中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 陆瑶华, 李星霞, 陈燕, 郭澄
, LU Yaohua, LI Xingxia, CHEN Yan, GUO Cheng,
, 陆瑶华, 李星霞, 陈燕, 郭澄
, LU Yaohua, LI Xingxia, CHEN Yan, GUO Cheng,
目的 系统评价使用人血白蛋白与晶体液对成人脓毒症及脓毒症休克患者液体复苏作用的影响。方法 采用计算机检索Cochrane Library、Pubmed、Embase、中国期刊全文数据库(CNKI)、维普中文科技期刊全文数据库(VIP)、万方数据库,检索时间从建库至2015年11月,对符合纳入标准的随机对照试验(RCT)进行质量评价,并采用RevMan5.3版软件进行Meta分析。结果 共纳入4项RCT,合计患者3 862例。人血白蛋白和晶体液对患者28 d死亡率[
Objective To systematically evaluate the effects of albumin compared with crystalloids on fluid resuscitation for adults with severe sepsis and septic shock. Methods The six databases as follows:Cochrane Library,Pubmed,Embase,CNKI,VIP and
1.1.1 纳入研究 纳入的文献研究类型均为随机对照试验(randomized controlled trial,RCT),无论是否采用盲法和分配隐藏,语种限定为中文和英文。
1.1.2 纳入标准 确诊为脓毒症或脓毒症休克的成人患者,年龄>18岁,均符合脓毒症或脓毒症休克的诊断标准[4]。
1.1.3 排除标准 排除以下任意一种情况:①合并急性心肌梗死者;②有原发肝、肾衰竭需替代治疗者;③曾有心搏骤停复苏病史者;④合并急性脑梗死或脑出血者;⑤入院治疗在72 h内死亡者;⑥24 h内紧急手术者;⑦住院期间放弃积极治疗者。剔除资料不完整的文献、相似或相同的重复报道文献,只选用最新报道。
1.1.4 干预措施 试验组以人血白蛋白作为复苏液体;对照组以0.9%氯化钠溶液、平衡液、高渗盐水等作为复苏液体。
1.1.5 结局指标 包括28 d死亡率、90 d死亡率、重症监护室(ICU)住院时间、总住院时间、机械通气时间和肾脏替代治疗。
计算机检索Cochrane Library、PubMed、Embase、中国期刊全文数据库(CNKI)、维普中文科技期刊全文数据库(VIP)、万方数据库,检索时间均从建库至2015年11月,采用“人血白蛋白”“胶体液”“白蛋白”“晶体液”“0.9%氯化钠溶液”“平衡液”“高渗盐水”“脓毒症”“脓毒症休克”“随机”“液体复苏”“colloid”“albumin”“crystalloid”“saline”“hypertonic saline solution”“sepsis”“sepsis shock”“randomized controlled tital”“fluid resuscitation”及其同名异型词等进行检索。
由2名研究人员独立进行文献筛选、数据提取和文献质量评价,并对纳入的信息进行交叉核对,遇分歧通过求助第三方讨论解决。数据提取的内容主要包括:受试人群基线特征及入组例数、干预措施及试验实施情况、文献方法学质量信息、结局指标和测量结果。方法学质量评价依据Cochrane系统评价手册进行。评价项目包括:①随机方法是否正确;②是否做到分配隐藏;③参与者是否采用盲法;④结局评估是否采用盲法;⑤有无失访或退出,如有失访或退出,是否采用意向治疗分析(ITT);⑥是否选择性报道;⑦其他偏倚来源。所有评价项目均满足者,发生偏倚的可能性最低,评为A级;如其中任何一项或多项评价标准仅部分满足或不清楚,则该研究存在相应偏倚的可能性为中等,评为B级;如其中任何一项或多项评价标准完全不满足,则该研究存在相应偏倚的高度可能性,评为C级。
本研究采用RevMan5.3版软件进行Meta分析。采用
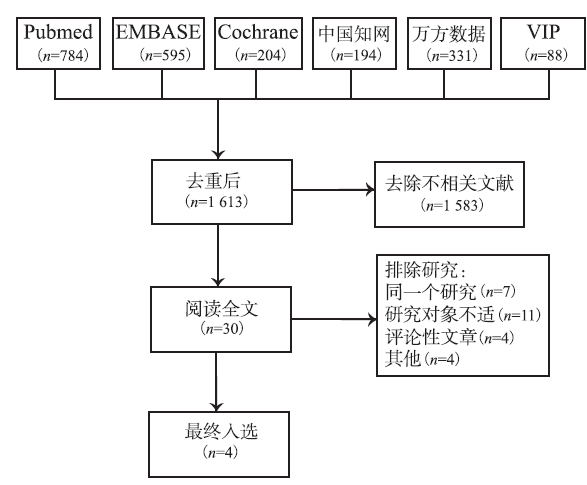
根据既定的检索策略对相应数据库进行检索,共检索得到文献2 196篇,排除重复文献后共计1 613篇。通过阅读文献题目和摘要,排除不相关文献后共计30篇,阅读全文后根据纳入与排除标准,最终纳入4篇RCT文献(
符合纳入标准的4篇文献共3 862例患者,均诊断为脓毒症或脓毒症休克。其中,3项RCT研究方案为人血白蛋白对比0.9%氯化钠溶液,1项RCT研究方案为人血白蛋白对比晶体溶液。干预措施、结局指标、入组人数等评价纳入研究特征,见
表1 纳入Meta分析的4项临床研究特征
Tab.1 Characteristics of the four clinical studies included in meta analysis
依据Cochrane系统评价手册对纳入的4项临床研究进行方法学质量评价,评价项目包括随机方法、分配隐藏、盲法、退出失访、选择性报道,见
表2 纳入Meta分析的4项临床研究质量评价
Tab.2 Quality assessment on the four clinical studies included in meta analysis
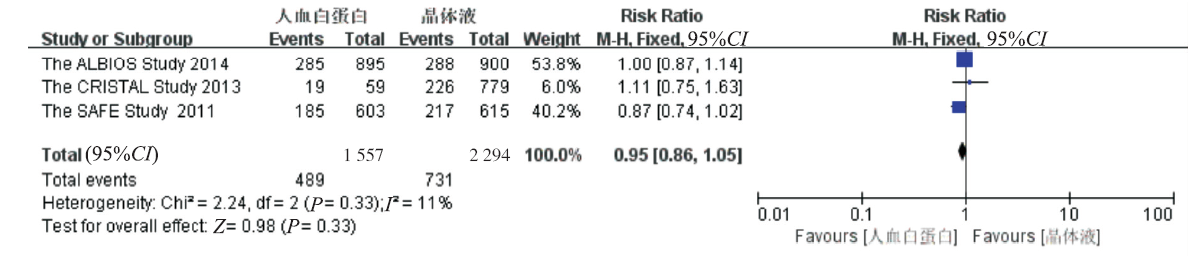
2.3.1 28 d死亡率 3项RCT均报道了28 d死亡率[3,6-7],各研究之间无统计学异质性(
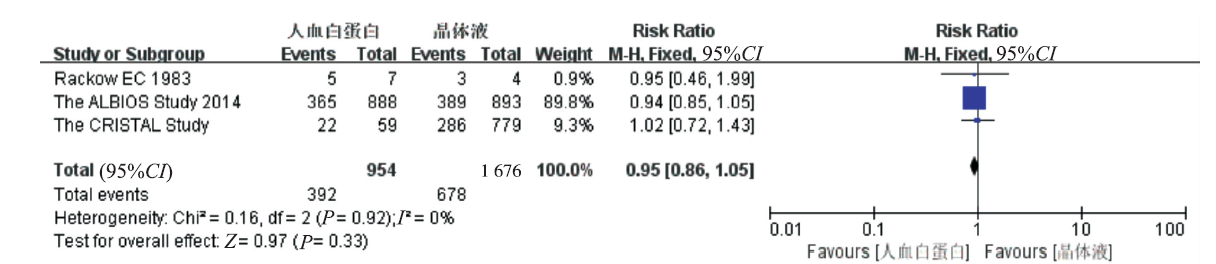
2.3.2 90 d死亡率 3项RCT均报道了90 d死亡率[3,6,8],各研究之间无统计学异质性(
2.3.3 ICU住院天数 2项RCT均报道了ICU住院天数[3,7],各研究之间无统计学异质性(
2.3.4 总住院时间 2项RCT均报道了总住院时间[3,7],各研究之间无统计学异质性(

图5 总住院时间的Meta分析森林图
Fig.5 Forest plot of total duration of hospital stay by meta analysis
2.3.5 机械通气时间 2项RCT报道了机械通气时间[3,7],各研究之间无统计学异质性(

图6 机械通气天数的Meta分析森林图
Fig.6 Forest plot of duration of mechanical ventilation by meta analysis
2.3.6 肾脏替代治疗 ALBIOS研究报道了成人脓毒症及脓毒症休克患者使用两种复苏液体后肾脏替代治疗使用率,白蛋白组为24.6%(222/903),晶体液组为21.4%(194/907),两组差异无统计学意义,
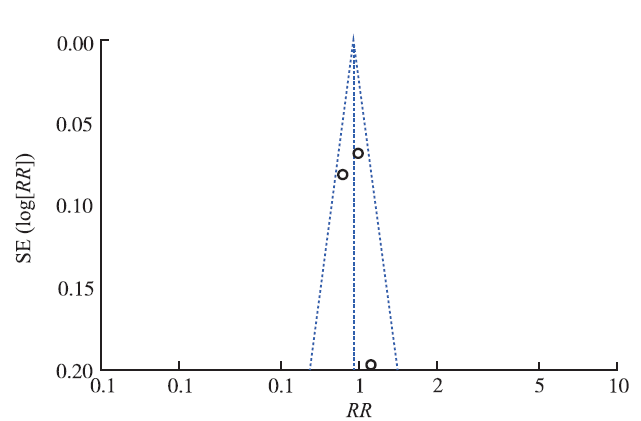
2.3.7 发表偏倚 为全面反映纳入研究的发表偏倚情况,采用28 d死亡率对纳入文献进行倒漏斗图分析,见
早期足够的液体复苏以维持有效的血管容量和组织灌注可明显提高脓毒症及脓毒症休克患者的预后。晶体溶液由于其有效性和廉价易得等优点,经常用于危重患者的液体复苏。晶体溶液由小分子如钠离子、氯离子等组成,大量补充晶体液可能引起高钠血症、高氯血症、酸中毒等不良反应,这对凝血功能、肾功能、胃肠功能和呼吸功能等都有影响[9]。此外,由于其相对分子质量小,晶体溶液可以轻易通过受损的毛细血管半透膜,导致血管内液体扩容持续性降低[10]。而白蛋白的相对分子质量较大,可以更有效保持血管内液体,扩容持续时间久。因此,与晶体溶液相比,白蛋白可以更好地增加胶体渗透压和中心静脉压,降低心率[11]。
本研究评估人血白蛋白和晶体液作为复苏液体对成人脓毒症及脓毒症休克患者的疗效。研究结果表明,人血白蛋白组和晶体液组对患者28 d死亡率、90 d死亡率、ICU住院时间、总住院时间、机械通气时间及肾脏替代治疗等研究指标的影响均差异无统计学意义。表明人血白蛋白和晶体液作为复苏液体,对成人脓毒症及脓毒症休克患者的预后无差异,使用人血白蛋白并无临床获益。此外,采用倒漏斗图方法进行了发表偏倚分析,对称性良好,各研究都落在95%线性范围内,提示文献偏倚较小,可信度较高。
本研究也存在一些局限性,如:①纳入文献数量较少,检索出2 196篇文献,符合条件的仅入选4项研究且均为国外研究,缺少中国人的临床研究数据,建议国内研究单位开展高质量、多中心、大样本的RCT研究;②结局指标方面,有的文献使用均数±标准差描述连续型变量,有的文献使用中位数和四分位数描述,需要经过数据转化才能进行合并分析,因此可能造成偏差。
综上所述,人血白蛋白和晶体液作为复苏液体,对成人脓毒症及脓毒症休克患者的预后无差异。而在关注人血白蛋白和晶体液复苏效果的同时,也应该充分考虑到使用人血白蛋白带来的医疗费用增加和输注血液制品的风险。
The authors have declared that no competing interests exist.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}