中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 郑丽, 戴晖, 杨爱华
, ZHENG Li, DAI Hui, YANG Aihua,
, 郑丽, 戴晖, 杨爱华
, ZHENG Li, DAI Hui, YANG Aihua,
目的 系统评价二甲双胍对妊娠期糖尿病(GDM)患者新生儿安全性的影响。方法 计算机检索PubMed数据库、CENTRAL数据库、EMBASE数据库、中国期刊全文数据库(CNKI)、万方数据库、中国生物医学文献数据库(CBM)。收集从建库至2016年7月关于二甲双胍在GDM治疗中对新生儿安全性影响的随机对照临床试验(RCTs)。按纳入及排除标准筛选文献,采用Cochrane系统评价员手册5.1.0版的偏倚风险评估工具评价纳入研究的文献质量。采用RevMan5.3版软件进行荟萃分析。结果 最终纳入11篇RCTs,共2056例患者。与单用胰岛素对照组比较,二甲双胍治疗组(单用或合用胰岛素)可以有效降低新生儿低血糖发生率[
Objective To evaluate the effects of metformin on safety of newborn of woman with gestational diabetes mellitus (GDM) treated with metformin. Methods MEDLINE,CENTRAL,EMBASE,CNKI,WANG FANG DATA and CBM were retrieved. Randomized controlled trials (RCTs) that enrolled women with GDM treated with metformin were included. According to the inclusion and exclusion criteria,the quality of the extracted literature were evaluated by the Cochrane Risk of Bias assessment tool of Interventions5.1.0. The included studies were evaluated and analyzed by Meta-analysis with RevMan 5.3. Results Totally,11 RCTs enrolled 2056 pregnant women with GDM. The results of meta-analysis showed that Metformin significantly lowered the risk of neonatal hypoglycemia [
妊娠期糖尿病(gestational diabetes mellitus,GDM)是指妊娠期间首次发生或诊断为糖耐量异常[1]。
GDM与多种妊娠并发症和新生儿不良结局相关[2]。GDM患者若血糖得不到较好控制,则其新生儿发生巨大儿、大于胎龄儿(large for gestational age,LGA)、小于胎龄儿(small for gestational age,SGA)、新生儿低血糖发生率及围产期病死率更高[3,4,5,6],子代患成人心血管疾病的风险增加[7,8,9]。为减少以上并发症,有效控制血糖水平是关键,治疗手段包括:饮食控制、运动疗法和药物治疗[10,11,12]。胰岛素能有效控制血糖水平且不透过胎盘组织,常作为GDM的首选药物[13,14,15],但服用不方便、依从性差,需根据患者体质量指数(BMI)、胰岛素水平等调整剂量,且增加妊娠期低血糖、增加孕期体质量风险[16,17]。口服降糖药二甲双胍日益成为替代胰岛素治疗GDM的有效药物[18,19]。英国国家优化卫生与保健研究所在GDM临床指南中推荐使用二甲双胍作为口服降糖药物[20],美国妇产科医师协会在新的GDM临床管理指南中推荐使用格列本脲和二甲双胍作为替代胰岛素治疗药物[21]。但二甲双胍可通过胎盘,脐带动脉血药浓度水平是母体静脉水平的2倍[22],胎儿暴露于二甲双胍的中长期影响是未知的。已有系统评价分析了二甲双胍在GDM治疗中对母婴结局指标的影响[23,24,25],但他们的研究结论不一致,尤其是缺少对子代长期随访数据的分析。近2年来,新增了多个二甲双胍治疗GDM的随机、对照临床研究[26,27],尤其是3个长期随访研究的报道[28,29,30],为进一步客观评价二甲双胍对GDM患者新生儿安全性的影响,笔者对已有随机、对照临床研究进行系统评价,以期为二甲双胍治疗GDM的安全性提供循证依据。
计算机检索PUBMED、CENTRAL、EMBASE数据库,检索时间均为建库至2016年7月,均采用主题词与自由词相结合的方式检索,语言限定为英文。英文使用检索词包括“metformin”“Diabetes,Gestational”“Gestational Diabetes Mellitus”“Gestational Diabetes”。
1.2.1 研究对象 临床诊断为GDM患者。
1.2.2 研究类型 ①随机对照试验;②文种限英文;③对同一课题组不同时期的结果报告,采用最新发表的研究。
1.2.3 干预措施 ①对照组:仅使用胰岛素治疗;②治疗组:单独二甲双胍治疗或对照组基础上加用二甲双胍治疗。
1.2.4 结局指标 新生儿低血糖发生率,出生体质量,巨大儿发生率,LGA发生率,SGA发生率,早产率,新生儿呼吸窘迫综合征(neonatal respiratory distress syndrome,NRDS)发生率,高胆红素血症发生率,肩难产发生率,新生儿重症监护室(NICU)入住率,围产期病死率,新生儿畸形率。
①非随机对照试验;②妊娠前已诊断为糖尿病患者,合并多囊卵巢综合征患者;③对照组不是接受胰岛素治疗;④无相关新生儿结局指标;⑤动物实验;⑥重复发表、质量差、报道信息过少的研究及短篇报告。
采用Cochrane协作网提供的RevMan5.3版软件进行统计学分析,计数资料采用相对危险度(
2.1.1 文献检索结果 初检出282篇文献,阅读文章题名和摘要及查重后余35篇供进一步筛选。通过对全文的阅读,根据纳入与排除标准,9篇因研究类型不符而排除,6篇因研究对象为2型糖尿病患者被排除,5篇无相关结局指标被排除,4篇因对照组不符或无对照组被排除。最终纳入11篇研究[26-27,31-39]。
2.1.2 纳入研究的基本特征及质量评价 在纳入的11篇文献中,二甲双胍治疗组(单用或合用胰岛素)1024例,单用胰岛素对照组1032例。其中来自伊朗3项研究,芬兰、巴基斯坦各2项研究,美国、巴西与埃及各1项研究,新西兰与澳大利亚1项。所有研究均报告了新生儿结局指标,纳入文献的详细特征见
表1 纳入文献的基本特征
Tab.1 Basic characteristics of the included studies
表2 GDM诊断标准和纳入标准
Tab.2 Criteria for diagnosis and inclusion of GDM
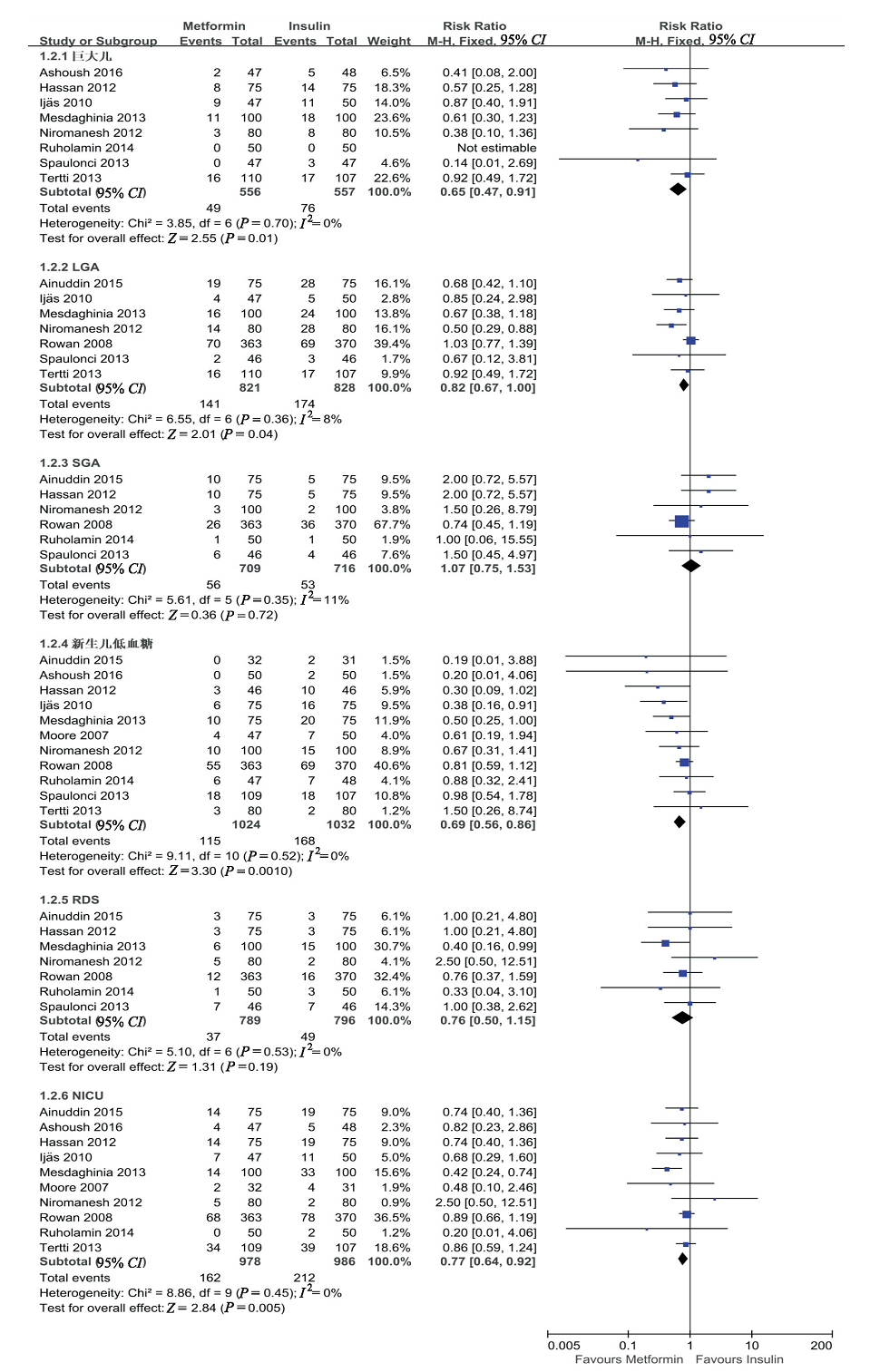
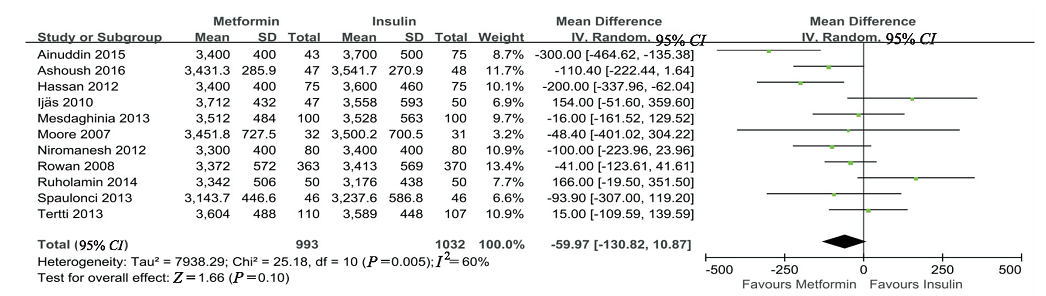
新生儿主要结局指标包括新生儿低血糖发生率,出生体质量,巨大儿发生率,LGA发生率,SGA发生率,新生儿呼吸窘迫综合征发生率,NICU入住率。除出生体质量外,其余指标均采用固定效应模型分析。纳入研究均报告了新生儿低血糖发生率与出生体质量情况,汇总结果显示与单用胰岛素比较,二甲双胍可以显著降低新生儿低血糖发生率[
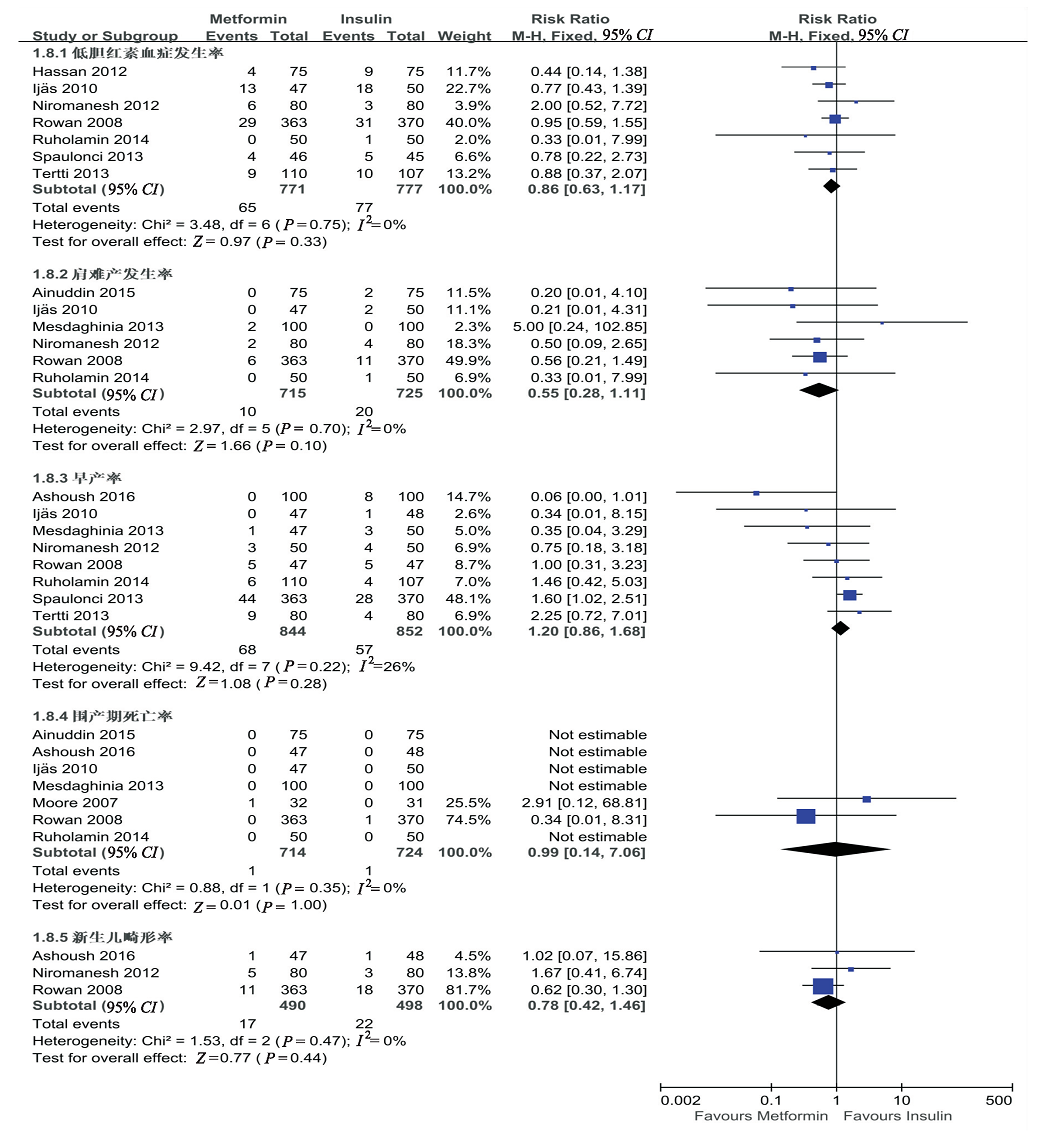
新生儿次要结局指标包括低胆红素血症发生率、早产率、肩难产发生率、围产期病死率、新生儿畸形率。所有指标均采用固定效应模型分析。汇总结果显示,高胆红素血症发生率[
所有纳入研究均报告了新生儿低血糖发生率,以其为研究指标将固定效应模型换成随机效应模型计算合并效应量,再进行Meta分析,所得合并效应量RR值分别为0.564,95%
汇总结果显示,与单用胰岛素对照组比较,二甲双胍治疗组可以显著降低新生儿低血糖发生率(
与单用胰岛素对照组比较,二甲双胍治疗组可有效降低新生儿低血糖、巨大儿、LGA、NICU不良妊娠结局发生率,未增加SGA、NRDS、高胆红素血症、肩难产、围产期死亡、新生儿畸形等不良反应结局发生率。二甲双胍可能是替代胰岛素治疗GDM的一种有效、安全口服药物。但目前中国相关指南中并未推荐任何口服药物应用于GDM的治疗,本文纳入的研究都来自于国外,得出的结果是否能应用于中国人群,尚需高质量、大样本的临床研究验证。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
The insulin receptor, an integral membrane glycoprotein, is synthesized as a single-chain precursor that is cleaved to produce two mature subunits, both of which contain N-linked oligosaccharide chains and covalently linked fatty acids. We report that the beta-subunit also contains O-linked oligosaccharides. The proreceptor, alpha-subunit, and beta-subunit were labeled with [3H]mannose and [3H]galactose in the presence or absence of an inhibitor of O-linked glycosylation. Tryptic peptides from each component were separated by reverse-phase high-performance liquid chromatography. N- and O-linked oligosaccharide chains were identified on these peptides by specific enzymatic digestions. The proreceptor and alpha-subunit contained only N-linked oligosaccharides, whereas the beta-subunit contained both N- and O-linked oligosaccharides. The O-linked oligosaccharide chains were attached to a single tryptic fraction of the beta-subunit, which also contained N-linked chains. This fraction was further localized to the NH2-terminal tryptic peptide of the beta-subunit by specific immunoprecipitation with an anti-peptide antibody with specificity for this region. Binding of insulin and autophosphorylation of the beta-subunit were not dependent on O-linked glycosylation, because cells grown in the presence of the inhibitor exhibited a normal dose response to insulin. Therefore, the insulin receptor contains O-linked oligosaccharides on the NH2-terminal tryptic peptide of the beta-subunit, and these O-linked oligosaccharides are not necessary to the binding or autophosphorylation function of the receptor.
[本文引用:1]
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
Gestational diabetes mellitus (GDM) is defined as glucose intolerance, first time detected in pregnancy. Diagnostic criteria for GDM have changed over the decades. The aim of the study was to examine the effect of diet on birth weight, number of large for gestational age (LGA) (birth weight > 90th percentile) babies, total maternal weight gain, gestational age and route of delivery among patients with positive 50 g glucose challenge test (GCT) and negative 100 g oral glucose tolerance test (OGTT).A prospective randomized controlled study was conducted among patients with positive 50 g GCT and negative 100 g OGTT. A plasma glucose value of 140 mg/dL was used as the threshold to define an abnormal GCT result. In group 1 50 patients were given a caloric diet and compared with group 2 with 50 patients without a given diet. Patients were followed up until delivery and evaluated for birth weight, number of LGA babies, total maternal weight gain, gestational age and route of delivery.There were no significant differences between the groups in maternal age, parity, body mass index and gestational age at delivery. There were significant differences in birth weight, number of LGA babies, total maternal weight gain during pregnancy. The mean gestational age at delivery was 38.7卤1.2 weeks in group 1 and 38.9卤1.1 weeks in group 2 (p = 0.615). The mean birth weight in group 1 was 3328卤399 g and 3623卤485 g in group 2 (p = 0.007), cesarean rate was 32% in group 1 and 40% in group 2 (p = 0.405).In the management of patients with positive 50 g GCT and negative 100 g OGTT, patients who were prescribed medical nutrition therapy by a dietitian experienced in GDM management had better perinatal outcomes.
[本文引用:1]
|
| [11] |
|
| [12] |
The incidence of gestational diabetes mellitus (GDM) is increasing in the United States. Universal GDM screening is recommended, although evidence of benefit is lacking. Treatment of GDM reduces the risk of shoulder dystocia, preeclampsia, and macrosomia. Intensive treatment is more effective than less-intensive treatment. Traditional management includes diet, exercise, and short- and intermediate-acting insulin regimens. Use of metformin and glyburide is controversial, but evidence supporting safety and efficacy is accumulating. Postpartum screening with a glucose tolerance test rather than a fasting blood glucose level should be performed 6 weeks after delivery.
[本文引用:1]
|
| [13] |
With the increase in obesity and sedentary lifestyles, the incidence of diabetes among reproductive-aged women is rising globally. Providers are expected to care for a growing number of women with gestational diabetes (GDM) in the coming decades. Traditionally, insulin has been considered the standard for management of GDM, when diet and exercise fail to achieve tight maternal glucose control without the risk of transfer of insulin across the placenta. Understanding the effectiveness and safety of the use of oral diabetes agents during pregnancy for both maternal and neonatal outcomes as an alternative management option is essential to the care of women with GDM and their offspring. In this review, our objectives were to (1) summarise the available evidence on the efficacy these medications, (2) review available data on adverse effect, (3) discuss current gaps in research, outlining limitations in current study designs that deserve attention and (4) summarise key points for the practicing clinician.
[本文引用:1]
|
| [14] |
Abstract Gestational diabetes (GD) develops because pregnancy increases requirements for insulin secretion while increasing insulin resistance. Women with GD often have impaired pancreatic beta-cell compensation for insulin resistance. The nature of GD is currently contentious, with debate about its existence, diagnosis and ramifications for both mother and offspring from pregnancy into later life. Also contentious are the outcomes of intervention with diet, insulin, glyburide (Glynase trade mark, Pharmacia Upjohn) and metformin (Glucophage trade mark, Bristol-Myers Squibb). There is consensus that women with unequivocal GD have a significant risk of adverse perinatal outcomes and increased risk of later type 2 diabetes mellitus. Foetuses from pregnancies with GD have a higher risk of macrosomia (associated with higher rate of birth injuries), asphyxia, and neonatal hypoglycaemia and hyperinsulinaemia. Uncontrolled GD predisposes foetuses to accelerated, excessive fat accumulation, insulin resistance, pancreatic exhaustion secondary to prenatal hyperglycaemia and possible higher risk of child and adult obesity and type 2 diabetes mellitus later in adult life. However, there is no consensus as to whether glucose intolerance of a severity below unequivocal GD is related to adverse maternal, fetal or perinatal outcomes, and whether this relationship is a continuous one. If dietary intervention is not sufficient in the treatment of GD, then, historically, insulin has been added. Recent studies suggest that glyburide may be efficaciously substituted for insulin. Preliminary studies suggest that metformin may have the unique potential to prevent the development of GD.
[本文引用:1]
|
| [15] |
|
| [16] |
Purpose of reviewThe use of insulin sensitizing drugs such as metformin in polycystic ovary syndrome has been increasingly popular and validated by systematic reviews. There has also been an interest in the use of metformin for gestational diabetes. However, administration of metformin to prevent miscarriage is controversial and widespread use of this drug in early pregnancy requires investigation.Recent findingsThere are claims that miscarriage and gestational diabetes are more common in polycystic ovary syndrome and that use of insulin sensitizers improves outcomes dramatically. This review suggests there is no evidence for increased risk of miscarriage solely due to polycystic ovary syndrome and that there are insufficient data for promoting therapy with metformin. There is some reason for use of metformin in mid-pregnancy for gestational diabetes but better evidence from randomized controlled trials is urgently needed.SummaryThe use of metformin in early pregnancy for reducing the risk of miscarriage should be avoided outside of the context of properly designed prospective randomized trials. Safety in early pregnancy appears to be reassuring but not completely proven. The use of metformin in mid-pregnancy for gestational diabetes appears more logical but also needs adequate trials before general use is advocated.
[本文引用:1]
|
| [17] |
The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study of over 23 000 diabetes-free pregnancies has shown that at a population level an unequivocal linear relationship exists between maternal glucose concentrations around the beginning of the third trimester of pregnancy and the risk of their baby being born above the ninetieth centile for weight. With the rising incidence of gestational diabetes (GDM) across the developed world, largely paralleling the increased prevalence of obesity, there has been a sharp increase in the risk of pregnancy complications developing related to the birth of macrosomic babies. The associated additional long-term complications of GDM pregnancies means that in the future there is likely to be a large increase in the incidence of type 2 diabetes and associated conditions in both the mothers and their affected offspring. The present review seeks to highlight recent advances and remaining gaps in knowledge about GDM in terms of its genetics (where some of the recently discovered polymorphic risk factors for type 2 diabetes have also proved to be risk factors for GDM) and its treatment by diet, exercise and drugs.
[本文引用:1]
|
| [18] |
Numerous studies have established a direct relationship between maternal levels of glycemic control and neonatal outcomes for pregnancies complicated by diabetes. The past several years have seen the addition of insulin analogues as well as many new oral agents to the pharmacological armamentarium available to treat diabetes. Insulin analogs (both rapid and long acting) are of potential interest for women with insulin-requiring diabetes because of the improved control reported in non-pregnant individuals. Insulin lispro is the only insulin analog to be systematically studied in pregnancy. At this time, the majority of evidence suggests that insulin lispro does not cross the placenta and does not have adverse maternal or fetal effects during pregnancy in women with diabetes.
[本文引用:1]
|
| [19] |
The negative impact of the gestational diabetes on the maternal and fetal health is well known and this impact is closely related to gestational age at which the diagnosis is done. Therefore, the use of therapeutic options able to prevent or delay the gestational diabetes occurrence has a positive impact on maternal and neonatal outcomes.Physical activity and dietary advice represent the first choice and they are the most studied as well. They represent a non-pharmacological option and have a positive impact on insulin resistance although they do not seem to prevent the gestational diabetes onset.The preconceptional use of metformin in women with polycystic ovary syndrome protects the pancreatic beta cell reserve preventing or delaying the occurrence of gestational diabetes. However, there are also doubts on the drug safety in pregnancy since it completely crosses the placenta.From this point of view, the inositol could represent an excellent alternative.Its role as insulin sensitizing agent is well documented on improving both the hormonal and reproductive parameters. However, the studies on its preconceptional use in preventing gestational diabetes are too limited though the first results are extremely encouraging.
[本文引用:1]
|
| [20] |
|
| [21] |
|
| [22] |
Metformin passes the placenta. Fetal serum levels are comparable with maternal values.
[本文引用:2]
|
| [23] |
|
| [24] |
DOI:10.1136/bmj.h102
URL
[本文引用:3]
|
| [25] |
To assess the efficacy of metformin and insulin in the treatment of pregnant women with gestational diabetes mellitus (GDM). A meta-analysis was conducted by including randomized controlled trials comparing metformin and insulin in GDM. An electronic search was conducted to identify relevant studies. Data were synthesized by a random effects meta-analysis model. A Bayesian analysis was also performed to account for uncertainties in the treatment efficacy. Eight clinical trials involving 1712 individuals were included in the final analysis. The pooled estimates of metformin–insulin differences were very small and statistically non-significant in fasting plasma glucose, postprandial plasma glucose and HbA1c, measured at 36–37 weeks of gestation. Notably, 14–46% of those receiving metformin required additional insulin. Compared with the insulin group, metformin treatment was associated with a lower incidence of neonatal hypoglycemia (relative risk, RR 0.74; 95% CI 0.58–0.93;P=0.01) and of neonatal intensive care admission (RR 0.76; 95% CI 0.59–0.97;P=0.03). Bayesian analysis revealed that the efficacy of metformin was consistently higher than insulin with a probability of over 98% on these two neonatal complications. Other outcomes were not significantly different between the two treatment groups. In women with gestational diabetes, metformin use and insulin therapy have comparable glycemic control profile, but metformin use was associated with lower risk of neonatal hypoglycemia.
[本文引用:4]
|
| [26] |
|
| [27] |
|
| [28] |
DOI:10.2337/dc11-0660
URL
[本文引用:3]
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
Objective: To assess the clinical efficacy of Metformin in the prevention of fetal macrosomia and neonatal morbidity in gestational diabetes pregnancies compared with insulin treatment. Methodology: In this interventional study, randomized clinical trial a total of 150 patients with gestational diabetes between 20-35 weeks of gestation were selected for pharmacological treatment using metformin or insulin during the study period form 20-Dec-2008 till 20-Dec-2010 from Antenatal OPD after screaning with 75 grams OGTT. The primary outcomes were fetal macrosomia and neonatal morbidity. Results: Patients on metformin and insulin were matched in age, parity, BMI and gestational age at study entry. Mean birth weight did not differ in both groups but fetal macrosomia was less in metformin group than in insulin group 18.67% V/S 10.65% P Conclusion: Metformin is a safe and effective alternative to insulin in gestational diabetes. Metformin treatment resulted in less fetal macrosomia and fewer NICU admissions and neonatal morbidity with advantages of cheap oral therapy in our resource poor setting.
[本文引用:4]
|
| [37] |
We reviewed recent data on the prevalence, risk factors, complications, and management of trauma during pregnancy. Using the terms “trauma” and “pregnancy” along with specified mechanisms of injury, we queried the PubMed database for studies reported from Jan. 1, 1990, through May 1, 2012. Studies with the largest number of patients for a given injury type and that were population-based and/or prospective were included. Case reports and case series were used only when more robust studies were lacking. A total of 1164 abstracts were reviewed and 225 met criteria for inclusion. Domestic violence/intimate partner violence and motor vehicle crashes are the predominant causes of reported trauma during pregnancy. Management of trauma during pregnancy is dictated by its severity and should be initially geared toward maternal stabilization. Minor trauma can often be safely evaluated with simple diagnostic modalities. Pregnancy should not lead to underdiagnosis or undertreatment of trauma due to unfounded fears of fetal effects. More studies are required to elucidate the safest and most cost-effective strategies for the management of trauma in pregnancy.
[本文引用:4]
|
| [38] |
|
| [39] |
DOI:10.1111/dom.12017
URL
[本文引用:7]
|
| [40] |
DOI:10.2337/dc16-S015
URL
[本文引用:1]
|
| [41] |
|
| [42] |
|
| [43] |
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}