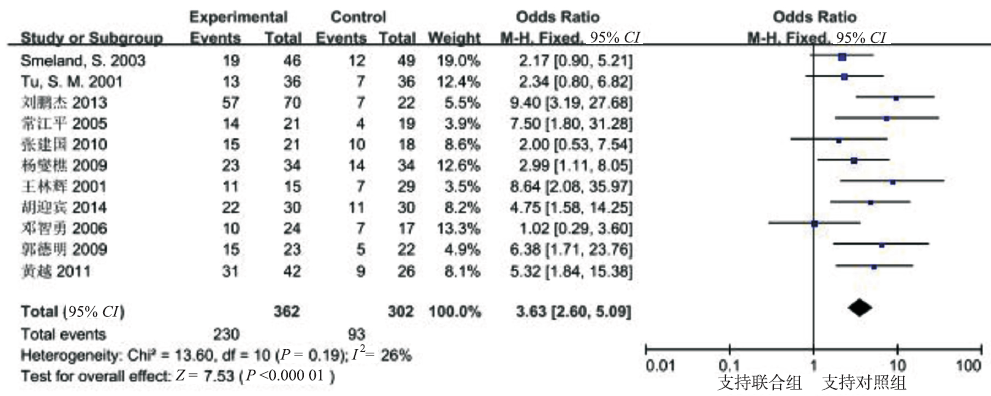
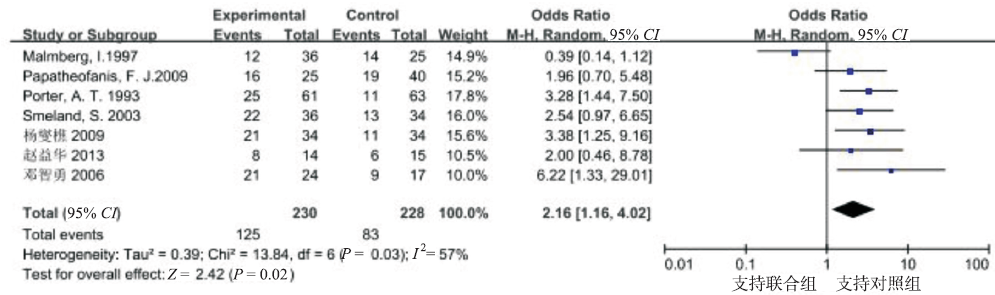
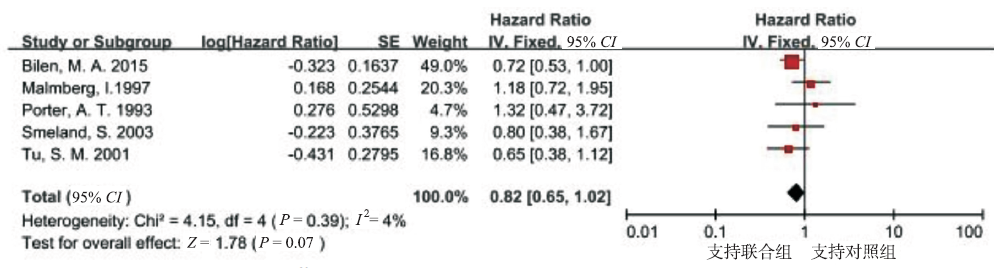
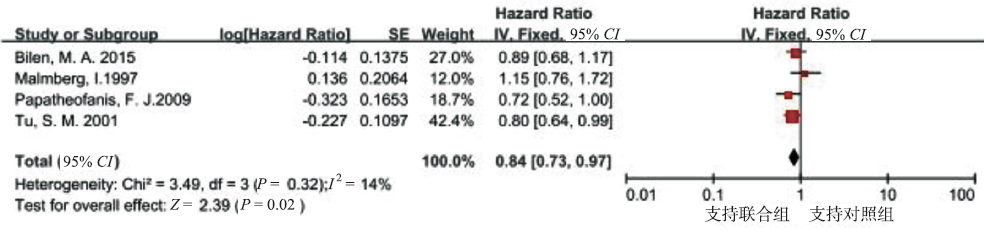
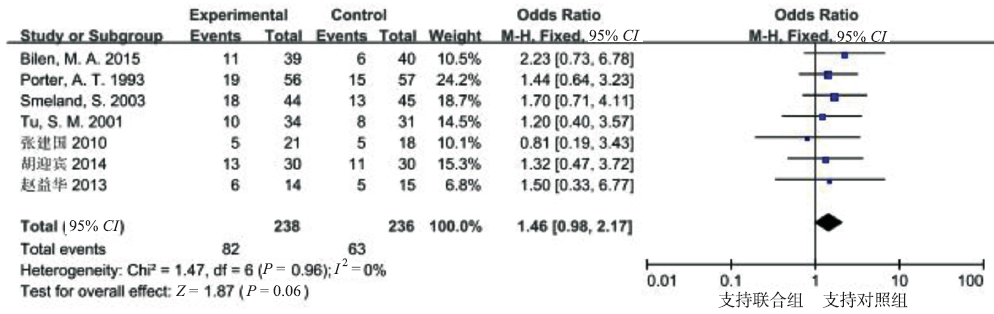
Objective To evaluate the efficacy and safety of combined therapy with 89Sr for treating skeletal-related events of prostate cancer. Methods Databases including PubMed,MEDLINE,EMBASE,the Cochrane library,CNKI,CBM and Wanfang were systematically searched since 89Sr was first reported in 1976 to September 2015 to include the randomized controlled trials (RCTs) of the combined therapy with 89Sr for skeletal-related events of prostate cancer.The statistical analysis was performed using Review Manager Version 5.2. Results A total of 18 RCTs involving 1 280 patients were analyzed.The results of meta-analysis indicated:there were statistically significant differences in the pain relief rate [OR=4.71,95%CI(3.34,6.62),P<0.000 1],decrement rate of bone metastasis [OR=3.63,95%CI(2.60,5.09),P<0.000 1] and improvement rate of life quality [OR=2.16,95%CI(1.16,4.02),P<0.05].Progression-free survival of patients in experimental group was significantly longer than that in control group [HR=0.84,95%CI(0.73,0.97),P=0.02].No significant difference was found in overall survival [HR=0.82,95%CI(0.65,1.02),P=0.07].There were no significant differences in the incidence of adverse events [OR=1.46,95%CI(0.98,2.17),P>0.05]. Conclusion Combined therapy with 89Sr has better efficacy and comparable safety profile compared with standard therapy.However,the quality and sample size of the included studies are limited,so more high-quality and large-sample RCTs are needed to verify the validity.
表1
纳入文献的基本特征
Tab.1
Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction
RAHEEMO,KULIDJIAN AA,WUC,et al.A novel patient-derived intra-femoral xenograft model of bone metastatic prostate cancer that recapitulates mixed osteolytic and osteoblastic lesions[J].J Transl Med,2011,9(28):185-189.
Prostate cancer metastasizes to bone in the majority of patients with advanced disease leading to painfully debilitating fractures, spinal compression and rapid decline. In addition, prostate cancer bone metastases often become resistant to standard therapies including androgen deprivation, radiation and chemotherapy. There are currently few models to elucidate mechanisms of interaction between the bone microenvironment and prostate cancer. It is, thus, essential to develop new patient-derived, orthotopic models. Here we report the development and characterization of PCSD1 (Prostate Cancer San Diego 1), a novel patient-derived intra-femoral xenograft model of prostate bone metastatic cancer that recapitulates mixed osteolytic and osteoblastic lesions. Methods A femoral bone metastasis of prostate cancer was removed during hemiarthroplasty and transplanted into Rag2-/-;??c-/- mice either intra-femorally or sub-cutaneously. Xenograft tumors that developed were analyzed for prostate cancer biomarker expression using RT-PCR and immunohistochemistry. Osteoblastic, osteolytic and mixed lesion formation was measured using micro-computed tomography (microCT). Results PCSD1 cells isolated directly from the patient formed tumors in all mice that were transplanted intra-femorally or sub-cutaneously into Rag2-/-;??c-/- mice. Xenograft tumors expressed human prostate specific antigen (PSA) in RT-PCR and immunohistochemical analyses. PCSD1 tumors also expressed AR, NKX3.1, Keratins 8 and 18, and AMACR. Histologic and microCT analyses revealed that intra-femoral PCSD1 xenograft tumors formed mixed osteolytic and osteoblastic lesions. PCSD1 tumors have been serially passaged in mice as xenografts intra-femorally or sub-cutaneously as well as grown in culture. Conclusions PCSD1 xenografts tumors were characterized as advanced, luminal epithelial prostate cancer from a bone metastasis using RT-PCR and immunohistochemical biomarker analyses. PCSD1 intra-femoral xenografts formed mixed osteoblastic/osteolytic lesions that closely resembled the bone lesions in the patient. PCSD1 is a new primary prostate cancer bone metastasis-derived xenograft model to study metastatic disease in the bone and to develop novel therapies for inhibiting prostate cancer growth in the bone-niche.
LEWINGTON VJ,MCEWAN AJ,ACKERY DM,et al.A prospective,randomised double-blind crossover study to examine the efficacy of strontium-89 in pain palliation in patients with advanced prostate cancer metastatic to bone[J].Eur J Cancer,1991,27(8):954-958.
Abstract The palliative efficacy of strontium-89 chloride has been evaluated in a prospective double-blind crossover study comparing it with stable strontium as placebo in 32 patients with prostate cancer metastatic to bone. Response was assessed 5 weeks after each treatment. 26 patients were evaluable. Complete pain relief was only reported following strontium-89 injection. Statistical comparison between placebo and strontium-89 showed clear evidence of a therapeutic response to strontium-89 compared with only a limited placebo effect (P less than 0.01).
PORTER AT,MCEWAN AJ,POWE JE,et al.Results of a randomized phase-Ⅲ trial to evaluate the efficacy of strontium-89 adjuvant to local field external beam irradiation in the management of endocrine resistant metastatic prostate cancer[J].Int J Radiat Oncol Biol Phys,1993,25(5):805-813.
MALMBERGI,PERSSONU,ASKA,et al.Painful bone metastases in hormone-refractory prostate cancer:economic costs of strontium-89 and/or external radiotherapy[J].Urology,1997,50(5):747-753.
In a prospective randomized Canadian trial, addition of radionuclide strontium (89Sr) to external radiotherapy (ER) was found to prolong the time to further ER by 15 weeks (35 versus 20, P = 0.006) compared to ER alone in patients with hormone-refractory metastatic prostate cancer (HRMPC). The total direct lifetime costs within the Swedish health care system for the following two treatment strategies was estimated as follows: (a) ER initially and in the event of relapse and (b) ER + 89Sr initially and ER in the event of relapse.Calculation of lifetime costs was based on the initial total treatment cost and the probability of future treatment costs. In a retrospective analysis, the average cost of a relapse treated with ER alone was calculated from the actual care consumption of 79 consecutive patients from the south of Sweden who received ER because of skeletal pain due to HRMPC. The costs related to ER included skeletal scintigraphy, ER, outpatient visits, inpatients days, and travel to the treatment center. When 89Sr was added, the cost also included the radionuclide and its administration. Costs in Swedish currency (SEK) were based on the regional tariff for 1993 (U.S. $1 = SEK 8.30).The initial cost for one relapse treated with ER alone was estimated to be SEK 31,011 (U.S. $3736) per patient resident within county (close to hospital) and SEK 48,585 (U.S. $5854) per patient resident out of county (far from hospital). The corresponding figure for initial addition of 89Sr to ER was SEK 43,426 (U.S. $5232) and 61,000 (U.S. $7349), respectively. However, comparison between estimated lifetime cost for the two treatment strategies indicated potential cost savings with initial addition of 89Sr to 3% SEK 2720 (U.S. $328) and 7% SEK 11,290 (U.S. $1360), respectively.Strontium-89 as initial supplement to ER for palliation of pain in HRMPC is beneficial both from the patient and lifetime health service costs perspectives.
TU SM,MILLIKAN RE,MENGISTUB,et al.Bone-targeted therapy for advanced androgen-independent carcinoma of the prostate:a randomised phase Ⅱ trial[J].Lancet,2001,357(9253):336-341.
Prostate carcinoma is linked to osteoblastic metastasis. We therefore investigated the value of bone-targeted consolidation therapy in selected patients with advanced androgen-independent carcinoma of the prostate.103 patients received induction chemotherapy, consisting of ketoconazole and doxorubicin alternating with estramustine and vinblastine. After two or three cycles of induction chemotherapy, we randomly assigned 72 patients who were clinically stable or responders to receive doxorubicin with or without strontium-89 (Sr-89) every week for 6 weeks.Overall 62 of the 103 (60%, 95% CI 50-70) patients had a 50% or greater reduction in serum prostate-specific antigen concentration that was maintained for at least 8 weeks, and 43 (42%, 32-52) had an 80% or greater reduction. 49 (52%) patients with bone pain at registration had complete resolution of pain. After follow-up of 67 patients until death, the estimated median survival for all 103 patients was 17.5 months (range 0.5-37.7). For the 36 patients randomly assigned to receive Sr-89 and doxorubicin, the median survival time was 27.7 months (4.9-37.7), and for the 36 who received doxorubicin alone it was 16.8 months (4.4-34.2) (p=0.0014). The hazard ratio was 2.76 (95% CI 1.44-5.29).Bone-targeted consolidation therapy consisting of one dose of Sr-89 plus doxorubicin once a week for 6 weeks, when given to patients with stable or responding advanced androgen-independent carcinoma of the prostate after induction chemotherapy, improved overall survival.
SMELANDS,ERIKSTEINB,AASM,et al.Role of stronti-um 2589 as adjuvant to palliative external beam radiotherapy is questionable:results of a double-blind randomized study[J].Int J Radiat Oncol Biol Phys,2003,56(5):1397-1404.
Abstract PURPOSE: To explore the efficacy of adjuvant (89)Sr applied with external beam radiotherapy (EBRT) to treat bone metastases. METHODS AND MATERIALS: Ninety-five patients were randomized to (89)Sr (Arm A) or saline (Arm B) on Day 1 of EBRT to demonstrate a reduction in 3-month physician-assessed subjective progression from 70% to 45%. RESULTS: At 3 and 6 months, no difference between treatment arms was observed in the progression rate. At 3 months, the physician-assessed response rate for all patients was 25%, with 46% of the patients progressing. The pretreatment use of opiates was independently associated with short progression-free survival. On the basis of the quality-of-life assessments, pain relief occurred in 50% of patients and 32% experienced improvement in global quality of life, without impact from (89)Sr. Differences were observed between the physician evaluation of radiotherapy efficacy and the patient assessment. In Arm A, serum alkaline phosphatase, but not serum prostate-specific antigen, decreased during the first 3 months after treatment. CONCLUSION: (89)Sr, adjuvant to ERBT, does not seem to reduce the number of patients with subjective progression at 3 months. Patients should be referred for palliative RT before their bone pain requires high doses of opiates. In radiotherapy trials, the evaluation of pain and pain relief remains problematic because of the confounding use of analgesics.
PAPATHEOFANIS FJ,SMITHC,NAJIBM.Improvement in sensory pain rating after palliative systemic radionuclide therapy in patients with advanced prostate cancer[J].Am J Ther,2009,16(2):127-132.
Abstract This study assessed whether baseline and short-term patient-reported quality of life (QOL) differs in patients with symptomatic metastatic prostate cancer undergoing palliative management using opioids, nonsteroidal anti-inflammatory agents (NSAIDs), (89)strontium chloride ((89)Sr), and samarium-lexidronam ((153)Sm). Males were grouped according to primary palliative intervention: opioids (n = 40), NSAIDs (n = 40), (89)Sr chloride (n = 25), and (153)Sm (n = 25). The short form of the self-administered McGill Pain Questionnaire was used to measure QOL at baseline, 4 and 8 weeks after initiation of treatment. Clinical data were collected from patients' medical records. Statistical analyses were conducted using descriptive methods and the Student t test. A significant increase in the sensory pain rating was observed in the patients treated by NSAIDs ([upward arrow]21%) and (89)Sr ([upward arrow]46%), whereas those treated by opioids ([downward arrow]27%) and (153)Sm ([downward arrow]27%) demonstrated a significant (P < 0.05) decrease in this subscore. There was a longitudinal decrease in QOL over time in patients treated by NSAIDs and (89)Sr as measured by the total pain rating score, whereas those treated with the other agents experienced improved QOL. This study demonstrates improvement in QOL achieved using (153)Sm, which is comparable to that achieved with the use of opioids during this observation interval.
BILEN MA,JOHNSON MM,MATHEWP,et al.Randomi-zed phase 2 study of bone-targeted therapy containing strontium-89 in advanced castrate-sensitive prostate cancer[J].Cancer,2015,121(1):69-76.
Abstract BACKGROUND: Radiopharmaceutical use may improve the survival time of patients with castrate-resistant prostate cancer and bone metastases. Whether androgen-deprivation therapy (ADT) combined with bone-targeted therapy provides a clinical benefit to patients with advanced castrate-sensitive prostate cancer has not been investigated. METHODS: Eighty male patients were enrolled, and 79 were randomized: 40 to the control arm and 39 to the strontium-89 (Sr-89) arm. After randomization, patients in both study arms received ADT, doxorubicin, and zoledronic acid. Kaplan-Meier methodology was used to evaluate the progression-free survival (PFS) time. Multivariate Cox proportional hazards regression was used to evaluate the effects of Sr-89 after controlling for the number of bone metastases. RESULTS: The median follow-up time for the 29 patients alive at the last follow-up was 76.9 months (range, 0.07-103.4 months). The median PFS time was 18.5 months (95% confidence interval, 9.7-49.4 months) for the control arm and 12.9 months (95% confidence interval, 8.9-72.5 months) for the Sr-89 arm (P65=65.86). No patient developed myelodysplastic syndrome or a hematologic malignancy. An unplanned subgroup analysis suggested increased efficacy of bone-targeted therapy with a greater extent of bone involvement (ie, >6 bone metastases vs ≤6 bone metastases on the bone scan). CONCLUSIONS: The data showed that bone-targeted therapy using 1 dose of Sr-89 combined with chemohormonal ablation therapy did not favorably affect the PFS of patients with castrate-sensitive prostate cancer. The combined therapy was feasible and safe. Whether such bone-targeted therapy provides a favorable outcome for those patients with a greater tumor burden in the bone warrants further investigation. Cancer 2015;121:69-76. 08 2014 American Cancer Society. 08 2014 American Cancer Society.
FURUBAYASHIN,NEGISHIT,URAS,et al.Palliative effects and adverse events of strontium-89 for prostate cancer patients with bone metastasis[J].Mol Clin Oncol,2015,3(1):257-263.
The aim of the present study was to evaluate the palliative effects and adverse events of strontium89 (Sr89) in patients with bone metastasis from prostate cancer. A total of 18 patients with prostate cancer and painful bone metastases, as diagnosed on bone scintigraphy, who were treated with Sr89 at the National Kyushu Cancer Center between February, 2008 and April, 2014 were reviewed. Of the 18 subjects, 13 (72.2%) achieved a pain response, whereas 5 were classified as pain nonresponders (27.8%). According to a logistic regression analysis, the preadministration characteristics, including age, prostatespecific antigen (PSA), alkaline phosphatase (ALP), history of bonemodifying agent administration, opioid use or palliative radiation therapy, time after the combined androgen blockade nadir and time since the pain onset, were not found to be significant predictors of the pain response. Similarly, the postadministration characteristics, including pain flares and the PSA and ALP response, were not found to be significant predictors of the pain response. Although no patients exhibited leukocyte toxicities, 2 patients experienced myelosuppression, involving anemia and thrombocytopenia, requiring transfusion of red cell or platelet concentrate following Sr89 treatment. of the 18 patients, 5 (27.8%) reported pain flares, all of whom were successfully treated with rescue drugs alone. According to the logistic regression analysis, of the preadministration characteristics, only ALP was identified as a significant predictor of bone marrow suppression in the univariate and multivariate analyses (P=0.006). Therefore, Sr89 treatment was found to be effective in ameliorating bone pain associated with metastasis from prostate cancer. Although it is difficult to identify the patients who will receive pain relief prior to Sr89 administration, this drug should be administered during the early stages due to the potential for bone marrow suppression in patients with high ALP levels.
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Sr联合内分泌疗法治疗前列腺癌骨转移的疗效观察
1
2005
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
内分泌联合SrCl治疗前列腺癌骨转移疗效分析
1
2006
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Sr联合内分泌疗法治疗前列腺癌骨转移的疗效观察
1
2009
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Sr联合内分泌治疗前列腺癌多发骨转移的临床研究
1
2009
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
SrCl联合内分泌疗法治疗前列腺癌骨转移
1
2009
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
唑来磷酸联合Sr治疗前列腺癌骨转移
1
2010
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Sr联合内分泌疗法治疗前列腺癌骨转移的疗效观察
1
2011
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
帕米膦酸二钠联合Sr治疗激素非依赖型前列腺癌骨转移疗效观察
1
2013
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
内分泌治疗在SrCl治疗前列腺癌骨转移中的作用
1
2013
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Sr治疗前列腺癌骨转移的疗效观察
1
2014
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
A prospective,randomised double-blind crossover study to examine the efficacy of strontium-89 in pain palliation in patients with advanced prostate cancer metastatic to bone
1
1991
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Results of a randomized phase-Ⅲ trial to evaluate the efficacy of strontium-89 adjuvant to local field external beam irradiation in the management of endocrine resistant metastatic prostate cancer
1
1993
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Painful bone metastases in hormone-refractory prostate cancer:economic costs of strontium-89 and/or external radiotherapy
2
1997
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Bone-targeted therapy for advanced androgen-independent carcinoma of the prostate:a randomised phase Ⅱ trial
1
2001
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Role of stronti-um 2589 as adjuvant to palliative external beam radiotherapy is questionable:results of a double-blind randomized study
2
2003
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Improvement in sensory pain rating after palliative systemic radionuclide therapy in patients with advanced prostate cancer
1
2009
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...
Randomi-zed phase 2 study of bone-targeted therapy containing strontium-89 in advanced castrate-sensitive prostate cancer
2
2015
... Basic characteristics of the included studies
第一作者及年份
例数
年龄/岁
干预措施
药物剂量
结局 指标
试验组
对照组
试验组
对照组
试验组
对照组
王林辉等[4](2001)
15
29
68.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
常江平等[5](2005)
21
19
69.3±6.5
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
148 MBq
邓智勇等[6](2006)
24
17
72.6
抗雄激素
抗雄激素
250 mg
250 mg
②③
89SrCl2
2.12 MBq·kg-1
郭德明[7](2009)
23
22
71.3±1.5
氟他胺
氟他胺
250 mg
250 mg
②
89SrCl2
55 μCi·kg-1
李焕斌等[8](2009)
32
20
69.4±16.7
抗雄激素
抗雄激素
不详
不详
①
89SrCl2
不详
杨燮樵等[9](2009)
34
34
68.5
氟他胺
氟他胺
250 mg
250 mg
①②③
89SrCl2
2.12 MBq·kg-1
张建国等[10](2010)
21
18
67.8
唑来膦酸
唑来膦酸
4 mg
4 mg
①②
89SrCl2
2.12 MBq·kg-1
黄越[11](2011)
42
26
71.5±2.7
氟他胺
氟他胺
250 mg
250 mg
①②
89SrCl2
40 μCi·kg-1
赵益华等[12](2013)
14
15
66.7±5.9
帕米膦酸
帕米膦酸
90 mg
90 mg
①③⑥
89SrCl2
1.48 MBq·kg-1
刘鹏杰等[13](2013)
70
22
63.0
抗雄激素
抗雄激素
不详
不详
①②
89SrCl2
不详
胡迎宾等[14](2014)
30
30
62~67
比卡鲁胺
比卡鲁胺
250 mg
250 mg
①②⑥
89SrCl2
2.12 MBq·kg-1
LEWINGTON等[15](1991)
16
16
71.3
抗雄激素
抗雄激素
250 mg
250 mg
①
89SrCl2
安慰药
150 MBq
PORTER等[16](1993)
61
63
75.2±1.9
抗雄激素
抗雄激素
不详
250 mg
①③④
89SrCl2
250 mg
⑥
MALMBERG等[17](1997)
36
35
69.5
放疗
放疗
不详
不详
③④⑤
89SrCl2
1.4 MeV
TU等[18](2001)
36
36
71.5
化疗
化疗
不详
不详
①②④
89SrCl2
安慰药
2.03 MBq·kg-1
安慰药
⑤⑥
SMELAND等[19](2003)
46
49
70.6
放疗
放疗
不详
不详
①②③
89SrCl2
0.9%氯化钠注射液
150 MBq
0.9%氯化钠注射液
④⑥
PAPATHEOFANIS等[20]
25
40
69.7±1.6
止痛药
止痛药
不详
不详
③⑤
(2009)
89SrCl2
安慰药
2.12 MBq·kg-1
安慰药
BILEN等[21](2015)
39
40
63.0
化疗
化疗
不详
不详
④⑤⑥
89SrCl2
40 mCi
Outcome indicators:①pain relief rate;②decrement rate of bone metastasis;③improvement rate of life quality;④overall survival;⑤progression-free survival;⑥incidence of adverse reaction ...

 , 任小强
, 任小强
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}