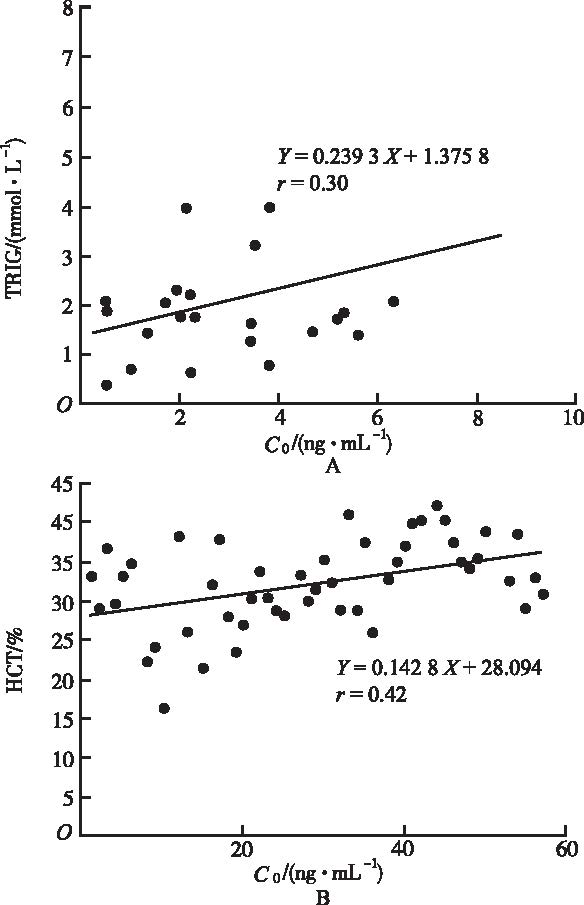
Objective To investigate the efficacy of tacrolimus in treating rheumatic immune disease patients with abnormal blood system,and relationship between tacrolimus concentration and laboratory examination indexes. Methods Basic information of 57 rheumatic immune disease patients with abnormal blood system treated with tacrolimus was collected.Laboratory examination indexes and blood concentration of tacrolimus were analyzed by using STATA. Results The levels of ESR,WBC,HB,PLT and HCT were statistically increased after tacrolimus medication.Additionally,the concentration of tacrolimus was positively related to the levels of TRIG and HCT. Conclusion Tacrolimus can effectively improve the levels of ESR,WBC,HB,PLT and HCT in patients with rheumatic immune disease accompanied with abnormal blood system.While tacrolimus concentration was above 3.1 ng·mL-1,the therapeutic effect was better,without serious adverse reactions.
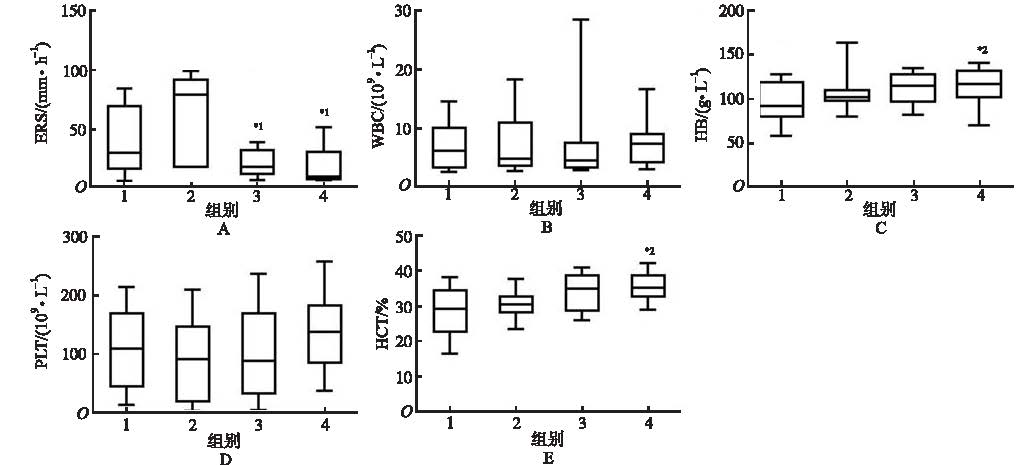
Fig.1
Distribution of ESR(A),WBC(B),HB(C),PLT(D) and HCT(E) in different groups divided by blood drug concentrations Compared with group 2,*1P<0.05;compared with group 1,*2P<0.05
SCHATTNERA,FTIEDMANJ,KLEPFISHA,et al.Immune cytopenias as the presenting finding in primary Sjgren's syndrome[J].Qjm Mon J Assoc Physic,2000,93(12):825-829.
A diagnostic delay of several years in primary Sj02gren's syndrome is common, even in patients who present with sicca symptoms. It is much more likely in cases with prominent symptomatic extraglandular involvement. We report on three such patients who presented as Coomb's positive haemolytic anaemia, systemic symptoms with agranulocytosis and gingival bleeding due to immune thrombocytopenia, to alert clinicians to the fact that primary Sj02gren's syndrome may present as clinically significant immune-mediated cytopenia in the absence of sicca symptoms. Sj02gren's syndrome, a common autoimmune disorder, should be considered in the differential diagnosis of apparently 'idiopathic' cytopenias and actively sought by directed history, Schirmer test and autoantibody screening.
BOROBIA AM,ROMEROI,JIMENEZC,et al.Trough tacrolimus concentrations in the first week after kidney transplantation are related to acute rejection.[J].Ther Drug Monit,2009,31(4):436-442.
There is evidence showing the importance of reaching immunosuppressant target concentrations as soon as possible. The aim of this study was to evaluate the relationship between tacrolimus trough concentrations within the first week after transplantation and the rate of acute rejection. In this descriptive-analytic study, we included 57 renal transplant patients receiving tacrolimus as the primary immunosuppressive drug. After univariate analysis, donor age, duration of hospital stay, and creatinine clearance (third month) showed significant differences between rejecters and nonrejecters. In addition, mean tacrolimus trough concentrations on day 5, day 7, mean of days 1-7, and mean of days 5-7 were found to be significantly lower in rejecters (P = 0.009, P = 0.012, P = 0.006, and P = 0.035, respectively). Receiver operating characteristic curve analysis with tacrolimus trough concentrations measured on days 5 and 7 was able to discriminate between patients with and without acute rejection (P = 0.028 and P = 0.048 after Bonferroni correction). The tacrolimus trough concentration with the best sensitivity-specificity balance was 9.3 ng/mL on day 5 and 8.7 ng/mL on day 7. In the Kaplan-Meier analysis, patients with tacrolimus trough concentrations below 9.3 mg/mL on day 5 showed a lower survival time without acute rejection (P = 0.048 after correction) in comparison with patients with tacrolimus trough concentrations above this concentration. After logistic regression, we obtained a model relating rejection with sex, donor age, and tacrolimus trough concentrations on day 5 (P = 0.004). No significant relationship between tacrolimus trough concentrations and delta creatinine clearance from week 1 to month 3 was obtained. These results confirm that tacrolimus trough concentrations during the first week are an important predictor of acute rejection. Therefore, it is critical to reach target blood concentrations of tacrolimus as soon as possible to improve allograft survival.
DUS,HIRAMATSUN,HAYAKAWAK,et al.Suppression of F-kappaB by cyclosporin a and tacrolimus (FK506) via induction of the C/EBP family:implication for unfolded protein response[J].JI,2009,182(11):7201-7211.
Immunosuppressive agents cyclosporin A (CsA) and tacrolimus (FK506) inhibit cytokine production by activated lymphocytes through interfering with calcineurin. However, little is known about their effects on the function of nonlymphoid cells. We found that, in renal tubular cells, induction of MCP-1 by inflammatory cytokines was blunted by CsA and FK506. This suppression was correlated with induction of unfolded protein response (UPR) evidenced by endogenous and exogenous indicators. The induction of UPR by these agents was reversible and observed generally in other nonimmune cells. Furthermore, administration with CsA in reporter mice caused rapid, systemic induction of UPR in vivo. In TNF-alpha-treated cells, suppression of MCP-1 by CsA or FK506 was associated with blunted responses of NF-kappaB, the crucial regulator of MCP-1. The suppression of NF-kappaB was reproduced by other inducers of UPR including AB(5) subtilase cytotoxin, tunicamycin, thapsigargin, and A23187. CsA and FK506, as well as other UPR inducers, caused up-regulation of C/EBP family members, especially C/EBPbeta and CHOP (C/EBP homologous protein), and overexpression of either C/EBPbeta or CHOP significantly attenuated TNF-alpha-triggered NF-kappaB activation. Furthermore, down-regulation of C/EBPbeta by small interfering RNA substantially reversed the suppressive effect of CsA on TNF-alpha-induced MCP-1 expression. These results suggested that CsA and FK506 confer insensitiveness to TNF-alpha on resident cells through UPR-dependent induction of the C/EBP family members.
STAATZ CE,TETT SE.Clinical Pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation[J].Clin Pharmac,2004,43(10):623-653.
The aim of this review is to analyse critically the recent literature on the clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplant recipients.Dosage and target concentration recommendations for tacrolimus vary from centre to centre, and large pharmacokinetic variability makes it difficult to predict what concentration will be achieved with a particular dose or dosage change. Therapeutic ranges have not been based on statistical approaches. The majority of pharmacokinetic studies have involved intense blood sampling in small homogeneous groups in the immediate post-transplant period. Most have used nonspecific immunoassays and provide little information on pharmacokinetic variability. Demographic investigations seeking correlations between pharmacokinetic parameters and patient factors have generally looked at one covariate at a time and have involved small patient numbers. Factors reported to influence the pharmacokinetics of tacrolimus include the patient group studied, hepatic dysfunction, hepatitis C status, time after transplantation, patient age, donor liver characteristics, recipient race, haematocrit and albumin concentrations, diurnal rhythm, food administration, corticosteroid dosage, diarrhoea and cytochrome P450 (CYP) isoenzyme and P-glycoprotein expression. Population analyses are adding to our understanding of the pharmacokinetics of tacrolimus, but such investigations are still in their infancy. A significant proportion of model variability remains unexplained. Population modelling and Bayesian forecasting may be improved if CYP isoenzymes and/or P-glycoprotein expression could be considered as covariates.Reports have been conflicting as to whether low tacrolimus trough concentrations are related to rejection. Several studies have demonstrated a correlation between high trough concentrations and toxicity, particularly nephrotoxicity. The best predictor of pharmacological effect may be drug concentrations in the transplanted organ itself. Researchers have started to question current reliance on trough measurement during therapeutic drug monitoring, with instances of toxicity and rejection occurring when trough concentrations are within 鈥榓cceptable鈥 ranges. The correlation between blood concentration and drug exposure can be improved by use of non-trough timepoints. However, controversy exists as to whether this will provide any great benefit, given the added complexity in monitoring. Investigators are now attempting to quantify the pharmacological effects of tacrolimus on immune cells through assays that measure in vivo calcineurin inhibition and markers of immunosuppression such as cytokine concentration. To date, no studies have correlated pharmacodynamic marker assay results with immunosuppressive efficacy, as determined by allograft outcome, or investigated the relationship between calcineurin inhibition and drug adverse effects. Little is known about the magnitude of the pharmacodynamic variability of tacrolimus.
SHIMOJIMAY,ISHIIW,MATSUDAM,et al.Coadministration of tacrolimus with corticosteroid accelerates recovery in refractory patients with polymyositis/ dermatomyositis:a retrospective study[J].Bmc Musc Dis,2012,13(1):1-6.
Background In workplace health promotion, all potential resources needs to be taken into consideration, not only factors relating to the absence of injury and the physical health of the workers, but also psychological aspects. A dynamic balance between the resources of the individual employees and the demands of work is an important prerequisite. In the home care services, there is a noticeable trend towards increased psychosocial strain on employees at work. There are a high frequency of work-related musculoskeletal disorders and injuries, and a low prevalence of sustainable work ability. The aim of this research was to identify factors promoting work ability and self-efficacy in care aides and assistant nurses within home care services. Methods This study is based on cross-sectional data collected in a municipality in northern Sweden. Care aides (n = 58) and assistant nurses (n = 79) replied to a self-administered questionnaire (response rate 46%). Hierarchical multiple regression analyses were performed to assess the influence of several independent variables on self-efficacy (model 1) and work ability (model 2) for care aides and assistant nurses separately. Results Perceptions of personal safety, self-efficacy and musculoskeletal wellbeing contributed to work ability for assistant nurses (R 2 adj of 0.36, p < 0.001), while for care aides, the safety climate, seniority and age contributed to work ability (R 2 adj of 0.29, p = 0.001). Self-efficacy was associated with the safety climate and the physical demands of the job in both professions (R 2 adj of 0.24, p = 0.003 for care aides), and also by sex and age for the assistant nurses (R 2 adj of 0.31, p < 0.001). Conclusions The intermediate factors contributed differently to work ability in the two professions. Self-efficacy, personal safety and musculoskeletal wellbeing were important for the assistant nurses, while the work ability of the care aides was associated with the safety climate, but also with the non-changeable factors age and seniority. All these factors are important to acknowledge in practice and in further research. Proactive workplace interventions need to focus on potentially modifiable factors such as self-efficacy, safety climate, physical job demands and musculoskeletal wellbeing.
ASAMIYAY,UCHIDAK,OTSUBOS,et al.Clinical assessment of tacrolimus therapy in lupus nephritis:one-year follow-up study in a single center[J].Neph Clin Pract,2009,113(4):330-336.
KAWAIS,YAMAMOTOK.Safety of tacrolimus,an immunosuppressive agent,in the treatment of rheumatoid arthritis in elderly patients[J].Rheumatology,2006,45(4):441-444.
To prospectively evaluate the safety of tacrolimus in active rheumatoid arthritis (RA) in elderly patients with insufficient response to disease-modifying antirheumatic drugs (DMARDs). Fifty-seven patients aged > or =65 yr with RA for > or =6 months were enrolled in an open-label, non-controlled study. All DMARDs were discontinued and tacrolimus was administered orally once daily after the evening meal for 28 weeks. Tacrolimus, initiated at 1.5 mg/day, was increased to 3 mg/day after 6 weeks if no abnormal changes developed. Existing NSAID and oral corticosteroid (< or =7.5 mg/day prednisolone equivalent) therapy could be continued during the study. Safety was evaluated as clinical symptoms, abnormal changes in laboratory values and the development of infection. Treatment response was determined using the American College of Rheumatology (ACR) criteria for improvement. Whole blood concentrations of tacrolimus 12 h after administration were measured by high-performance liquid chromatography and tandem mass spectrometry. Clinical adverse events developed in 25 patients (46.3%). Abnormal changes in laboratory values occurred in 25 patients (46.3%). Ten patients (18.5%) developed infection. An ACR20 response was achieved by 50.0% of efficacy-evaluable patients and ACR20 success rates (the proportion of patients achieving ACR20 response and completing the study) was 46.3%. The ACR50 response rate was 18.5% of evaluable patients. Mean blood concentration of tacrolimus was 3.3 and 5.3 ng/ml in patients receiving 1.5 and 3.0 mg daily, respectively. No relationship between its concentration and adverse reactions was observed. In elderly patients with insufficient response to DMARD therapy, tacrolimus at 1.5-3.0 mg/day is safe and well-tolerated and provides clinical benefit.
LI HY,LIB,WEI YG,et al.Higher tacrolimus blood concentration is related to hyperlipidemia in living donor liver transplantation recipients[J].Dig Dis Sci,2012,57(1):204-209.
The arrival of tacrolimus has drastically improved AALDLT recipients' survival. However, little data of tacrolimus have been reported concerning its effects on lipid metabolism for AALDLT recipients.Out aim was to investigate the relationship between tacrolimus blood concentration and lipid metabolism in AALDLT recipients.The pre and postoperative data of 77 adult patients receiving AALDLT between 2002 and December 2007 were retrospectively reviewed. The postoperative immune suppressive regimen was prednisone with tacrolimus ± mycophenolate mofetil. Prednisone was withdrawn within the first postoperative month. Blood lipids and tacrolimus concentration were detected at the first, third, and sixth month during follow-up. Episodes of acute rejection were diagnosed based on biopsy.Overall prevalence of post-transplantation hyperlipidemia was 29.9% (23/77) at the sixth postoperative month. The patients were divided into two groups, the hyperlipidemia group and the ortholipidemia group. In the 23 patients with hyperlipidemia, 15 (65%) were hypercholesterolemia, five (22%) were hypertriglyceridemia, and three (13%) patients had both hypercholesterolemia and hypertriglyceridemia. In univariate analysis, only tacrolimus blood concentration at the third and sixth post-transplantation months showed significant difference (8.7 ± 2.1 vs. 6.9 ± 3.2, p = 0.013; 9.2 ± 2.7 vs. 7.3 ± 3.8, p = 0.038, respectively). In multivariate logistic analysis, only two factors appear to be risk factors, namely, tacrolimus blood concentration at the third and sixth post-transplantation months (8.7 ± 2.1 vs. 6.9 ± 3.2, p = 0.043; 9.2 ± 2.7 vs. 7.3 ± 3.8 p = 0.035, respectively).Higher tacrolimus blood concentration was related to hyperlipidemia at an early postoperative period. This indicates that tacrolimus blood concentration should be controlled as low as possible in the premise that there is no risk of rejection to minimize post-transplant hyperlipidemia after AALDLT.
Coadministration of tacrolimus with corticosteroid accelerates recovery in refractory patients with polymyositis/ dermatomyositis:a retrospective study

 , 姚瑶
, 姚瑶
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}