中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 赵亮, 徐德生, ZHAO Liang, XU Desheng
, 赵亮, 徐德生, ZHAO Liang, XU Desheng桥本甲状腺炎(Hashimoto’s thyroiditis,HT)是一种临床上常见的自身免疫性甲状腺疾病(autoimmune thyroid disease,AITD),以体内出现甲状腺特异性自身抗体和甲状腺淋巴细胞浸润为主要特征,最终导致甲状腺组织结构破坏和甲状腺功能低下。该病好发于30~50岁女性。每年全球范围内每1 000人中有0.3~1.5人发病[1-2]。国内报道HT是导致甲状腺功能减退(甲减)的最常见病因[3],每年以5%递增,女性多见,高碘地区发病率增高,占甲状腺疾病20%~25%。HT的发生主要与遗传、免疫、环境等因素有关,其中,免疫调节异常在HT 中具有重要作用,已经得到广泛认可。近年来,调节性T细胞(regulatory T cell,Treg)和辅助性T细胞17型(T helper 17,Th17)相继被发现。两者在分化和功能上存在相互拮抗,形成新的T细胞亚群细胞轴,使对HT 的发病机制有了新的认识。实验性自身免疫性甲状腺炎(experimental autoimmune thyroiditis,EAT)大鼠模型具有甲状腺抗体升高和甲状腺淋巴细胞浸润的病理表现,是作为研究桥本甲状腺炎常用的动物模型。笔者在本实验拟通过EAT动物模型,观察消瘿合剂对HT的药效学作用,并进一步从Treg/Th17细胞轴角度,探讨药效学作用机制。
清洁级SD大鼠,体质量120~160 g,雌性,上海斯莱克实验动物有限责任公司,动物生产许可证号:SCXK(沪)2012-0002,合格证号:2013001805889。置于室温为(24±2)℃,相对湿度为(20±5)%,昼夜明暗交替时间为12 h∶12 h,自由饮水、进食的清洁级动物房内饲养。
消瘿合剂由夏枯草、芥子、泽漆、海浮石、浙贝母、黄芪、党参、白芍、玄参、北沙参、制香附、土茯苓共12味药物组成。由上海中医药大学附属曙光医院制剂室生产制备(沪药制字Z04100928,批号:20150528)。因使用消瘿合剂原制剂直接动物灌胃,单次给药容积过大,故采用蒸发浓缩方式制备消瘿合剂浓缩液。具体方法:取消瘿合剂500 mL,蒸发浓缩至适宜体积,再加入双蒸水定容至250 mL,质量标准按消瘿合剂生产制备标准。雷公藤多苷片(上海复旦复华药业有限公司,批号:141203)。
血清游离三碘甲状腺原氨酸(free triiodothyronine,FT3)(批号:S10950167)、血清游离甲状腺素(free thyroxine,FT4)(批号:S10950166)、血清甲状腺球蛋白抗体(thyroglobulin antibody,TgAb)(批号:S10950139)放射免疫分析药盒,均购自北京北方生物技术研究所;Trizol(货号:1596-026,Invitrogen公司),SYBR Green PCR试剂盒(货号:K0223,Thermo公司),逆转录试剂盒(货号:K1622,Fermentas公司);Anti-rat CD4 FITC(货号:11-0040-82),Anti-rat CD25 APC(货号:17-0390-82),Anti-rat/mouse Foxp3 PE(货号:12-5773-82),Anti-rat/mouse IL-17A PE(货号:12-7177-81),均购自Ebioscience公司;乙酸肉豆蔻佛波醇(PMA)(货号:P8139),离子霉素(货号:I0634),莫能菌素(货号:M128779),猪甲状腺球蛋白(PTg,货号:T1126),完全弗氏佐剂(CFA,货号:F5881)、不完全弗氏佐剂(IFA,货号:F5506),均购自Sigma公司。
Real-time检测仪(型号ABI-7300,ABI公司),低温冷冻离心机(型号TG-16M,上海卢湘仪离心机仪器有限公司),流式细胞仪(型号Accuri C6,BD公司),石蜡切片机(型号SQ2125,徕克公司),正置显微镜(型号CX41,OLYMPUS公司)。
参照文献[4]方法。大鼠适应饲养1周后造模。PTg用磷酸盐缓冲液(PBS)溶解,浓度为1 g·L-1。第1周进行2次初次免疫,中间间隔2 d,将配制好的PTg溶液与完全弗氏佐剂(CFA)按体积比1∶1混合乳化,每只大鼠按PTg100 μg进行背部皮下多点注射。第2周进行加强免疫,每周1次,连续4周。
将SD大鼠按体质量分层,按数字表法随机分为正常对照组、模型对照组、雷公藤多苷组及消瘿合剂小剂量、大剂量组。除正常对照组外,其他组按“1.5”项造模。造模成功后,消瘿合剂小剂量组每日给予消瘿合剂浓缩液17.24 g·kg-1,相当于临床常用量。消瘿合剂大剂量组每日给予消瘿合剂浓缩液68.95 g·kg-1,相当于临床用药量的4倍。雷公藤多苷组每日给予雷公藤混悬液6.25 mg·kg-1。连续灌胃8周。
大鼠给予戊巴比妥麻醉。腹主动脉取血,一部分分离血清,存入1.5 mL Eppendoff管中,-20 ℃冰柜中保存,用于甲状腺功能及抗体检测;另一部分用于流式细胞术检测。分离甲状腺,甲醛固定,苏木精-伊红(HE)染色。另取脾脏存入2 mL Eppendoff管中,滴入Trizol试剂1 mL,-80 ℃冰柜中保存,用于Real-time 聚合酶链反应(RT-PCR)检测。
1.8.1 甲状腺功能及抗体测定 采用RIA法测定血清FT3、FT4、TgAb。
1.8.2 甲状腺形态学观察 采用常规HE染色,光镜下观察各组大鼠甲状腺炎症浸润情况。评分标准[5]:0分,无炎症细胞浸润;1分,2或3个滤泡之间的间质可见炎症细胞浸润;2分,至少一个或两个滤泡大小的炎症细胞病灶;3分,广泛浸润达总面积的10%~40%;4分,广泛浸润达总面积>40%~80%;5分,广泛浸润超过总面积80%。
1.8.3 RT-PCR测定大鼠脾脏 Foxp3 mRNA和IL-17 mRNA 取大鼠脾脏于1 mL的Trizol匀浆管充分裂解,三氯甲烷萃取后,异丙醇沉淀, 75%乙醇1 mL洗涤后,溶于DEPC水40 μL。取总RNA逆转录为cDNA。RT-PCR 25 μL反应体系:SYBRGreen Mix12.5 μL,上下游引物各0.5 μL,灭菌双蒸水9.5 μL,cDNA模板2 μL。反应程序:95 ℃,10 min(预变性95 ℃,15 s;60 ℃,45 s),扩增40个循环;95 ℃,15 s,60 ℃,1 min,95 ℃,15 s,60 ℃,15 s,扩增1个循环。Foxp3 mRNA、IL-17mRNA和内参照GAPDH基因扩增的引物序列由基尔顿生物科技(上海)有限公司设计并合成,引物序列见
表1 引物序列及PCR产物的大小
Tab.1 Primer sequence and predicated size of PCR product
1.8.4 流式细胞术检测大鼠外周血Treg细胞、Th17细胞比例 将大鼠腹主动脉血4 mL先后加入PBS溶液2 mL,人淋巴细胞分离溶液4 mL,收集单核细胞悬液。计数细胞,取约1×106细胞重悬于PBS100 μL中,按照试剂说明书进行抗体CD4、抗体IL-17染色,上机检测外周血Th17细胞比例;加入抗体CD4、抗体CD25、抗体Foxp3染色,上机检测外周血Treg细胞比例。
采用SPSS17.0版软件进行数据分析。先进行各组数据的正态性检验及方差齐性检验,对符合正态性分布的数据采用均数±标准差表示,满足方差齐性时,进行多组比较,采用单因素方差分析,符合组间均数比较时,采用最小显著差异法检验。非正态性分布数据采用中位数表示,并进行秩和检验。以
与正常对照组比较,模型对照组FT3、FT4、TgAb均升高,且差异有统计学意义(FT3:
表2 5组大鼠血清FT3、FT4和TgAb水平
Tab.2
Determination results of the serum level of FT3, FT4 and TgAb in five groups of rats
5组甲状腺炎症细胞浸润情况见
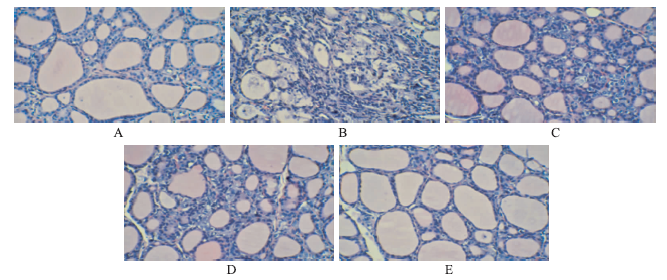
图1 5组大鼠甲状腺病理特征(HE染色,×200) A.正常对照组;B.模型对照组;C.雷公藤多苷组;D.消瘿合剂小剂量组;E.消瘿合剂大剂量组
Fig.1
Pathological feature of thyroid in five groups of rats (HE staining,×200)
A. normal control group; B. model control group; C. tripterygium glycoside group; D.low-dose
与正常对照组比较,模型对照组Foxp3 mRNA表达降低,IL-17 mRNA表达升高,均差异有统计学意义(
表3 5组大鼠甲状腺Foxp3 mRNA、IL-17mRNA表达
Tab.1
与正常对照组比较,模型对照组Treg细胞比例下降,Th17细胞比例升高,均差异有统计学意义(均
表4 5组大鼠外周血Treg细胞和Th17细胞比例
Tab.4
Ratio of Treg cells and Th17 cells in peripheral blood in five groups of rats %,
Th17 细胞和Treg细胞均属C
Treg 细胞主要以主动方式诱导和维持机体外周免疫耐受,调节机体免疫平衡。Treg细胞免疫抑制性是指其具有以下特性:①能够抑制C
自身免疫性甲状腺炎在中医学尚没有对应具体名称,但总体属于中医“瘿病”范畴[10]。历代医家对瘿病的认识,指出其病机始于情志不畅,肝郁气滞,日久则血行不畅而致血瘀,或气郁化火,火热炼液灼津,肝阳上亢,致木克脾土,致水谷运化失常,无法化气成精,精微化生不足,则肾阳亏虚。
从本研究结果来看,消瘿合剂能够降低自身免疫性甲状腺炎大鼠模型FT3、FT4水平,同时在改善炎症浸润、TgAb方面也被证明具有效果。作用机制研究显示,与正常对照组大鼠比较,模型对照组存在Foxp3 mRNA表达降低,IL-17表达升高的现象。同时,由C
The authors have declared that no competing interests exist.
| [1] |
More than a century has passed since the first description of Hashimoto thyroiditis (HT) as a clinicopathologic entity. HT is an autoimmune disease in which a breakdown of immune tolerance is caused by interplay of a variety of immunologic, genetic, and environmental factors. Thyrocyte injury resulting from environmental factors results in expression of new or hidden epitopes that leads to proliferation of autoreactive T and B cells. Infiltration of thyroid by these cells results in HT. In addition to the usual type of HT, several variants such as the fibrous type and Riedal thyroiditis are also recognized. The most recently recognized variant is immunoglobulin G4(+) HT, which may occur as isolated thyroid limited disease or as part of a generalized Ig4-related sclerosing disease. The relationship between HT and Riedel thyroiditis remains unclear; however, recent evidence seems to suggest that it may also be part of the spectrum of Ig4-related sclerosing disease. HT is frequently associated with papillary thyroid carcinoma and may indeed be a risk factor for developing this type of cancer. The relationship between thyroid lymphoma and HT on the other hand appears well established.
[本文引用:1]
|
| [2] |
Context Medical centers worldwide report an increased frequency of Hashimoto's thyroiditis (HT) and thyroid cancer (TC), two environmentally influenced diseases. In Sicily, data on HT are available for the province of Messina (1975–2005); data on TC are available for the whole island (2002–2004), with the volcanic province of Catania having the highest incidence. Objective To replicate in Catania, on comparable years, the HT data of Messina. Design, Methods, Setting Review of the clinical records of patients in years 1995–2005 to compare presentation and yearly changes of HT. During 1995–2005, records were computer stored in the Endocrine Divisions of the University Hospitals of Catania and Messina, two tertiary referral centers. Results Catania is outnumbered by Messina (742 vs. 3,409 HT patients). Similar were the linear increase in the yearly number of HT patients, rates of thyroid dysfunctions though with different proportions of subclinical and overt hypothyroidism, and rates of positiveness for TgAb or TPOAb. Different were age and its yearly trend; gender distribution and rates of the sonography variants, though yearly trends were similar. Conclusion The HT epidemics is smaller in Catania, with changes in presentation overlapping partially those in Messina. Whatever environmental factors might be involved, they (and/or their intensity) were not necessarily the same in these provinces. Intriguingly, the expected number of TC in HT patients with thyroid nodules in Catania is congruent with that of the general population of this province, but it is far less than in the Messina province. Thus, TC and HT incidences could be influenced by distinct environmental factors.
[本文引用:1]
|
| [3] |
Iodine is an essential component of thyroid hormones; either low or high intake may lead to thyroid disease. We observed an increase in the prevalence of overt hypothyroidism, subclinical hypothyroidism, and autoimmune thyroiditis with increasing iodine intake in China in cohorts from three regions with different levels of iodine intake: mildly deficient (median urinary iodine excretion, 84 microg per liter), more than adequate (median, 243 microg per liter), and excessive (median, 651 microg per liter). Participants enrolled in a baseline study in 1999, and during the five-year follow-up through 2004, we examined the effect of regional differences in iodine intake on the incidence of thyroid disease.Of the 3761 unselected subjects who were enrolled at baseline, 3018 (80.2 percent) participated in this follow-up study. Levels of thyroid hormones and thyroid autoantibodies in serum, and iodine in urine, were measured and B-mode ultrasonography of the thyroid was performed at baseline and follow-up.Among subjects with mildly deficient iodine intake, those with more than adequate intake, and those with excessive intake, the cumulative incidence of overt hypothyroidism was 0.2 percent, 0.5 percent, and 0.3 percent, respectively; that of subclinical hypothyroidism, 0.2 percent, 2.6 percent, and 2.9 percent, respectively; and that of autoimmune thyroiditis, 0.2 percent, 1.0 percent, and 1.3 percent, respectively. Among subjects with euthyroidism and antithyroid antibodies at baseline, the five-year incidence of elevated serum thyrotropin levels was greater among those with more than adequate or excessive iodine intake than among those with mildly deficient iodine intake. A baseline serum thyrotropin level of 1.0 to 1.9 mIU per liter was associated with the lowest subsequent incidence of abnormal thyroid function.More than adequate or excessive iodine intake may lead to hypothyroidism and autoimmune thyroiditis.
[本文引用:1]
|
| [4] |
目的:观察海藻玉壶汤加减方对实验性自身免疫性甲状腺炎(EAT)大鼠甲状腺中Fas/FasL蛋白表达的影响。方法:在建立EAT大鼠模型的基础上,设立海藻玉壶汤加减方(浸膏)高、低剂量组、模型组、正常组、丙基硫氧嘧啶组、雷公藤多苷片组、夏枯草膏组,采用免疫组化法检测EAT大鼠的Fas/FasL蛋白表达情况。结果:正常组甲状腺组织Fas和FasL免疫阳性物表达颜色较浅,表达范围小,模型组免疫阳性物颜色较深,表达范围广。其中,模型组的Fas和FasL表达程度与正常组相比有显著性差异(P〈0.01);海藻玉壶汤加减方高剂量组、雷公藤多苷片组与丙基硫氧嘧啶组、夏枯草膏组相比有显著性差异(P〈0.01)。结论:海藻玉壶汤加减方高剂量组对凋亡蛋白Fas/FasL的表达具有一定的抑制作用,提示海藻玉壶汤加减方可能通过抑制各凋亡蛋白的表达,从而避免细胞过度凋亡对甲状腺组织的破坏。
[本文引用:0]
|
| [5] |
ABSTRACT Thyroglobulin (Tg) is unique in its ability to incorporate and store available iodine in the form of iodotyrosyl residues. Iodination of Tg has been known to increase its immunopathogenicity in experimental animals, presumably through the formation of iodine-containing neoantigenic determinants that can elicit an autoimmune response, but defined pathogenic Tg peptides carrying iodotyrosyls have not yet been identified. We report in this study that a systematic, algorithm-based search of mouse Tg has delineated three iodotyrosyl-containing peptides that activate autoreactive T cells and cause experimental autoimmune thyroiditis in normal CBA/J mice. These peptides (aa 117-132, 304-318, and 1931-1945) were not immunogenic in their native form, and iodination of tyrosyls facilitated either peptide binding to MHC or T cell recognition of the peptide. These results demonstrate that iodotyrosyl formation in normal Tg confers pathogenic potential to certain peptides that may otherwise remain innocuous and undetectable by conventional mapping methods.
[本文引用:1]
|
| [6] |
T helper type 17 (Th17) cells are a distinct lineage of T cells that produce the effector molecules IL-17, IL-17F, IL-21, and IL-22. Th17 cells have been shown to have critical roles in autoimmunity and tissue inflammation. However, emerging evidence also shows these cells are critical regulators of host immunity against bacterial, fungal, and viral infections at mucosal surfaces. Moreover, these cells can be induced following vaccination and have been shown to be critical for vaccine efficacy against both extracellular and intracellular pathogens. In this issue, we summarize recent progress in our understanding of the function of Th17 cells and where these cells fit in protective immunity and immunopathology.
|
| [7] |
|
| [8] |
|
| [9] |
The immune system has evolved a variety of mechanisms to achieve and maintain tolerance both centrally and in the periphery. Central tolerance is achieved through negative selection of autoreactive T cells, while peripheral tolerance is achieved primarily via three mechanisms: activation-induced , anergy, and the induction of regulatory T cells. Three forms of these regulatory T cells have been described: those that function via the production of the cytokine (T regulatory 1 cells), transforming growth factor beta (Th3 cells), and a population of T cells that suppresses proliferation via a cell-contact-dependent mechanism (+CD25+ TR cells). The present review focuses on the third form of peripheral tolerance - the induction of regulatory T cells. The review will address the induction of the three types of regulatory T cells, the mechanisms by which they suppress T-cell responses in the periphery, the role they play in immune , and the potential these cells have as therapeutic agents in immune-mediated disease.
DOI:10.1186/ar1226
[本文引用:1]
|
| [10] |
基于桥本甲状腺炎的发病特征及对中医古今文献的考究,现对桥本甲状腺炎的中医病名进行辨析。桥本甲状腺炎临床表现多种多样,主要有三种阶段表现:甲状腺功能亢进期、甲状腺功能正常期、甲状腺功能减低期。现经古文考证辨析:"瘿"相当于无症状单纯甲状腺肿的肿桥本甲状腺炎,"瘿.瘿气"相当于桥本甲状腺炎合并甲状腺功能亢进,"瘿.虚劳"为桥本甲状腺炎合并甲状腺功能减低,等等。通过规范的桥本中医命名使桥本病中医诊断更加系统,方便临床辨证施治。
|
| [11] |
|
| [12] |
正消瘿扶正方为我院名老中医夏少农治疗桥本甲状腺炎之经验方,临床疗效显著。近年我们将其与优甲乐对照治疗桥本甲状腺炎患者30例,现报道如下。1临床资料1.1一般资料所有病例来自于本院中医外科2011年11月初至2013年3月初门诊,共60例,随机分为2组。治疗组30例:男9例,女21例;年龄24~47岁,平均年龄34岁;病程4个月至6年,平均病程26个月。对照组30例:男11例,女19
[本文引用:1]
|

{kind=link}
{kind=link}