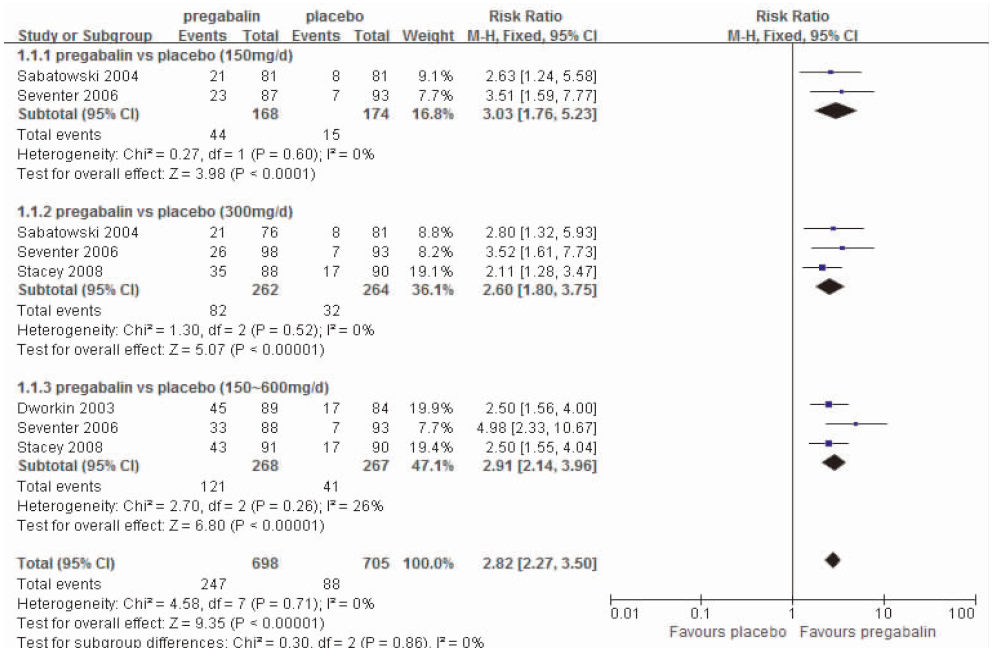
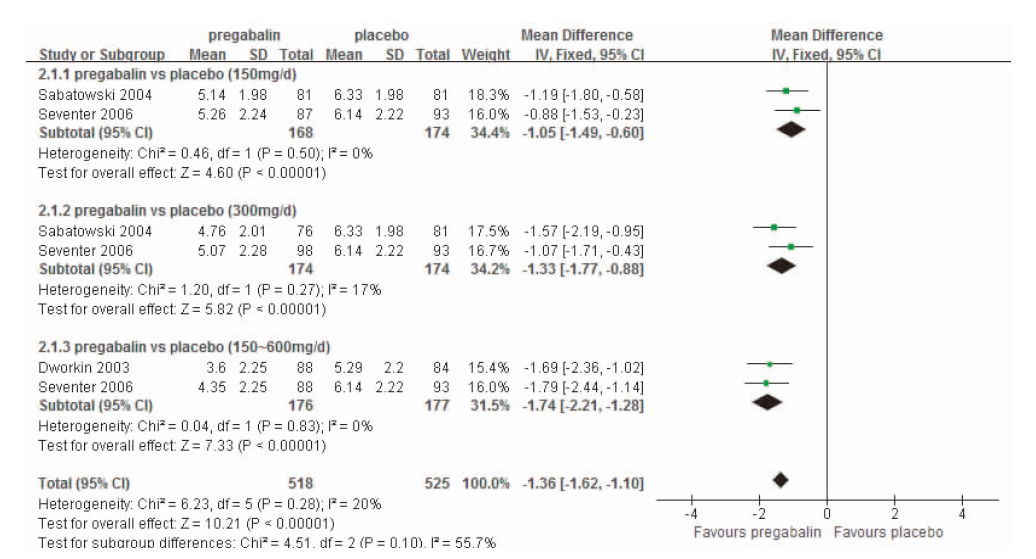
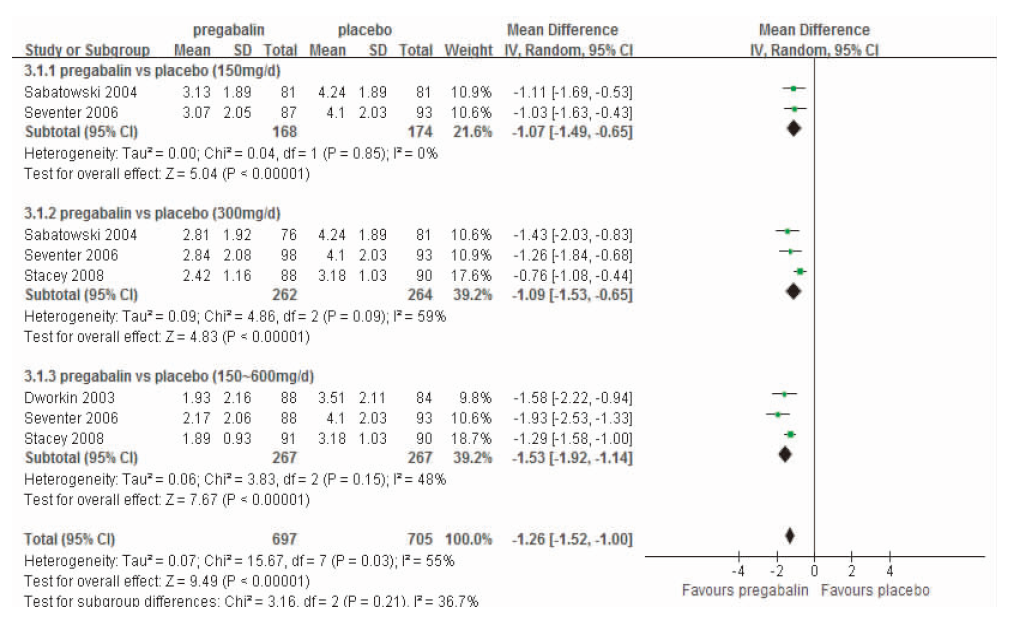
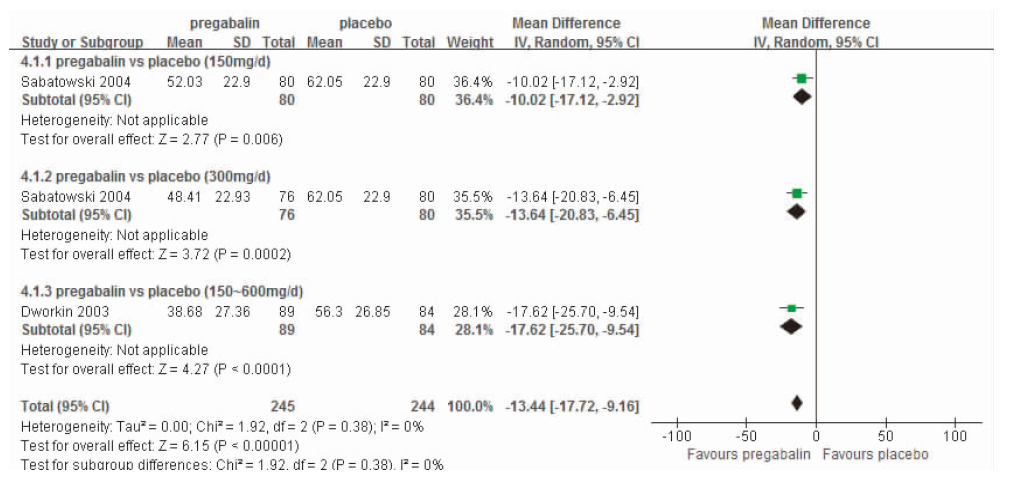
1.1.4 结局指标 采用下列一项或者多项有效性和安全性指标的试验可被纳入:①反应有效率( 平均疼痛评分减少≥50%的比例);②研究终点疼痛评分;③疼痛对睡眠的影响程度评分;④VAS评分;⑤患者总体印象变化(patient global impression of change,PGIC);⑥不良反应发生率,包括眩晕、嗜睡、头痛、外周水肿及口干等。
仅纳入1项研究,98例患者。普瑞巴林日剂量第1周150 mg,第2周300 mg,第3周开始600 mg,疗程4周。5%利多卡因膏,每12 h在疼痛最甚处给予2或3块药膏,疗程4周。研究结果显示,在有效性方面,普瑞巴林反应有效率较利多卡因低(65.0% vs 82.1%),SF-MPQ中VAS评分改变低于利多卡因(-17.2±25.57 vs -25.9±23.14);在安全性方面,普瑞巴林不良反应发生率较利多卡因高(42.9% vs 28.0%),主要不良反应包括眩晕、疲乏、嗜睡和头痛,均可耐受。
一、定义及分类 国际疼痛学会(International Association for the Study of Pain,IASP)于1994年将神经病理性疼痛(Neuropathic Pain,NP)定义为:“由神经系统的原发损害或功能障碍所引发或导致的疼痛(Paininitiated or caused by a primary lesion or dysfunction in the nervous system).2008年,IASP神经病理性疼痛特别兴趣小组(NeuPSIG)将该定义更新为:“由躯体感觉系统的损害或疾病导致的疼痛”(neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory system)[1].
DWORKIN RH, CORBIN AE, YOUNG JP, et al.Pregabalin for the treatment of postherpetic neuralgia: a randomized,placebo-controlled trial[J]. Neurology, 2003, 60(8): 1274-1283.
Abstract OBJECTIVE: To evaluate the efficacy and safety of pregabalin in the treatment of postherpetic neuralgia (PHN). METHODS: The authors conducted a multicenter, parallel-group, double-blind, placebo-controlled, 8-week, randomized clinical trial in PHN, defined as pain for 3 or more months following herpes zoster rash healing. Patients (n = 173) were randomized to treatment with pregabalin or placebo. Patients randomized to pregabalin received either 600 mg/day (creatinine clearance > 60 mL/min) or 300 mg/day (creatinine clearance 30 to 60 mL/min). The primary efficacy measure was the mean of the last seven daily pain ratings. Secondary endpoints included additional pain ratings, sleep interference, quality of life, mood, and patient and clinician ratings of global improvement. RESULTS: Pregabalin-treated patients had greater decreases in pain than patients treated with placebo (endpoint mean scores 3.60 vs 5.29, p = 0.0001). Pain was significantly reduced in the pregabalin-treated patients after the first full day of treatment and throughout the study, and significant improvement on the McGill Pain Questionnaire total, sensory, and affective pain scores was also found. The proportions of patients with >or=30% and >or=50% decreases in mean pain scores were greater in the pregabalin than in the placebo group (63% vs 25% and 50% vs 20%, p = 0.001). Sleep also improved in patients treated with pregabalin compared to placebo (p = 0.0001). Both patients and clinicians were more likely to report global improvement with pregabalin than placebo (p = 0.001). Given the maximal dosage studied, pregabalin had acceptable tolerability compared to placebo despite a greater incidence of side effects, which were generally mild to moderate in intensity. CONCLUSIONS: Treatment of PHN with pregabalin is safe, efficacious in relieving pain and sleep interference, and associated with greater global improvement than treatment with placebo.
SABATOWSKIR, GALVEZR, CHERRY DA, et al.Pregabalin reduces pain and improves sleep and mood disturbances in patients with post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial[J]. Pain, 2004, 109(1-2): 26-35.
[本文引用:0]
[7]
SEVENTER RV, FEISTER HA, YOUNG JP, et al.Efficacy and tolerability of twice-daily pregabalin for treating pain and related sleep interference in postherpetic neuralgia: a 13-week, randomized trial[J]. Curr Med Res Opin, 2006, 22(2): 375-384.
This trial evaluated the efficacy and safety of pregabalin dosed twice daily (BID) for relief of neuro-pathic pain associated with postherpetic neuralgia (PHN).The 13-week, double-blind, placebo-controlled study randomized 370 patients with PHN to pregabalin (150, 300, or 600 mg/day BID) or placebo.Primary efficacy measure was endpoint mean pain score from daily pain diaries. Secondary efficacy measures included endpoint mean sleep-interference score from daily sleep diaries and Patient Global Impression of Change (PGIC). Safety evaluations included adverse events (AEs), physical and neurologic examinations, 12-lead ECG, vital signs, and laboratory testing.Pregabalin provided significant, dose-proportional pain relief at endpoint: difference from placebo in mean pain score, 150 mg/day, -0.88, p = 0.0077; 300 mg/day, -1.07, p = 0.0016; 600 mg/day, -1.79, p = 0.0003. Weekly mean pain scores significantly improved as early as week 1. Sleep interference in all pregabalin groups was also significantly improved at endpoint, compared with placebo (p < 0.001), beginning at week 1 (p < 0.01). At study termination, patients in the 150 (p = 0.02) and 600 mg/day (p = 0.003) groups were more likely to report global improvement than were those in the placebo group. Most AEs were mild or moderate. Among pregabalin-treated patients, 13.5% withdrew due to AEs, most commonly for dizziness (16 patients, 5.8%), somnolence (8, 2.9%), or ataxia (7, 2.5%).Pregabalin, dosed BID, reduced neuropathic pain associated with PHN and was well tolerated. It also reduced the extent to which pain interfered with sleep. Pregabalin's effects were seen as early as week 1 and were sustained throughout the 13-week study.
STACEY BR, BARRETT JA, WHALENE, et al.Pregabalin for postherpetic neuralgia: placebo-controlled trial of fixed and flexible dosing regimens on allodynia and time to onset of pain relief[J]. J Pain, 2008, 9(11): 1006-1017.
Abstract Unlabelled: Time to onset of pain relief and improvement in allodynia in 269 patients with postherpetic neuralgia was examined in a 4-week randomized trial comparing flexibly dosed pregabalin (150-600 mg/d), fixed-dose pregabalin (300 mg/d), and placebo. For each patient with clinically meaningful pain reduction (>or=30%) at end point, onset of pain relief was defined as the first study day on which a patient reported >or=1-point reduction in pain relative to baseline. Average dose achieved was 396 mg/d in the flexible-dose group compared with 295 mg/d in the fixed-dose group. Median pain relief onset times were 3.5 days (flexible-dose), 1.5 days (fixed-dose), and >4 weeks (placebo). Compared with placebo, significantly more patients in both pregabalin treatment groups achieved >or=30% and >or=50% pain reduction at end point. Almost 95% of patients had brush-evoked allodynia, with 68% having moderate to severe allodynia (>or=40/100 mm). At baseline, pain and allodynia were highly correlated. Independent of treatment assignment, improvement in pain and improvement in allodynia were significantly correlated. Allodynia could serve as a useful surrogate outcome measure in future studies. Pregabalin was significantly better than placebo in alleviating allodynia (flexible-dose reduction, 26 mm; fixed-dose, 21 mm; placebo, 12 mm). Discontinuation rates due to adverse events were more frequent in the fixed-dose group. Perspective: A flexible-dose regimen reduces discontinuations, facilitates higher final doses, and results in a slightly greater pain relief. Allodynia (touch-evoked pain) can be of disabling severity and is present in nearly all patients with postherpetic neuralgia. Allodynia severity is correlated with pain severity and improvement in allodynia is correlated with clinical response.
ACHARA, CHATTERIEEG, RAY TG, et al.Comparative study of clinical efficacy with amitriptyline, pregabalin, and amitriptyline plus pregabalin combination in postherpetic neuralgia[J]. Indian J Dermatol Venereol Leprol, 2010, 76(1): 63-65.
The most common and most intractable sequel of herpes zoster is postherpetic neuralgia (PHN). There is no universally accepted definition of postherpetic neuralgia. The duration of PHN was evaluated by using two definitions: Pain that persisted after healing of rash and pain that persisted for more than 30 days from the time of enrollment. Some authors also described PHN as pain persisting for at least three months after healing of rash. The overall incidence of PHN is 8 to 15%, using the first two definitions. Patients of age 50 years or older had a 14.7-fold higher prevalence of pain, 30 days after onset of rash, than patients younger than 50 years of age. PHN is thought to be due to nerve damage caused by the varicella virus.
ACHARA, CHAKRABORTY PP, BISAIS, et al.Comparative study of clinical efficacy of amitriptyline and pregabalin in postherpetic neuralgia[J]. Acta Dermatovenerol Croat, 2012, 20(2): 89-94.
SUMMARY The most common complication of herpes zoster in immunocompetentpatients is postherpetic neuralgia, which is very difficult to treat. Significantbeneficial effects have been found for amitriptyline, gabapentin, pregabalin,carbamazepine, sodium valproate, oxycodone, corticosteroid, topical capsaicin,tramadol, etc. The aim of this open randomized comparative study was to demonstrateclinical efficacy of amitriptyline and pregabalin. The study included 50patients, 32 (64%) male and 18 (36%) female, randomized to receive either amitriptylineor pregabalin (n=25 each). Amitriptyline was administered in a dose of25 mg once daily and pregabalin in a dose of 75 mg twice daily. Inclusion criteriawere as follows: postherpetic neuralgia of more than 1 month duration; pain ofat least moderate severity; and patient age 40 years or older and no pregnancy.Patients with a history of any serious diseases (renal, cardiac, hepatic or seizure)were excluded. Total treatment period spanned 8 weeks, with patient follow upvisits at 2, 4 and 8 weeks to assess the degree of improvement in pain perceptionand any adverse reaction. Patients with four herpes zoster types were included inthis study, of which thoracic type predominated (54%). Other types were cervicalin 12 (24%), trigeminal in 8 (16%) and lumbosacral in 3 (6%) patients. Prodromalsymptoms before herpes zoster were reported by 66% of study patients. Satisfactoryimprovements of pain perception at the end of 8 weeks (>75%) were noticedin pregabalin group, which was statistically significant (2=10.08; P<0.05).Dry mouth was the commonest complication in amitriptyline group and dizzinessin pregabalin group. More importantly, none of the patients stopped treatmentdue to adverse reaction. In conclusion, therapy with pregabalin is bettercompared to amitriptyline in postherpetic neuralgia patients. However, a similarstudy in a larger sample is required to validate the present findings.
REHMS, BINDERA, BARONR.Post-herpetic neuralgia: 5% lidocaine medicated plaster,pregabalin,or a combination of both? A randomized,open,clinical effectiveness study[J]. Curr Med Res Opin, 2010, 26(7): 1607-1619.
Pregabalin reduces pain and improves sleep and mood disturbances in patients with post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial
2004
Efficacy and tolerability of twice-daily pregabalin for treating pain and related sleep interference in postherpetic neuralgia: a 13-week, randomized trial

 , 肖顺林, 王海雪
, 肖顺林, 王海雪

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}