中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

编者按 呼吸系统疾病是严重危害人民健康的常见病、多发病,给社会和国民经济带来沉重负担,同时还伴随着临床不合理用药问题。雾化吸入疗法是呼吸系统相关疾病的重要治疗手段之一,因其临床应用优势被国内外广泛使用。在我国,很多基层医院,甚至大型综合医院由于医务人员对雾化吸入疗法及其药物应用认识不足,临床应用中存在许多不合理用药现象。在这种形式下加强雾化吸入药物的规范管理与合理使用尤为重要!
基于此,由中华医学会临床药学分会和中国药理学会发起,中华医学会临床药学分会合理用药学组组织了“2018年度全国医药学术交流会暨临床药学与药学服务研究进展培训班——雾化吸入疗法合理用药专家研讨会”,正式启动“雾化吸入疗法合理用药专家共识”撰写项目(简称“共识”)。会议由中国药理学会主办、《医药导报》编辑部承办,2018年6月23日在山东省临沂市召开。本次会议确定了编写专家组成员,并对“共识”大纲进行专业细致的研讨。2018年7月10日在湖北省武汉市确定“共识”大纲内容。2018年11月3日在湖北省武汉市召开“中华医学会临床药学分会第三届委员会第二次全体委员会议”上进行“共识”中期审稿,委员及学组专家对“共识”初稿内容进行逐条修订,并提出近50条专业修改建议,对“共识”内容的准确性与药学特色进行了严格的把关。经过多次专家审稿和修订, 2018年12月8日在河南省郑州市召开“中华医学会临床药学分会第三届委员会第三次全体委员会议”,对“共识”的内容进行最后修订,得到编委会专家组的一致认可而最终定稿。
本“共识”在中华医学会临床药学分会、中国药理学会、中华医学会临床药学分会合理用药学组专家,以及游一中教授为代表的专家顾问组共同努力下完成编写,旨在提高我国雾化吸入疗法合理用药水平,造福广大患者!
雾化吸入是一种以呼吸道和肺为靶器官的直接给药方法,具有起效快、局部药物浓度高、用药量少、应用方便及全身不良反应少等优点,已作为呼吸系统相关疾病重要的治疗手段。但雾化吸入疗法的不规范使用不仅会直接影响治疗效果,更可能带来安全隐患,威胁患者生命健康。为进一步促进雾化吸入药物在临床的合理应用,维护患者健康,中华医学会临床药学分会携手全国药学领域知名专家,结合我国医疗卫生实践,制定出符合我国国情的雾化吸入疗法合理用药专家共识。本共识可以为各级医疗机构医务工作者开展规范的雾化吸入治疗提供参考。
雾化吸入装置是一种将药物转变为气溶胶形态,并经口腔(或鼻腔)吸入的药物输送装置[1]。小容量雾化器是目前临床最为常用的雾化吸入装置,其储液容量一般小于10 mL。根据发生装置特点及原理不同,目前临床常用雾化器可分为射流雾化器(jet nebulizers)、超声雾化器(ultrasonic nebulizers)和振动筛孔雾化器(mesh nebulizers)3种。
射流雾化器适用于下呼吸道病变或感染、气道分泌物较多,尤其伴有小气道痉挛倾向、有低氧血症严重气促患者。气管插管患者常选用射流雾化器雾化吸入支气管舒张剂治疗支气管痉挛,然而气管插管可影响气溶胶进入下呼吸道,若欲达到相同的疗效,一般需要较大的药物剂量[2]。
振动筛孔雾化器是通过压电陶瓷片的高频振动,使药液穿过细小的筛孔而产生药雾的装置,减少超声振动液体产热对药物的影响。筛孔的直径可决定产生药雾颗粒的大小。振动筛孔雾化器雾化效率较高且残留药量较少(0.1~0.5 mL),并具有噪音小、小巧轻便等优点。与射流雾化器和超声雾化器比较,震动筛孔雾化器的储药罐可位于呼吸管路上方,方便增加药物剂量。
2.1.1 雾化吸入疗法的特点及作用机制 雾化吸入疗法是应用雾化吸入装置,使药液形成粒径0.01~10 μm的气溶胶微粒,被吸入并沉积于气道和肺部,发挥治疗作用。雾化颗粒直径对药物沉积位置有直接影响,有效雾化颗粒直径应在0.5~10 μm。其中粒径5~10 μm的雾粒主要沉积于口咽部,粒径3~<5 μm的雾粒主要沉积于肺部,粒径<3 μm的雾粒50%~60%沉积于肺泡。
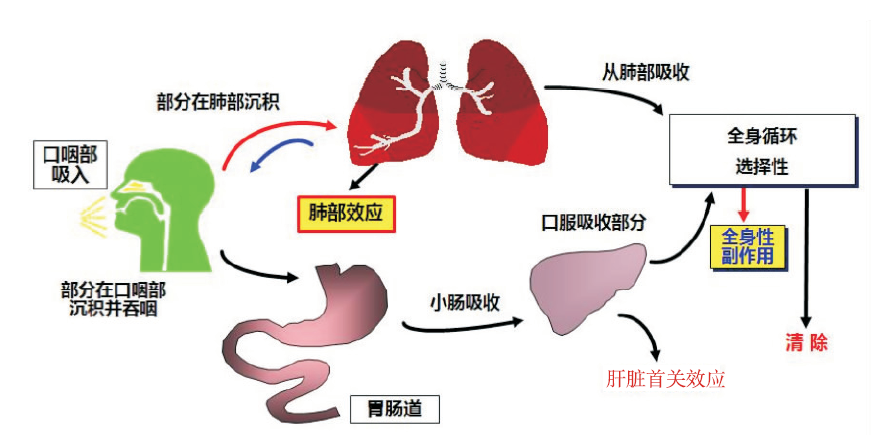
2.1.2 雾化吸入药物的理化特性 药物经雾化吸入后可产生局部及全身作用,理想的雾化吸入药物主要在肺部和气道产生作用,而作用于全身的副反应少,在理化特性上具有“两短一长”的特点,即在气道黏膜表面停留时间短、血浆半衰期短和局部组织滞留时间长。
临床常用雾化吸入药物主要有吸入性糖皮质激素(inhaled corticosteroid,ICS)、短效 β2受体激动剂(short-acting beta 2 receptor agonists, SABA),短效胆碱M受体拮抗剂(short-acting muscarinic antagonist,SAMA)和黏液溶解剂等几大类。
2.1.3 雾化吸入药物配伍与常用雾化联合方案 《Trissel 混合组分的稳定性》和Trissel的两个临床药剂学数据库提供国内外多种雾化吸入药物的配伍数据,包括各种药物在同一雾化器中配伍使用的相容性和稳定性数据(
表1 常用雾化吸入药物的配伍
表2 常用雾化联合方案
2.1.4 非雾化吸入制剂不推荐用于雾化吸入治疗 非雾化吸入制剂用于雾化吸入治疗属于超说明书用药,临床比较普遍,但存在较大的安全隐患,故不推荐以下使用。①不推荐以静脉制剂替代雾化吸入制剂使用。静脉制剂中常含有酚、亚硝酸盐等防腐剂,吸入后可诱发哮喘发作。而且非雾化吸入制剂的药物无法达到有效雾化颗粒要求,无法经呼吸道清除,可能沉积在肺部,从而增加肺部感染的发生率。如盐酸氨溴索注射液,国内尚无雾化吸入剂型。②不推荐传统“呼三联”方案(地塞米松、庆大霉素、α-糜蛋白酶)。“呼三联”药物无相应雾化吸入制剂,无充分安全性证据,且剂量、疗程及疗效均无统一规范。③不推荐雾化吸入中成药。中成药因无雾化吸入制剂,所含成分较多,安全性有效性证据不足。④因无雾化吸入剂型而不推荐使用的其他药物还包括:抗病毒药物、干扰素[2]、低分子肝素[8,9]、氟尿嘧啶、顺铂、羟喜树碱、生物反应调节剂(如白细胞介素-2、贝伐单抗)[10,11]等。
2.2.1 ICS ①药理作用机制。糖皮质激素(glucocorticoids,GS)抗炎作用基本机制可分为经典途径(基因途径)和非经典途径(非基因途径)[12,13]。经典途径指GS易通过细胞膜进入细胞,与细胞质内糖皮质激素受体(glucocorticoid receptor,GR)结合形成活化的GS-GR复合物,进入细胞核内启动基因转录,引起转录增加或C:有临床研究确证特定混合物的稳定性和相容性;*1C:来自生产厂家的报告确证特定混合物的稳定性和相容性,在许多情况下,这些例子不适用于综述,通过包装内的说明或与厂家直接沟通确认;X:有证据确认或建议,特定混合物不能配伍;NI:评价配伍稳定性证据不充分,除非将来有证据证明可行;CD:配伍稳定性数据有争议减少,改变介质相关蛋白的水平,对炎症反应所必需的细胞和分子产生影响而发挥抗炎作用。经典途径属于延迟反应,一般需要数小时起效。非基因途径是GS直接作用于细胞膜膜受体,数分钟起效。膜受体的数量仅占受体总量的10%~25%,且解离常数远高于细胞质受体的解离常数。因此,需要大剂量ICS才能启动非经典途径。
②药学特性。理想的ICS应包括以下几个特点:空气动力学粒径<5 μm,口服生物利用度低,受体亲和力高,肺内滞留时间长,蛋白结合率高,系统清除快等。
ICS体内过程:ICS吸入后,部分经气道在肺部沉积而发挥肺部的抗炎效应,而其他大部分沉积在口咽部。ICS生物利用度(systemic bioavailability)是经气道吸收入血(肺生物利用度)和经肠道吸收入血(口服生物利用度)的总和[14],具体代谢过程见
颗粒粒径:吸入药物在肺内的分布取决于空气动力学粒径,其影响因素包括物理粒径、晶型、外形、密度等。一般体外测定为物理粒径,如电镜下,丙酸倍氯米松、丙酸氟替卡松均为长约10 μm的针状微粒,布地奈德为粒径2.0~3.0 μm球状颗粒可能更适合肺内分布[15]。
受体亲和力与抗炎活性:气道上皮细胞和支气管血管细胞均有丰富的GR[16]。ICS与肺部GR结合产生有益效应,与肺外GR结合则常产生有害效应。不同ICS(活性成分)的受体亲和力不同(
表3 常用ICS药效学和药动学特点
亲脂性、酯化作用和分布容积:ICS肺滞留时间延长可增强肺局部抗炎作用,与本身亲脂性和酯化作用相关[17]。 目前临床常用的ICS均具有相对较高的亲脂性,亲脂性高的ICS易穿过靶细胞膜,与细胞质内GR结合。亲脂性过高可导致分布容积增大,不利于ICS在水/酯相间组织转运,使半衰期延长而增加体内药物蓄积风险,因此要求ICS有适度亲脂性和亲水性。具有酯化作用的药物可在气道组织与脂类物质可逆性结合,形成长链脂肪酸复合物贮存于细胞质中,相当于在靶组织中提供ICS的缓释储库,使其肺滞留时间延长[14,18]。
前体药物:前体药物是指在体外活性较小或者无活性的化合物,进入体内经酶催化或者非酶作用,迅速释放出活性物质而发挥药理作用的化合物[19]。丙酸倍氯米松为前体药物,在体内催化酶作用下水解为活性代谢物17-单丙酸倍氯米松。但这种催化酶在人体许多组织,如肝脏、结肠、胃、乳腺和脑组织也有表达[20]。因此,在肺外组织中活化、且与受体高亲和力的17-单丙酸倍氯米松潜在的全身不良反应风险需要警惕。
表4 常见雾化吸入ICS和支气管舒张剂的临床应用及推荐给药方案
2.2.2 SABA ①作用机制。SABA通过兴奋气道平滑肌和肥大细胞膜表面的β2受体,活化腺苷酸环化酶(AC),增加细胞内环磷酸腺苷(cAMP)的合成,舒张气道平滑肌,稳定肥大细胞膜而发挥作用。ICS与SABA联合应用时具有协同作用,ICS可上调β2受体表达,减少因β2受体下调导致的β激动剂耐受性,而SABA可促进糖皮质激素受体易位,增加其抗炎作用。②药学特性。特布他林雾化溶液经吸入后,在数分钟内起效,1.0 h达到峰值,疗效持续4~6 h,主要用于缓解症状,按需使用。沙丁胺醇数分钟内起效,1.0~1.5 h达到峰值,疗效持续3~6 h[37]。③国内常用雾化吸入用SABA的临床应用及推荐用法。目前中国已上市的SABA有特布他林和沙丁胺醇,临床应用和推荐剂量可参见
2.2.3 SAMA ①作用机制。SAMA通过与内源性胆碱竞争靶细胞上的毒蕈碱受体(M受体)而发挥作用。M受体有5个亚型,但呼吸道内只有M1 、M2和M3有明确的生理活性[38]。SAMA拮抗M1及M3受体可舒张支气管平滑肌并抑制黏液高分泌状态,拮抗M2受体则促使神经末梢释放乙酰胆碱,使支气管收缩,因此部分削弱了拮抗M1和M3受体所带来的支气管舒张作用。②药学特性。M3受体主要存在于大气道,支气管收缩的作用最强,故SAMA对大气道的舒张作用强于对周围气道的作用。一般在15 min内起效,1~2 h达峰值[39],持续4~6 h。与SABA比较,SAMA起效时间较慢,但持续时间较长。③国内常用雾化吸入SAMA的临床应用及推荐用法。国内上市的SAMA雾化制剂仅有异丙托溴铵及其复方制剂。SAMA一般与SABA联合应用,常用于COPD和支气管哮喘急性发作时的起始治疗。复方异丙托溴铵含异丙托溴铵0.5 mg 和硫酸沙丁胺醇3.0 mg。适用于需要多种支气管扩张剂联合应用的成人和>12岁青少年,如治疗气道阻塞性疾病有关的可逆性支气管痉挛[40]。由于该制剂本身为复方制剂,尚缺乏本品与其他药物配伍的研究,说明书指出不需要把本品与其他药物混合在同一雾化器中使用。
临床应用和推荐剂量可参见
由于抗感染药物的雾化吸入剂型尚未在我国上市,临床应用抗感染药物注射剂型用作雾化吸入较为普遍,而其疗效及安全性缺乏充分的循证医学证据。非雾化吸入剂型抗感染药物雾化可引起多种不良反应,如呼吸机麻痹、变态反应、肌无力、神经肌肉接头阻断反应等。此外,注射剂型中抗氧化剂和防腐剂等辅料还可导致患者出现严重的气道痉挛[43]。因此,不推荐非雾化吸入剂型的抗感染药物作雾化使用。
2.2.5 黏液溶解剂 ①作用机制。国内上市的黏液溶解剂雾化吸入制剂仅有乙酰半胱氨酸。其分子结构中含有巯基(-SH)基团,可使黏蛋白分子复合物间的双硫键(-S-S)断裂,从而降低痰液的黏滞性,使液化后容易咳出;还可使脓性痰液的DNA纤维断裂,溶解脓性痰[37]。同时,
目前国内尚无氨溴索雾化制剂,尽管有较多的临床应用静脉制剂进行雾化治疗的经验报道[51,52,53],但氨溴索注射液说明书并无雾化吸入的用法,其雾化吸入的用法用量、配置浓度及疗效、安全性尚需更多临床研究验证[28,53-56]。
雾化吸入治疗不良反应程度与类型各不相同,与患者本身因素、雾化吸入不规范、雾化治疗药物副作用,以及非雾化剂型不合理使用等因素有关,因此需要进行药学监护与用药教育。
3.1.1 常用雾化吸入药物的不良反应及处理 ①ICS。与全身用糖皮质激素比较, ICS的不良反应发生率低,安全性较好。但由于给药方式的特殊性,ICS吸入后沉积在口咽部、喉部可造成局部不良反应,使用后立即漱口和漱喉,可有效减少局部不良反应。长期研究并未显示小剂量雾化吸入布地奈德对儿童生长发育、骨质疏松、下丘脑-垂体-肾上腺轴有明显的抑制作用[65,66,67]。对于需要长期吸入大剂量ICS的患者,应定期检查患者的皮肤、骨骼、代谢等情况[68,69]。ICS常见局部不良反应[70]见
表5 ICS的常见不良反应
②支气管舒张剂。SABA和SAMA常见不良反应见
表6 几种吸入性支气管舒张剂的常见不良反应
以上常见不良反应均来源于相关产品说明书在应用β2受体激动剂或胆碱M受体拮抗剂雾化吸入治疗时应加强观察对于出现不良反应的患者可考虑暂停雾化吸入治疗,并观察心率、脉搏等指标,严重者及时就医处理[73]。
③乙酰半胱氨酸。对鼻咽和胃肠道有刺激,可出现鼻液溢、胃肠道刺激,如:口腔炎、恶心和呕吐的情况[74]。对于胃溃疡或有胃溃疡病史的患者,尤其是当与其他对胃黏膜有刺激作用的药物合用时,慎用本品[74]。患有支气管哮喘的患者,在治疗期间应密切观察病情,如有支气管痉挛发生,应立即终止治疗。
3.1.2 雾化吸入治疗相关不良事件及处理 ①雾化器及装置相关不良事件。戴面罩进行雾化吸入治疗时,药物可能会沉积在眼部,刺激眼球,如发生应立即用清水清洗,并换用咬嘴[2]。气溶胶温度过低、输送的气溶胶密度过高、雾化溶液pH值不当、低渗及高渗气溶胶或可导致哮喘或其他呼吸系统疾病患者发生支气管痉挛[75],应立即停止雾化吸入,并予以相应治疗措施。②患者相关不良事件。雾化吸入治疗根据其吸入药物的不同,可出现口腔干燥症、龋齿、口腔黏膜改变、溃疡、牙龈炎、牙周炎、味觉障碍等多种口腔疾病,通常与患者个人卫生习惯和治疗期间未注重口腔护理有关[76]。如出现上述口腔问题,应积极就医,加强口腔护理。对于长期治疗患者应定期进行口腔检查。
3.1.3 对特殊人群加强用药监护
①老年患者:老年患者在使用雾化吸入制剂时,一方面提高其用药依从性和准确性,另一方面需确保其用药的安全性。ICS:老年人群用药时肺炎发生风险受到广泛关注,不同的ICS肺炎风险之间可能存在差异[77]。支气管扩张剂:患有心脏病(如心律失常、冠心病等)的老年患者,雾化吸入SABA时,应严格掌握按需吸入的原则,吸入次数过多或吸入剂量过大易引起心律失常或冠心病症状加重;前列腺增生或膀胱癌颈部梗阻的老年患者应慎用SAMA。
②儿童患者:布地奈德混悬液是目前美国食品药品管理局(FDA)批准的唯一可用于4岁以下儿童的ICS雾化剂型[5,78],是我国2018年版《国家基本药物目录》中唯一推荐用于平喘的ICS雾化剂型。也是世界卫生组织(WHO)儿童基药目录(适用于12 岁以下儿童)中唯一推荐用于治疗哮喘的ICS[79]。SABA是治疗任何年龄儿童喘息发作的首选药物[35]。
儿童雾化吸入时应根据需要进行剂量调整,尽可能使用口罩吸入(年幼者应使用面罩吸入器),优先选择密闭式面罩。且最好在安静状态下进行雾化吸入治疗。治疗过程中,应密切观察生命体征,如出现频繁咳嗽、气促、气道痉挛等症状时,应立即暂停雾化治疗进行观察,待缓解后评估是否适合继续治疗[5,28,35]。对于需长期雾化治疗的儿童,应定期随访评估疗效,家长切不可自认孩子有好转就自行停药[5]。
③孕期及哺乳期妇女。NAEPP专家组和ACOG发布的临床指南都指出,对于有持续性哮喘的妊娠期及哺乳期妇女,ICS是控制气道炎症的首选药物[80,81]。布地奈德的FDA妊娠分级为B级,丙酸倍氯米松和丙酸氟替卡松为C级。瑞典出生登记中心研究显示,布地奈德治疗对先天畸形、胎儿死亡、孕龄及胎儿生长均无显著性影响[82]。推荐妊娠期及哺乳期妇女首选布地奈德。
美国儿科学会(American Academy of Pediatrics,AAP)声明[83],特布他林很少经母乳排泄,可作为哺乳期妇女优先选用的SABA。
3.2.1 药物贮藏 应按说明书要求贮存。使用前应仔细检查药品,确保药品在有效期内,颜色性状均正常。
3.2.2 药物配置 碱性药液、高渗盐水及纯化水可引起气道高反应性,应避免用于雾化吸入。油性制剂可能引起脂质性肺炎,不能用于雾化吸入。雾化吸入制剂应在开瓶后立即使用。部分药物不能在同一容器中混合使用,应严格遵医嘱用药。
3.2.3 雾化吸入治疗前 雾化吸入治疗前1 h不应进食,清洁口腔分泌物和食物残渣,以防雾化过程中气流刺激引起呕吐;洗脸、不抹油性面膏,以免药物吸附在皮肤上。对于婴幼儿和儿童,为保持平静呼吸宜在安静或睡眠状态下治疗,前30 min内不应进食。
3.2.4 雾化吸入治疗中 ①按医嘱将药液配置好放入雾化吸入器内,如采用氧气驱动雾化,应调整好氧流量至6~8 L·min-1,观察出雾情况,注意勿将药液溅入眼内。②采用舒适的坐位或半卧位,用嘴深吸气、鼻呼气方式进行深呼吸,使药液充分达到支气管和肺部。③密切关注患者雾化吸入治疗中潜在的药物不良反应。出现急剧频繁咳嗽及喘息加重,如是雾化吸入过快或过猛导致,应放缓雾化吸入的速度;出现震颤、肌肉痉挛等不适,不必恐慌,及时停药,如为SABA类药物,如特布他林引起,一般停药后即可恢复,后随访告知医生;出现呼吸急促、感到困倦或突然胸痛,应停止治疗并立即就医。
3.2.5 雾化吸入治疗后 ①使用面罩者嘱其及时洗脸,或用湿毛巾抹干净口鼻部以下的雾珠,以防残留雾滴刺激口鼻皮肤引起皮肤过敏或受损。婴幼儿面部皮肤薄,血管丰富,残留药液更易被吸收,需及时洗漱。②年幼儿童可用棉球蘸水擦拭口腔后,再适量喂水,特别是使用激素类药物后,以减少口咽部的激素沉积,减少真菌感染等不良反应的发生。③及时翻身拍背有助于使粘附于气管、支气管壁上的痰液脱落,保持呼吸道通畅。
3.2.6 雾化吸入装置 雾化吸入装置应该专人专用,避免交叉污染。每次使用后需进行清洁并干燥存放,以防受到污染后成为感染源,影响治疗。
《雾化吸入疗法合理用药专家共识》编写组
编写组长:杜光 赵杰
审核专家成员名单(按姓氏拼音排序)
巴桑拉姆 西藏自治区人民医院
曹力 南昌大学第一附属医院
陈万生 上海第二军医大学
陈孝 中山大学附属第一医院
陈英 广西壮族自治区人民医院
董亚琳 西安交通大学医学院第一附属医院
杜光 华中科技大学同济医学院附属同济医院
杜智敏 哈尔滨医科大学附属第二医院
方晴霞 浙江省人民医院
冯婉玉 中国医科大学第一附属医院
高申 海军军医大学附属长海医院
葛卫红 南京大学医学院附属鼓楼医院
龚志成 中南大学湘雅医院
郭代红 中国人民解放军总医院
郭瑞臣 山东大学齐鲁医院
侯锐钢 山西医科大学第二医院
胡欣 卫计委北京医院
黄红谦 海南医学院附属医院
黄品芳 福建医科大学附属第一医院
菅凌燕 中国医科大学附属盛京医院
姜玲 安徽省立医院
阚全程 郑州大学第一附属医院
李焕德 中南大学湘雅二医院
李丽 海南医学院第一附属医院
李雪松 昆明医学院第一附属医院云大医院
刘皋林 上海市第一人民医院
刘景丰 福建医科大学孟超肝胆医院
刘丽宏 首都医科大学附属北京朝阳医院
刘世霆 南方医科大学南方医院
刘小玲 内蒙古自治区人民医院
刘玉梅 吉林大学中日联谊医院
卢海儒 青海省人民医院
吕迁洲 复旦大学附属中山医院
马瑞莲 内蒙古医学院附属医院
梅丹 中国医学科学院北京协和医院
缪丽燕 苏州大学附属第一医院
齐晓勇 河北省人民医院
邱峰 重庆医科大学附属第一医院
沈承武 山东省立医院
师少军 华中科技大学同济医学院协和医院
宋金春 武汉大学人民医院、湖北省人民医院
隋忠国 青岛大学附属医院
孙洲亮 厦门大学附属第一医院
童荣生 四川省医学科学院·四川省人民医院
王春革 天津市第一中心医院
王建华 新疆医科大学第一附属医院
文爱东 第四军医大学西京医院
文友民 宁夏医科大学总医院
武新安 兰州大学第一附属医院
夏培元 第三军医大学第一附属医院
胥婕 北京大学第三医院
杨宏昕 内蒙古自治区人民医院
杨婉花 上海交通大学医学院附属瑞金医院
于倩 吉林大学中日联谊医院
张健 上海交通大学医学院附属新华医院
张鉴 山东省立医院
张抗怀 西安交通大学第二附属医院西北医院
张抒扬 北京协和医院
张伟 河南省人民医院
张文婷 华中科技大学同济医学院附属同济医院
张相林 卫生部中日友好医院
张晓坚 郑州大学第一附属医院
张幸国 浙江大学医学院附属第一医院
张永军 石河子大学医学院第一附属医院
张玉 华中科技大学同济医学院附属协和医院
张志清 河北医科大学第二医院
张志仁 哈尔滨医科大学附属肿瘤医院
赵杰 郑州大学第一附属医院
赵庆春 沈阳军区总医院
赵志刚 首都医科大学附属天坛医院
郑志昌 贵阳医学院附属医院
左笑丛 中南大学湘雅三医院
《雾化吸入疗法合理用药专家共识》执笔专家成员名单(按姓氏拼音排序)
卜书红 上海交通大学医学院附属新华医院
陈娜 浙江大学医学院附属第一医院
陈瑞玲 首都医科大学附属天坛医院
陈万生 海军军医大学长征医院
陈孝 中山大学附属第一医院
陈泳伍 安徽省立医院
戴智勇 中南大学湘雅医院
杜光 华中科技大学同济医学院附属同济医院
冯瑾 海军军医大学长征医院
高杰 苏州大学附属第一医院
高申 海军军医大学附属长海医院
葛卫红 南京大学医学院附属鼓楼医院
郭瑞臣 山东大学齐鲁医院
菅凌燕 中国医科大学附属盛京医院
姜玲 安徽省立医院
李峰 郑州大学第一附属医院
李佳 中山大学附属第一医院
李玉平 上海肺科医院
刘皋林 上海市第一人民医院
卢晓阳 浙江大学医学院附属第一医院
吕迁州 复旦大学附属中山医院
闵光宁 兰州大学第一医院
缪丽燕 苏州大学附属第一医院
沈承武 山东省立医院
隋忠国 青岛大学附属医院
童荣生 四川省医学科学院·四川省人民医院
王春革 天津市第一中心医院
王卓 海军军医大学附属长海医院
武新安 兰州大学第一附属医院
徐珽 四川大学华西医院
叶晓芬 复旦大学附属中山医院
尹桃 中南大学湘雅医院
游一中 常州市第一人民医院
张健 上海交通大学医学院附属新华医院
张玮 上海肺科医院
张文婷 华中科技大学同济医学院附属同济医院
张晓坚 郑州大学第一附属医院
赵杰 郑州大学第一附属医院
赵志刚 首都医科大学附属天坛医院
朱立勤 天津市第一中心医院
邹东娜 山东省立医院
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
目前的静脉注射用药,无论是在药物选择,还是配伍方面都有一定的安全用药参考信息,可供临床医师、药剂师和护士参考。然而,关于雾化吸入治疗的用药方案以及药物配伍的信息却非常有限。近期美国发表的常用雾化吸入药物混合配伍指南采用了易于使用的表格形式,为临床提供了可供雾化吸入的药物及其配伍的各种参考信息。我们在该指南基础上,结合中国呼吸道疾病雾化吸入治疗现状,制定了儿童雾化吸入治疗共识,根据不同疾病提出了雾化治疗推荐方案,供临床医师参考。
[本文引用:3]
|
| [3] |
|
| [4] |
Astra Draco AB, Lund, SUEDE
[本文引用:1]
|
| [5] |
吸入型糖皮质激素(inhaled corticosteroids,Ics)是治疗气道急、慢性炎症的常用药物。ICS不同剂型的药物,如压力定量气雾剂、干粉剂和雾化吸入混悬液,在临床应用中均显示出良好的疗效,其中雾化吸人糖皮质激素以其可靠疗效、良好安全性和易操作性,在我国儿科临床获得了广泛应用,尤其是在年幼儿童,包括各级医疗机构以及家庭;不仅用于支气管哮喘的长期控制和急性发作,也用于其他呼吸系统疾病。
[本文引用:5]
|
| [6] |
|
| [7] |
\0
[本文引用:1]
|
| [8] |
Although heparin and low-molecular-weight heparins (LMWH) have been widely used clinically as anticoagulants, their broader use has been limited by the lack of noninvasive delivery methods for this class of molecules. In this study, we demonstrate an efficient, rapid, and reproducible delivery system for heparin through the lungs that is not confined to particles of a certain geometric or aerodynamic diameter. Importantly, blood levels after intrapulmonary administration of either heparin or LMWH were comparable to that of s.c. administration but are characterized by a more rapid onset of action (t(1/2) = 40 min vs. 2.5 h, respectively). Furthermore, we show in animal models, that inhaled heparin species efficiently inhibit diseases such as thrombosis and emphysema, and that the repetitive inhalation of formulated LMWH results in no observable toxicity from the delivery of reproducible systemic levels of heparin or LMWH.
[本文引用:1]
|
| [9] |
目的探讨低分子肝素钙雾化吸入对慢性肺源性心脏病(肺心病)的治疗效果。方法 90例肺心病患者随机分为治疗组与对照组,对照组给予常规治疗,治疗组在常规治疗的基础上应用低分子肝素钙雾化吸入,100IU/kg,q12h,疗程7 天。治疗前后监测动脉血气分析、血凝及纤溶指标,治疗后评估疗效。结果临床疗效治疗组优于对照组(P〈0.05),治疗7天后治疗组血液流变学指标明显改 善,PaO2明显上升,PaCO2明显下降,血液学指标变化不明显。结论低分子肝素钙雾化吸入可明显改善肺心病患者的血液粘稠度和肺通气功能,给药方便, 安全有效。
[本文引用:1]
|
| [10] |
正雾化吸入抗肿瘤药物为肺癌及肺转移瘤的治疗,提供了一种有效、低毒的治疗方法。本文重点介绍了雾化吸入抗肿瘤药物的种类、常见不良反应,以及脂质体药物的进展,对临床推广和规范雾化吸入抗肿瘤药物治疗肺部恶性肿瘤具有重要意义。非小细胞肺癌(non-small cell lung carcinoma,NSCLC)是原发于肺部的高度异质性肿瘤,全球发病率和致死率最高,5年生存率仅15%。尽管随着新的治疗途径和新药物剂型的不断发展,但
[本文引用:1]
|
| [11] |
目的研究雾化吸入抗癌药物治疗肺部肿瘤的临床效果。方法选取我院在2015年3月至2016年2月行雾化吸入抗癌药物治疗的18例肺部肿瘤患者(研究组),与同期行化疗治疗的18例肺部肿瘤患者(对照组),观察比较两组的治疗效果与毒副反应发生情况。结果两组的治疗效果相比较,无统计学意义(P>0.05);而两组的毒副反应发生情况相比较,研究组明显低于对照组,具统计学意义(P<0.05)。结论肺部肿瘤患者采用雾化吸入抗癌药物进行治疗具有良好的临床效果,能够将毒副作用减小,且操作便捷,临床应用价值高。
[本文引用:1]
|
| [12] |
Abstract Inhaled corticosteroids suppress airway inflammation and components of airway remodelling in bronchial asthma. In the tracheobronchial (airway) vasculature, these include the inhibition of inflammatory hyperperfusion, microvascular hyperpermeability, mucosal oedema formation, and the formation of new blood vessels (angiogenesis). Corticosteroids are now known to exert their effects on the airway vasculature through genomic and nongenomic mechanisms. Genomic actions involve the regulation of target genes, and suppress most of the vascular elements of inflammation and angiogenesis in the airway. In contrast, nongenomic actions are mediated by rapid cellular mechanisms, and induce transient vasoconstriction in the airway, thereby reversing inflammatory hyperperfusion. The vascular actions of corticosteroids contribute to controlling clinical symptoms of asthma primarily by influencing airway calibre in the lung periphery and airway hyperreactivity. In this review article, recent advances into the understanding of cellular mechanisms and the clinical implications of the interaction of inhaled corticosteroids and the airway vasculature in asthma are reviewed.
[本文引用:1]
|
| [13] |
Glucocorticoids act via genomic and non-genomic actions. The genomic glucocorticoid actions are well known and new details on processes of transactivation and transrepression have been reported recently. Here we describe the current knowledge on non-genomic glucocorticoid actions and discuss why these actions are considered to be of therapeutic relevance. It is assumed that rapid non-genomic glucocorticoid effects are mediated by three different mechanisms: (1) physicochemical interactions with cellular membranes (non-specific non-genomic effects); (2) membrane-bound glucocorticoid receptor (mGCR)-mediated non-genomic effects; and (3) cytosolic glucocorticoid receptor (cGCR)-mediated non-genomic effects. With regard to the first mechanism, we discuss here lazaroids and the novel development of drug targeting with liposomes as the carrier system for glucocorticoids. The clinical use of the latter two mechanisms is still speculative, but intriguing ideas are being discussed in this regard.
[本文引用:1]
|
| [14] |
|
| [15] |
This study compared the in vitro performance of two inhaled corticosteroid products for nebulisation, Pulmicort Respules03 (budesonide 0.5mg/mL) and Clenil03 per Aerosol (beclomethasone dipropionate (BDP) 0.4mg/mL). Each product was used in combination with three different nebulisers (2mL/test, 5min run time) and the dose to the lungs was determined according to standard methods. The shape of the suspended particles in each product was studied using scanning electron microscopy (SEM). Overall, a higher fine particle dose was achieved with Pulmicort Respules03 versus Clenil03 per Aerosol, with estimated dose to the lungs of 8–14 and 3–6% of nominal dose, respectively. SEM showed that budesonide particles were small, typically 652–3μm in diameter, whereas those of BDP were needle-shaped and up to 6510μm long. The more favourable particle shape and size of suspended budesonide may explain the higher fine particle dose with Pulmicort Respules03 versus Clenil03 per Aerosol.
[本文引用:1]
|
| [16] |
The localization and distribution of the human glucocorticoid receptor (GR) mRNA and protein was investigated in human lung obtained from transplant donors and recipients by in situ hybridization, RNA blot analysis, immunolocalization, and Western analysis. Subjects were either nonasthmatic or had mild asthma requiring only beta(2)-agonists. No difference in amount of GR mRNA was found in total RNA isolated from nonasthmatic or asthmatic donor lung. In situ hybridization showed the highest concentration of GR mRNA in the alveolar walls and vascular endothelium and smooth muscle, with lesser amounts in the airway epithelium and smooth muscle. There was no change in the level or sites of expression of GR mRNA between normal and asthmatic subjects. Immunolocalization of GR confirmed the in situ hybridization data. There was no change in the level or sites of expression of GR, in either the lung or airway, between normal and asthmatic subjects. Immunolocalization of GR in bronchial biopsies from two normal and asthmatic subjects confirmed the localization and distribution of GR. Western analysis and mobility shift assays confirmed no differences in GR levels between the two subject groups. The localization of GR mRNA and protein to specific cell types within lung and airway will make it possible to study the cellular targets of glucocorticoid therapy in inflammatory lung diseases such as asthma.
[本文引用:1]
|
| [17] |
Elsevier’s Scopus, the largest abstract and citation database of peer-reviewed literature. Search and access research from the science, technology, medicine, social sciences and arts and humanities fields.
[本文引用:1]
|
| [18] |
ABSTRACT Microsomes from human lung and liver catalyze the formation of fatty acid esters of budesonide, a glucocorticoid used for inhalation treatment of asthma. The conjugation was dependent on coenzyme A and ATP. Addition of free fatty acids to the incubations affected the pattern of metabolites, but ester formation was observed also without such addition. Budesonide oleate, palmitate, linoleate, palmitoleate, and arachidonate were identified as metabolites. The fatty acid conjugates of budesonide were shown to be substrates for lipase in vitro, thus budesonide is regainable from the conjugates. The data suggest that an equilibrium between budesonide and these pharmacologically inactive lipoidal conjugates will be established in tissues at repeated exposure to budesonide. Since the fatty acid conjugates most likely will be retained intracellularly for a longer time than unchanged budesonide, the duration of tissue exposure to budesonide will depend partly on the rate of lipase-catalyzed hydrolysis of the conjugates. The findings in this study provide a possible explanation for the efficacy of budesonide in mild asthmatics also when inhaled once daily.
[本文引用:1]
|
| [19] |
Abstract Bronchial asthma and allergic rhinitis are among the most common diseases of modern society and to an increasing degree a major cause of illness, hospitalization, loss of productivity, and death. Despite improvements in drug therapy over the years, the incidence is still increasing. Inhaled and intranasal corticosteroids are the drugs of choice in the therapy of asthma and allergic rhinitis. Inhalation and intranasal use result in better, target-specific delivery of corticosteroids. Higher concentrations at the site of action and minimized systemic exposure provide improved therapeutic ratios. However, there is still considerable concern over the risk of systemic side effects. It is the goal of inhaled and intranasal corticosteroid therapy to produce long-lasting therapeutic effects at the site of action and minimize systemic side effects with high clearance, low oral bioavailability and high plasma protein binding. This article reviews the pharmacokinetic and pharmacodynamic properties of corticosteroids used in asthma and allergic rhinitis.
[本文引用:1]
|
| [20] |
Abstract An NADPH dependent arylamine carcinogen and fatty acid steroid ester metabolizing esterase activity belonging to the B- or carboxylesterase class of non-specific esterase (EC 3.1.1.1) was measured by two different methods: (i) a spectrophotometric assay using alpha naphthyl acetate (ANA) as substrate and (ii) a radiometric method using the conversion of beclomethasone-17,21-dipropionate to beclomethasone-17-monopropionate as the endpoint. The two methods were strongly correlated when assayed in human mononuclear leukocytes (r = 0.89, P < 0.0001) and human mammary tissue (r = 0.91, P < 0.0001). Hence it was concluded that the two substrates are metabolized at least in part by the same enzyme. This esterase activity was abundant in human monocytes, present in T-lymphocytes and equally divided between CD4 and CD8 T-lymphocyte subsets. The same activity was expressed in human liver, colon, stomach, breast and brain tissues. The distribution of this esterase in human tissues showed high activity in liver, intermediate activity in colon, stomach and breast and low activity in brain tissue. The interorgan distribution observed in human tissues was closely mimicked when the esterase activity was assessed in liver, colon and brain tissues from three mouse strains and three rat strains. The non-specific steroidal esterase activity determined by ANA metabolism in human mammary tissue was shown to be reproducible when assayed as triplicate samples from each of 16 different women (intraclass correlation coefficient 67.3%, P < 0.03). The interindividual variation in mammary tissue was high (18.4-fold) and there was a positive correlation between the esterase activity and age (r = 0.58, P < 0.01), as well as a tendency toward bimodal distribution. To our knowledge, these data represent the first systematic study of interorgan and interspecies comparisons of a non-specific steroidal esterase activity.
[本文引用:2]
|
| [21] |
|
| [22] |
|
| [23] |
Background and objectiveThe efficacy of inhaled corticosteroids (ICS) in asthma exacerbation are yet to be clarified. The aim of this study was to investigate the efficacy of nebulized ICS in children with moderate-to-severe acute exacerbation of asthma in an emergency room setting in order to elucidate the potential use of ICS as the first-line therapy in the management of acute exacerbation of asthma.MethodsThis was a prospective, randomized, double-blind, placebo-controlled study. Paediatric patients with moderate-to-severe acute exacerbation of asthma in emergency room were randomized to receive nebulized salbutamol and ipratropium bromide, with the addition of nebulized high-dose budesonide (BUD group, n090009=09000960) or normal saline (control group, n090009=09000958), three doses in the first hour.ResultsThe improvement in forced expiratory volume in 1090009s was similar in both groups at 0090009h after three doses of nebulization, but there was significantly further improvement at 1 and 2090009h in the BUD group (0.09509000900±0900090.062090009L and 0.10009000900±0900090.120090009L, respectively) compared with the control group (0.05909000900±0900090.082090009L and 0.02109000900±0900090.128090009L, respectively), P090009=0900090.013 and 0.001, respectively. Complete remission rate was significantly higher (84.7% vs 46.3%, P090009=0900090.004) and need for oral corticosteroids was significantly lower (16.9% vs 46.3%, P090009=0900090.011) in BUD group than in control group.ConclusionOn the basis of nebulized short-acting bronchodilators, addition of nebulized high-dose budesonide resulted in clinical improvement in children with moderate-to-severe acute exacerbation of asthma, suggesting that nebulized high-dose ICS can be used as first-line therapy for non-life-threatening acute exacerbation of asthma in children.
[本文引用:0]
|
| [24] |
Background: Since their introduction in the 1970s, inhaled corticosteroids (ICSs) have been used to control airway inflammation associated with asthma. Budesonide is one of the ICSs recommended as first-line therapy for mild to moderate persistent asthma. Objective: This article describes the esterification of budesonide and how it results in prolonged, location-specific retention of drug in the airways, allowing once-daily dosing. Results: Studies conducted over the past decade have shown that budesonide forms reversible fatty acid esters within the cells of airway tissue, resulting in the formation of an intracellular depot pool of inactive drug. As the intracellular concentration of free budesonide decreases, these budesonide esters are hydrolyzed back to their active state. This process increases budesonide's retention in the airways, prolongs its duration of action, and lowers the risk of systemic effects. Conclusions: By extending budesonide's local anti-inflammatory effect and increasing its airway selectivity, the esterification process appears to contribute to the drug's efficacy, particularly during once-daily administration. Reducing the number of required daily inhalations may increase patient compliance with asthma therapy, although this remains to be evaluated.
[本文引用:0]
|
| [25] |
Background: Glucocorticoids (GCs) are the most potent anti-inflammatory agents available for allergic diseases including asthma, which are routinely believed to need several hours to take effect through regulating gene expression. Our previous report had shown that GCs could inhibit allergic asthma within 10 min, which the classical mechanism could not explain. Objective: To confirm the existence and verify the sites of GCs' rapid action, we investigated nongenomic effects of GCs on degranulation of mast cells in allergic asthma. Methods: The GCs' rapid action on airway mast cells deregulations was evaluated in the allergic asthma model of guinea pigs by the computer-assisted morphometry. Using whole-cell patch clamp and fluorometric assay, we examined GCs' nongenomic effect on IgE-mediated exocytosis and histamine release of rat basophilic leukaemia-2H3 mast cells. Employing the flash photolysis technique, we studied the role of Ca 2+ signal in the GCs' nongenomic effect. Results: Inhaled GCs significantly inhibited airway mast cells degranulation in the allergic asthma model of guinea pigs within 10 min. In vitro , GCs could rapidly inhibit IgE-mediated exocytosis and histamine release of mast cells, and neither GC nuclear receptor antagonist nor protein synthesis inhibitor could block the rapid action. We further demonstrated that GCs' nongenomic effect was not through direct action on secretory machinery, but was mediated by a reduction in the [Ca 2+ ] i elevation. Conclusions: The study suggested for the first time that nongenomic pathway was involved in GCs' rapid inhibition on allergic asthma, and raised the possibility of new therapeutic strategies for allergic diseases including asthma.
[本文引用:0]
|
| [26] |
Abstract BACKGROUND: In patients with asthma, single doses of inhaled glucocorticosteroids (ICS) have been reported to have antiinflammatory actions that can be detected several hours after drug administration. However, the onset and duration of the effect have not been investigated. We therefore measured airway blood flow ([Formula: see text]aw) as an index of airway inflammation to determine the time course and dose dependence of the antiinflammatory action of an ICS in 20 patients with moderate asthma receiving regular ICS treatment. METHODS: [Formula: see text]aw and spirometry were measured before and serially for 360 minutes after a single inhaled dose of 360 g, 720 g, and 1,440 g budesonide or placebo as well as after four repetitive 720-g budesonide doses given 30 minutes apart. RESULTS: Baseline mean [Formula: see text]aw was increased and FEV1 was decreased without significant differences among the 5 treatment days. After budesonide inhalation, there was a transient, dose-dependent decrease in mean [Formula: see text]aw from 12 to 21%, with significant differences from baseline at 60 and 90 minutes for the 720-g and 1,440-g doses (P < 0.05). Thirty minutes after four repetitive budesonide administrations, mean [Formula: see text]aw was 28% below baseline (P < 0.05) and remained 11% below baseline after 270 minutes. There was no change in mean FEV1 after any of the treatments. CONCLUSIONS: In subjects with moderate asthma who use ICS regularly, inhaled budesonide caused a transient dose-dependent vasoconstriction in the airway, thereby reversing one manifestation of airway inflammation. These results suggest that a pure controller medication can have immediate beneficial effects not paralleled by changes in airflow. Clinical trial registered with www.clinicaltrials.gov ( NCT 01219738 ).
[本文引用:0]
|
| [27] |
This study was conducted to investigate whether a single dose of nebulized budesonide effectively decreased airway inflammation as demonstrated by exhaled nitric oxide (eNO) levels. A single dose of nebulized budesonide, but not nebulized terbutaline, rapidly decreased eNO levels in 6 hours. The decrease in eNO levels induced by nebulized budesonide was correlated to an increase in peak expiratory flow rate. (J Pediatr 2001;139:433-7)
[本文引用:0]
|
| [28] |
尽管工业化进程推动了中国经济的飞速发展,但随之而来的环境恶化尤其是空气污染以及吸烟率居高不下等因素,使得呼吸系统疾病的防控工作面临严峻考验。呼吸系统疾病在我国城乡居民中最常见、病死率最高,经济负担也最重。雾化吸入疗法是呼吸系统相关疾病的重要治疗手段。与口服、肌肉注射和静脉给药等方式相比,雾化吸入疗法因药物直接作用于靶器官,具有起效迅速、疗效佳、全身不良反应少、不需要患者刻意配合等优势,被国内外广泛应用。在我国,由于缺乏药物、设备和临床经验等原因,许多基层医院甚至高级别医院在雾化吸入治疗中存在许多不规范之处,进而影响到患者的疗效[1]。基于此,中华医学会呼吸病学分会携手国内儿科、耳鼻喉科、胸外科和药理学相关领域知名专家制定本共识,以期更好地指导各级医务人员开展规范的雾化吸入治疗工作。
[本文引用:4]
|
| [29] |
正支气管哮喘急性发作是指喘息、气促、咳嗽、胸闷等症状突然发生,或原有症状急剧加重,伴有呼吸困难,以呼气流量降低为其特征,通常需要改变治疗药物。大多数情况与接触过敏原、刺激物或病毒性上呼吸道感染诱发及控制性药物依从性差有关,但也有少数患者无明确的诱因。急性发作总体治疗目标在于尽快缓解症状、解除支气管痉挛和改善缺氧,恢复肺功能,预防进一步恶化或再次发作,防治并发症。中华医学会呼吸病学分会哮喘学组,中国哮喘联盟制定《支气管哮喘急性发作评估及处理中国专家共识》,为支气管哮喘急性发作的临床诊
[本文引用:0]
|
| [30] |
|
| [31] |
|
| [32] |
目的 观察高龄慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)患者雾化吸入布地奈德混悬液的临床疗效及安全性评估.方法 25例高龄COPD稳定期患者随机分为两组,分别给予布地奈德1mg bid,2 mg bid雾化吸入1年.15例正常高龄老人为对照组.结果 雾化吸入布地奈德2mg bid明显改善COPD患者PaCO2(P<0.01)、FEV1 (P<0.05).治疗6m后两组CAT评分均较治疗前明显改善(P< 0.05,P<0.01);较高剂量组治疗12 m后CAT评分较治疗6m后有进一步改善(P<0.05),治疗6m后及12 m后的CAT改善率均优于较低剂量组(P<0.05,P< 0.01).两组患者治疗期内慢性阻塞性肺疾病急性加重的发生率无明显差异.治疗组与正常对照组相比,糖代谢及血尿骨代谢均无明显影响.治疗期间两组患者肺炎的发生率无明显差异.结论 雾化吸入布地奈德1年可改善中重度COPD高龄患者肺功能和临床症状,未对糖代谢和骨代谢产生不良影响.较高剂量雾化吸入布地奈德1年未增加COPD患者的肺炎发生率.
[本文引用:0]
|
| [33] |
|
| [34] |
2009年发表的《胸外科围手术期肺保护的专家共识》强调加强围手术期肺保护,采取各种有效措施减少肺部并发症,使患者“快速康复”。为了深化细化《胸外科围手术期肺保护的专家共识》,中华医学会胸心血管外科分会和中国医师协会胸外科医师分会在2009年《胸外科围手术期肺保护的共识》的基础上,组织有关专家反复学术研讨,就吸入型抗胆碱能药物在围手术期肺保护中的应用达成以下共识,供各位同道参考。
[本文引用:0]
|
| [35] |
篇首:
[本文引用:2]
|
| [36] |
目的 评价吸入用布地奈德混悬液雾化吸入对儿童腺样体大小的改善疗效.方法 114例腺样体肥大儿童自身前后对照方法,患者家长对于常见症状评分,腺样体经纤维鼻咽镜检查X线鼻咽侧位拍片.予以吸入用布地奈德混悬液雾化吸入,同时口服标准桃金娘油肠溶胶囊.结果 经治疗后儿童腺样体肥大引起的常见症状评分及体积变化差异具有统计学意义(P<0.05).入组114例病例中,显效79例,有效21例继续一个疗程治疗后明显好转,无效14例改行手术治疗,有效率87.7%.结论 吸入用布地奈德混悬液雾化吸入治疗儿童腺样体肥大临床效果良好,副作用小.
[本文引用:1]
|
| [37] |
|
| [38] |
BACKGROUND AND PURPOSE Muscarinic acetylcholine receptors (mAChRs) and 0205-adrenoceptors in the airways and lungs are clinically important in chronic obstructive pulmonary disease (COPD) and asthma. However, the quantitative and qualitative estimation of these receptors by radioligand binding approaches in human airways has not yet been reported because of tissue limitations.EXPERIMENTAL APPROACH The regional distribution and relative proportion of mAChR and 0205-adrenoceptor subtypes were evaluated in human bronchus and lung parenchyma by a tissue segment binding method with [3H]-N-methylscopolamine ([3H]-NMS) for mAChRs and [3H]-CGP-12,177 for 0205-adrenoceptors. Functional responses to carbachol and isoprenaline were also analysed in the bronchus.KEY RESULTS The M3 subtype predominantly occurred in the bronchus, but the density decreased from the segmental to subsegmental bronchus, and was absent in lung parenchyma. On the other hand, the M1 subtype occurred in the lung only, and the M2 subtype was distributed ubiquitously in the bronchus and lungs. 02052-adrenoceptors were increased along the airways, and their densities in the subsegmental bronchus and lung parenchyma were approximately twofold higher than those of mAChRs in the same region. 02051-adrenoceptors were also detected in lung parenchyma but not in the bronchus. The muscarinic contractions and adrenoceptor relaxations in both bronchial regions were mediated through M3-mAChRs and 02052-adrenoceptors, respectively.CONCLUSIONS AND IMPLICATIONS From the present radioligand binding approach with intact tissue segments, we constructed a distribution map of mAChRs and 0205-adrenoceptors in human bronchus and lung parenchyma for the first time, providing important evidence for future pharmacotherapy and new drug development for respiratory disorders.
[本文引用:1]
|
| [39] |
Abstract Bronchodilators are central in the treatment of of airways disorders. They are the mainstay of the current management of chronic obstructive pulmonary disease (COPD) and are critical in the symptomatic management of asthma, although controversies around the use of these drugs remain. Bronchodilators work through their direct relaxation effect on airway smooth muscle cells. at present, three major classes of bronchodilators, (2)-adrenoceptor (AR) agonists, muscarinic receptor antagonists, and xanthines are available and can be used individually or in combination. The use of the inhaled route is currently preferred to minimize systemic effects. Fast- and short-acting agents are best used for rescue of symptoms, whereas long-acting agents are best used for maintenance therapy. It has proven difficult to discover novel classes of bronchodilator drugs, although potential new targets are emerging. Consequently, the logical approach has been to improve the existing bronchodilators, although several novel broncholytic classes are under development. An important step in simplifying asthma and COPD management and improving adherence with prescribed therapy is to reduce the dose frequency to the minimum necessary to maintain disease control. Therefore, the incorporation of once-daily dose administration is an important strategy to improve adherence. Several once-daily (2)-AR agonists or ultra-long-acting (2)-AR-agonists (LABAs), such as indacaterol, olodaterol, and vilanterol, are already in the market or under development for the treatment of COPD and asthma, but current recommendations suggest the use of LABAs only in combination with an inhaled corticosteroid. In addition, some new potentially long-acting antimuscarinic agents, such as glycopyrronium bromide (NVA-237), aclidinium bromide, and umeclidinium bromide (GSK573719), are under development, as well as combinations of several classes of long-acting bronchodilator drugs, in an attempt to simplify treatment regimens as much as possible. This review will describe the pharmacology and therapeutics of old, new, and emerging classes of bronchodilator.
[本文引用:1]
|
| [40] |
|
| [41] |
Abstract Inhaled antibiotics have been used to treat chronic airway infections since the 1940s. The earliest experience with inhaled antibiotics involved aerosolizing antibiotics designed for parenteral administration. These formulations caused significant bronchial irritation due to added preservatives and nonphysiologic chemical composition. A major therapeutic advance took place in 1997, when tobramycin designed for inhalation was approved by the U.S. Food and Drug Administration (FDA) for use in patients with cystic fibrosis (CF) with chronic Pseudomonas aeruginosa infection. Attracted by the clinical benefits observed in CF and the availability of dry powder antibiotic formulations, there has been a growing interest in the use of inhaled antibiotics in other lower respiratory tract infections, such as non-CF bronchiectasis, ventilator-associated pneumonia, chronic obstructive pulmonary disease, mycobacterial disease, and in the post-lung transplant setting over the past decade. Antibiotics currently marketed for inhalation include nebulized and dry powder forms of tobramycin and colistin and nebulized aztreonam. Although both the U.S. Food and Drug Administration and European Medicines Agency have approved their use in CF, they have not been approved in other disease areas due to lack of supportive clinical trial evidence. Injectable formulations of gentamicin, tobramycin, amikacin, ceftazidime, and amphotericin are currently nebulized "off-label" to manage non-CF bronchiectasis, drug-resistant nontuberculous mycobacterial infections, ventilator-associated pneumonia, and post-transplant airway infections. Future inhaled antibiotic trials must focus on disease areas outside of CF with sample sizes large enough to evaluate clinically important endpoints such as exacerbations. Extrapolating from CF, the impact of eradicating organisms such as P. aeruginosa in non-CF bronchiectasis should also be evaluated.
[本文引用:1]
|
| [42] |
|
| [43] |
吸入疗法已经成为治疗呼吸系统疾病的常用治疗方法,主要包括压力定量吸入、干粉吸入和雾化吸入给药等。其中雾化吸入给药由于具有明显的优势,近几年来其临床应用药物种类、治疗疾病类型等都有了进一步的发展。笔者就雾化吸入给药的原理、现状及相关临床应用进展等进行综述。
[本文引用:1]
|
| [44] |
The effect of on mucus trasnport velocity (MV), ciliary beat frequency (), mucus production (MP), mucus lysis and on the micro-morphology of the secretory cells was studied in mammalian airways. The results showed that: 1. MV increased in healthy and , as well as in bronchitic , after concentrations as low as 10(-14) g/ml. of MV occurred first at 10(-6) and 10(-5) g/ml in healthy and bronchitic , respectively. 2. was stimulated at concentrations between 10(-12) and 10(-10) g/ml and decreased at concentrations above 10(-8) g/ml. 3. MP increased by approximately 100% over control values. 4. Lysis of stagnant mucus was evident first at a concentration of 10(-11) g/ml after 15 min incubation. 5. TEM confirmed the increased activity of the mucus secreting cells and showed that no pathological changes occurred within the cell following incubation at 10(-7) g/ml for up to 150 min. The importance of these findings on the overall mucociliary function is discussed.
[本文引用:1]
|
| [45] |
Abstract The purpose of the present study was to compare the effects of two mucolytic drugs with different mechanism of action on mucociliary transport (MCT). N-acetylcysteine (NAC-600 mg/day) and ambroxol (AMB-90 mg/day) were administered according to a double-blind cross-over scheme to 12 heavy smokers suffering from hypersecretory bronchitis and homogeneous reduction of the MCT. Placebo of both treatments was administered during an interval of ten days between the administrations of NAC and AMB. The entire treatment period was 30 days. The data were analyzed according to ANOVA for the two-period cross-over clinical trial. The results indicate that: NAC and AMB, administered both before and after placebo, produce a significant increase in MCT, NAC showed a slightly greater efficacy than AMB, but the differences are not statistically significant. The overall efficacy of NAC and AMB is consistently greater than that of placebo. The sequence of administration of the drugs does not influence their effect.
[本文引用:1]
|
| [46] |
Mereto GC, Balestra L, Henriquet F.
[本文引用:1]
|
| [47] |
|
| [48] |
Oxidative stress is involved in the pathogenesis of pulmonary fibrosis, therefore antioxidants may be of therapeutic value. Clinical work indicates that N-acetylcysteine (NAC) may be beneficial in this disease. The activity of this antioxidant was examined on bleomycin-induced lung damage, mucus secretory cells hyperplasia and mucin Muc5ac gene expression in rats. NAC (3 mmol x kg(-1) x day(-1)) or saline was given orally to Sprague-Dawley rats for 1 week prior to a single intratracheal instillation of bleomycin (2.5 U x kg(-1)) and for 14 days postinstillation. NAC decreased collagen deposition in bleomycin-exposed rats (hydroxyproline content was 4,257+/-323 and 3,200+/-192 microg x lung(-1) in vehicle- and NAC-treated rats, respectively) and lessened the fibrotic area assessed by morphometric analysis. The bleomycin-induced increases in lung tumour necrosis factor-alpha and myeloperoxidase activity were reduced by NAC treatment. The numbers of mucus secretory cells in airway epithelium, and the Muc5ac messenger ribonucleic acid and protein expression, were markedly augmented in rats exposed to bleomycin. These changes were significantly reduced in NAC-treated rats. These results indicate that bleomycin increases the number of airway secretory cells and their mucin production, and that oral N-acetylcysteine improved pulmonary lesions and reduced the mucus hypersecretion in the bleomycin rat model.
[本文引用:1]
|
| [49] |
Biofilms are microbial communities consisting of bacteria, extremely capable to self-reproduce on biological surfaces, causing infections. Frequently, these biofilms are resistant to classical antibacterial treatments and host immune response. Thus, new adjuvant molecules are mandatory in clinical practice. N-acetylcysteine (NAC), a precursor to the antioxidant glutathione, has been investigated for its effectiveness both in inhibiting biofilm formation and in destroying developed biofilms. The aim of our study was to conduct a systematic literature review of clinical trials involving NAC as adjuvant treatment to eradicate pre-formed mature biofilms and to inhibit new biofilm production.A careful analysis of the Medline was conducted and eight studies were selected according to the following criteria: site of infection, kind of bacteria, design of the research, dose of the treatment, administration, biological effects and results. We fixed an arbitrary scale of scores from 0 (lowest score) to 5 (highest score) for each criterion and a threshold value of 3.The studies analyzed, with score over 3, suggested a potential role for NAC as adjuvant molecule in the treatment of bacterial biofilms, with an excellent safety and efficacy profile. NAC, in combination with different antibiotics, significantly promoted their permeability to the deepest layers of the biofilm, overcoming the problem of the resistance to the classic antibacterial therapeutic approach.Overall, these results are encouraging to a more widespread clinical use of NAC, as adjuvant therapy for microbial infections followed by biofilm settle, which may occur in several body districts, such as the vaginal cavity.
[本文引用:1]
|
| [50] |
Antimicrob Agents Chemother. 2010 Aug;54(8):3529-30. doi: 10.1128/AAC.00710-10. Epub 2010 Jun 14. Letter
[本文引用:1]
|
| [51] |
目的:评价氨溴索(商品名沐舒坦)静滴与雾化吸入联用对新生儿肺炎的疗效。方法:将收治的新生儿肺炎患儿88例,分为治疗组(采用静脉滴注加雾化吸入沐舒坦)和对照组(采用静脉滴注沐舒坦),每组44例;两组患者在常规治疗的基础上,治疗组予大剂量沐舒坦,应用微量泵输注与雾化吸入;对照组患者给予微量泵输注沐舒坦治疗,观察两组患儿治疗前后临床表现、并发症的发生率和X-线胸片的变化,以及主要症状消失时间和住院时间的长短。结果:治疗组患者总有效率为95.45%,对照组患者为72.73%,总有效率经比较,其差异有统计学意义(P0.05);治疗组患者咳嗽消失时间(5.05±1.30)d,气促消失时间(3.12±1.02)d,肺部罗音消失时间(4.02±1.40)d及其住院时间(6.02±1.86)d;对照组患者分别为(6.46±1.38)d,(4.65±1.42)d,(7.66±2.40)d,(9.05±2.40)d,经两两比较其差异有统计学意义(P0.05)。结论:该法治疗新生儿肺炎,疗效确切,适用于新生儿肺炎的治疗。
[本文引用:1]
|
| [52] |
目的观察老年慢性支气管炎患者采用盐酸氨溴索雾化吸入疗法的临床效果。方法从医院收治的200例慢性支气管炎老年患者中抽取符合条件的70例患者作为研究对象,随机分为对照组和观察组,每组35例。对照组采用常规疗法,观察组在对照组基础上采用盐酸氨溴索雾化吸入疗法。观察2组治疗2周后的临床效果,统计2组患者咳嗽、气喘、发热、哮鸣音症状消失时间。结果观察组总有效率为85.71%,高于对照组的42.86%(P〈0.01)。观察组咳嗽、气喘、发热、哮鸣症状消失时间均短于对照组(P〈0.01)。结论在治疗老年慢性支气管炎患者中采用盐酸氨溴索雾化吸入疗法有利于提高其治疗效果,见效速度快,值得临床推广应用。
[本文引用:1]
|
| [53] |
目的评价静脉滴注联合雾化吸入盐酸氨溴索注射液治疗新生儿肺炎的临床疗效。方法计算机检索中国知网(CNKI)、维普中文数据库(VIP)、中国生物医学全文数据库(CBM)和万方数据等数据库,筛选有关静脉滴注联合雾化吸入盐酸氨溴索注射液治疗新生儿肺炎的随机对照研究(RCT),其中试验组患儿采用静脉滴注联合雾化吸入盐酸氨溴索注射液治疗,对照组患儿采用盐酸氨溴索注射液静脉滴注治疗。比较两组患儿临床疗效、咳嗽消失时间、气喘消失时间、肺部啰音消失时间、住院时间及药物不良反应发生率。结果最终共有11篇文献纳入Meta分析,共包含1 007例患儿。Meta分析结果显示,试验组患儿临床疗效优于对照组〔OR=3.60,95%CI(2.38,5.45),P〈0.000 01〕,咳嗽消失时间〔MD=-1.56,95%CI(-1.77,-1.35),P〈0.000 01〕、气喘消失时间〔MD=-0.89,95%CI(-1.28,-0.51),P〈0.000 01〕、肺部啰音消失时间〔MD=-1.31,95%CI(-1.51,-1.11),P〈0.00001〕和住院时间〔MD=-2.13,95%CI(-2.36,-1.91),P〈0.000 01〕短于对照组;两组患儿药物不良反应发生率比较,差异无统计学意义〔OR=1.09,95%CI(0.48,2.50),P=0.83〕。结论静脉滴注联合雾化吸入盐酸氨溴索注射液能提高新生儿肺炎的临床疗效,缩短临床症状消失时间及住院时间,且不增加药物不良反应发生风险。
[本文引用:2]
|
| [54] |
目的:系统评价盐酸氨溴索注射液静脉滴注联合雾化吸入治疗新生儿肺炎的疗效和安全性,以为临床提供循证参考.方法:计算机检索PubMed、Medline、中国生物医学文献数据库、中国期刊全文数据库、中文科技期刊数据库和万方数据库,收集盐酸氨溴索注射液静脉滴注联合雾化吸入(试验组)对比单用盐酸氨溴索注射液静脉滴注(对照组)治疗新生儿肺炎的随机对照试验(RCT),对符合纳入标准的临床研究进行资料提取,并采用Cochrane系统评价员手册5.1.0进行质量评价,采用Rev Man 5.2统计软件进行Meta分析.结果:共纳入14项RCT,合计1 407例患儿.Meta分析结果显示,试验组患儿的临床总有效率[RR=1.19, 95%CI(1.13,1.24),P<0.001]显著高于对照组,咳嗽消失时间[MD=-1.75,95%CI(-1.91,-1.58),P<0.001]、气喘消失时间[MD=-1.38,95%CI(-1.67,-1.08),P<0.001]、肺部啰音消失时间[MD=-1.44,95%CI(-1.77,-1.11),P<0.001]和住院天数[MD=-2.04,95%CI(-2.25,-1.82),P<0.001]均显著短于对照组,差异均有统计学意义;两组患儿不良反应发生率比较差异无统计学意义[RR=1.00,95%CI(0.49,2.05),P=1.00].结论:盐酸氨溴索注射液静脉滴注联合雾化吸入治疗新生儿肺炎的疗效和安全性均较好.
[本文引用:0]
|
| [55] |
目的分析在慢阻肺性急性加重期患者治疗中应用氧驱雾化吸入盐酸氨溴索进行治疗的疗效与护理方法。方法选取2015年2月至2016年2月我院接收治疗的慢阻肺急性加重期患者70例作为研究对象,分为观察与对照两组,对照组给予常规治疗,观察组在此基础上给予盐酸氨溴索氧驱雾化吸入治疗,并给予相应的护理措施,观察两组疗效。结果观察组治疗有效率为94.3%,明显比对照组的80%高,观察组护理满意度为97.1%,明显比对照组的77.1%高,差异存在统计学方面的意义(P<0.05)。结论在慢阻肺急性加重期患者的治疗中应用应用氧驱雾化吸入盐酸氨溴索治疗,并给以患者综合性的护理措施能够提升治疗效果,具有推广使用的价值。
[本文引用:0]
|
| [56] |
|
| [57] |
N -Acetylcysteine is useful as a mucolytic agent for treatment of chronic bronchitis and other pulmonary diseases complicated by the production of viscous mucus. It is also used as an antidote to paracetamol (acetaminophen) poisoning and found to be effective for the prevention of car-diotoxicity by doxorubicin and hae norrhagic cystitis from oxazaphosphorines.After an oral dose of N -acetylcysteine 200 to 400mg the peak plasma concentration of 0.35 to 4 mg/L is achieved within 1 to 2 hours. Although the data are conflicting, it appears that the administration of charcoal may interfere with drug absorption, with up to 96% of the drug adsorbed on to the charcoal. Information on absorption in the presence of food or other drugs is not available. The volume of distribution ranges from 0.33 to 0.47 L/kg and protein binding is significant, reaching approximately 50% 4 hours after the dose. Pharmacokinetic information is not available as to whether or not N -acetylcysteine crosses the blood-brain barrier or placenta, or into breast milk. Renal clearance has been reponed as 0.190 to 0.211 L/h/ke and approximately 70% of the total body clearance is nonrenal. Following oral administration, reduced /V-acetyl-cysteine has a terminal half-life of 6.25h. Little is known of the metabolism of this agent, although it is believed to be rapidly metabolised and incorporated on to proteins. The major excretory product is inorganic sulphate.Frequently reported side effects are nausea, vomiting and diarrhoea. Biochemical and hae-matological adverse effects are observed but are not clinically relevant. Drug interactions of clinical significance have been observed with paracetamol, glutathione and anticancer agents.
[本文引用:1]
|
| [58] |
|
| [59] |
|
| [60] |
目的:探究乙酰半胱氨酸雾化吸入治疗小儿气管炎的临床效果.方法:将我院收治的114例小儿气管炎患者作为观察对象,入院时间在2015年6月—2016年6月.将选取的患者采用随机分组法分为A、B两组后,每组57例患者.给予A组患者乙酰半胱氨酸雾化吸入治疗,B组患者采用常规疗法.将两组患者的治疗效果采用量化处理后,分别以数据的形式来进行统计,并在两组间进行对比,分析两种治疗方案的差异.结果:在A组中,治疗痊愈、显效、有效的病例数分别为25例、25例和5例,总有效率为96.5%(55/57);而在B组中,治疗痊愈、显效、有效的病例数分别为16例、20例和10例,总有效率为80.7%(46/57),A、B两组的有效率进行比较得出的差异显著(χ2=7.0327;P<0.05).同时,A组中出现不良反应的患者有3例,占5.3%,B组中,出现不良反应的有12例,占21.1%,两组进行比较得出的差异显著(χ2=6.2182;P<0.05).结论:采用乙酰半胱氨酸雾化吸入来治疗小儿气管炎,具有较好的临床效果,治疗的有效率高,快速缓解患儿咳嗽,痰粘稠等症状,并且患者出现不良反应的情况也较少,治疗的可行性和可行性较高,值得在临床推广应用.
[本文引用:1]
|
| [61] |
目的 探讨评价在老年慢性阻塞性肺疾病急性加重期(AECOPD)患者中使用N-乙酰半胱氨酸(NAC)雾化吸入治疗的临床疗效.方法 将60例IV级AECOPD患者随机分为观察组和对照组各30例,两组均给予常规治疗,观察组在常规治疗的基础上加用N-乙酰半胱氨酸(NAC)雾化吸入,2次/天.在入院第1天和入院后第14天测定比较两组患者血气分析(PaO2、PaCO2)、肺功能(FEV1%prd、FEV1/FVC%)及血清中CRP、PCT水平.结果 治疗第14天两组患者血气分析(PaO2、PaCO2)、肺功能(FEV1%prd、FEV1/FVC%)及血清中CRP、PCT水平均有好转(P〈0.05),且观察组较对照组改善更加明显,差异有统计学意义(P〈0.05). 结论 N-乙酰半胱氨酸(NAC)雾化吸入辅助治疗可明显改善老年AECOPD患者的临床症状和肺功能,减轻炎症反应,且安全有效.
[本文引用:1]
|
| [62] |
研究N-乙酰半胱氨酸(NAC)雾化吸入对稳定期COPD患者运动耐量和生活质量的影响。方法研究纳入 140例2012年4月~2013年6月在兰州石化总医院就诊的COPD稳定期患者。将上述患者随机分为仅有常规治疗的对照组和联合了NAC雾化吸入的观 察组。治疗6个月后,检测1秒用力呼气量(FEV 1)、深吸气量(IC),功能残气量(FRC)、最大耗氧量(VO2 max)等指标,并进行6分钟步行试验和Brog呼吸困难评分,圣乔治呼吸问卷评估患者生活质量。结果2组患者的肺功能指标、VO2max、六分钟步行试 验行走距离、圣乔治呼吸问卷评分均比治疗前有所改善,但是观察组上述指标的改善更明显,在反应运动耐量的指标方面要优于对照组(P<0.05)。结 论 NAC雾化吸入能够改善COPD患者的运动耐量和生活质量。
[本文引用:1]
|
| [63] |
Abstract Inhalation injury causes a heterogeneous cascade of insults that increase morbidity and mortality among the burn population. Despite major advancements in burn care for the past several decades, there remains a significant burden of disease attributable to inhalation injury. For this reason, effort has been devoted to finding new therapeutic approaches to improve outcomes for patients who sustain inhalation injuries.The three major injury classes are the following: supraglottic, subglottic, and systemic. Treatment options for these three subtypes differ based on the pathophysiologic changes that each one elicits.Currently, no consensus exists for diagnosis or grading of the injury, and there are large variations in treatment worldwide, ranging from observation and conservative management to advanced therapies with nebulization of different pharmacologic agents.The main pathophysiologic change after a subglottic inhalation injury is an increase in the bronchial blood flow. An induced mucosal hyperemia leads to edema, increases mucus secretion and plasma transudation into the airways, disables the mucociliary escalator, and inactivates hypoxic vasocontriction. Collectively, these insults potentiate airway obstruction with casts formed from epithelial debris, fibrin clots, and inspissated mucus, resulting in impaired ventilation. Prompt bronchoscopic diagnosis and multimodal treatment improve outcomes. Despite the lack of globally accepted standard treatments, data exist to support the use of bronchoscopy and suctioning to remove debris, nebulized heparin for fibrin casts, nebulized N-acetylcysteine for mucus casts, and bronchodilators.Systemic effects of inhalation injury occur both indirectly from hypoxia or hypercapnia resulting from loss of pulmonary function and systemic effects of proinflammatory cytokines, as well as directly from metabolic poisons such as carbon monoxide and cyanide. Both present with nonspecific clinical symptoms including cardiovascular collapse. Carbon monoxide intoxication should be treated with oxygen and cyanide with hydroxocobalamin.Inhalation injury remains a great challenge for clinicians and an area of opportunity for scientists. Management of this concomitant injury lags behind other aspects of burn care. More clinical research is required to improve the outcome of inhalation injury.The goal of this review is to comprehensively summarize the diagnoses, treatment options, and current research.
DOI:10.1097/SAP.0000000000001377
PMID:29461292
[本文引用:1]
|
| [64] |
目的:探讨富露施雾化吸入对支气管扩张住院病人的临床疗效.方法:将52例支气管扩张住院患者分为观察组(27例)和对照组(25例),分别在支持性治疗基础上加用乙酰半胱氨酸和高渗盐雾化吸入,比较两组临床治疗效果.结果:观察组患者痰量减少时间、咳嗽消失时间和住院时间均短于对照组,肺功能改善优于对照组,比较差异显著(P<0.05).结论:雾化吸入是提高支气管扩张住院患者临床疗效的有效方法,其中乙酰半胱氨酸雾化吸入的临床应用价值值得肯定.
[本文引用:1]
|
| [65] |
Background Short-term studies have shown that inhaled corticosteroids may reduce the growth of children with asthma. However, the effect of long-term treatment on adult height is uncertain. Methods We conducted a prospective study in children with asthma to examine the effect of long-term treatment with inhaled budesonide on adult height. We report on 211 children who have attained adult height: 142 budesonide-treated children with asthma, 18 control patients with asthma who have never received inhaled corticosteroids, and 51 healthy siblings of patients in the budesonide group, who also served as controls. Results The children in the budesonide group attained adult height after a mean of 9.2 years of budesonide treatment (range, 3 to 13) at a mean daily dose of 412 mug (range, 110 to 877). The mean cumulative dose of budesonide was 1.35 g (range, 0.41 to 3.99). The mean differences between the measured and target adult heights were +0.3 cm (95 percent confidence interval, -0.6 to +1.2) for the budesonide-treated children, -0.2 cm (95 percent confidence interval, -2.4 to +2.1) for the control children with asthma, and +0.9 cm (95 percent confidence interval, -0.4 to +2.2) for the healthy siblings. The adult height depended significantly (P<0.001) on the child's height before budesonide treatment. Although growth rates were significantly reduced during the first years of budesonide treatment, these changes in growth rate were not significantly associated with adult height. Conclusions Children with asthma who have received long-term treatment with budesonide attain normal adult height.
[本文引用:1]
|
| [66] |
Pediatric Research publishes original papers, invited reviews, and commentaries on the etiologies of diseases of children and disorders of development, extending from molecular biology to epidemiology. Use of model organisms and in vitro techniques relevant to developmental biology and medicine are acceptable, as are translational human studies.
[本文引用:1]
|
| [67] |
Three open-label extension trials evaluated the safety of budesonide inhalation suspension (BIS; Pulmicort Respules) in 670 children (8 months-9 years of age) with mild-to-severe persistent asthma. Patients were randomized to receive either BIS or conventional asthma therapy (CAT) for 52 weeks. The percentage of patients who discontinued because of clinical adverse events was low and similar among the CAT (0.4%) and BIS (0.7%) groups. After adjusting for length of time in the studies, there were no clinically relevant differences between the BIS and CAT groups in the type, incidence, or intensity of adverse events; vital signs or physical examination outcomes; or changes in clinical laboratory evaluations or oral fungal cultures.
[本文引用:1]
|
| [68] |
|
| [69] |
|
| [70] |
The widespread use of inhaled corticosteroids (ICS) for the treatment of persistent asthma, although highly effective, may be associated with both systemic and local side effects. Systemic side effects of ICS have been extensively studied. In contrast, relatively few studies have been performed to specifically evaluate local side effects of ICS. These local side effects 090009 including oropharyngeal candidiasis, dysphonia, pharyngitis, and cough 090009 are generally viewed as minor complications of therapy. However, they can be clinically significant, affect patient quality of life, hinder compliance with therapy, and mask symptoms of more serious disease. Local side effects result from deposition of an active ICS in the oropharynx during administration of the drug. Numerous factors can influence the proportion of an inhaled dose that is deposited in the oropharyngeal cavity, including the ICS formulation, type of delivery system, and patient compliance with administration instructions. Therefore, the incidence of local side effects can vary widely. The goal in developing a new ICS is to include key pharmacologic characteristics that reduce oropharyngeal exposure to active drug while maintaining efficacy comparable with currently available ICS.
[本文引用:1]
|
| [71] |
Long-term inhaled corticosteroids (ICS) may reduce growth velocity and final height of children with asthma. We aimed to evaluate the association between ICS use of >12 months and growth. We initially searched MEDLINE and EMBASE in July 2013, followed by a PubMed search updated to December 2014. We selected RCTs and controlled observational studies of ICS use in patients with asthma. We conducted random effects meta-analysis of mean differences in growth velocity (cm/year) or final height (cm) between groups. Heterogeneity was assessed using the I2 statistic. We found 23 relevant studies (twenty RCTs and three observational studies) after screening 1882 hits. Meta-analysis of 16 RCTs showed that ICS use significantly reduced growth velocity at one year follow-up (mean difference -0.48 cm/year (95% CI -0.66 to -0.29)). There was evidence of a dose-response effect in three RCTs. Final adult height showed a mean reduction of -1.20 cm (95% CI -1.90 cm to -0.50 cm) with budesonide versus placebo in a high quality RCT. Meta-analysis of two lower quality observational studies revealed uncertainty in the association between ICS use and final adult height, pooled mean difference -0.85 cm (95% CI -3.35 to 1.65). Use of ICS for >12 months in children with asthma has a limited impact on annual growth velocity. In ICS users, there is a slight reduction of about a centimeter in final adult height, which when interpreted in the context of average adult height in England (175 cm for men and 161 cm for women), represents a 0.7% reduction compared to non-ICS users.
[本文引用:1]
|
| [72] |
Corticosteroids have a significant role in the management of asthma due to their powerful anti-inflammatory actions. However, when given orally, they cause significant and unwanted side-effects. Early attempts to circumvent these side-effects were largely unsuccessful. Recently, new synthetic corticosteroids have been developed that have powerful topical action but weak generalised effects due to rapid systemic metabolism. These new compounds provide adequate control of airways' obstruction in almost all asthmatics. Oral candidiasis may occur but can generally be controlled by adjusting the frequency of dosage and changing delivery systems. In high doses, there is biochemical evidence of adrenal suppression, but the clinical importance of this is not yet clear and there is no evidence of a significant effect on growth in children. High dose inhaled corticosteroids have been shown to affect biochemical indices of bone turnover in the short term. The long term clinical consequences of this are still under evaluation. Inhaled corticosteroids have provided a significant advance in the management of asthma, but physicans need to remain alert for the possibility of systemic side effects when used in high doses for long periods of time.
[本文引用:1]
|
| [73] |
|
| [74] |
|
| [75] |
Clearly, determining the cause of a suspectedadverse reaction to an inhaled medication may not be straightforward. An increasing number of drugs are being prescribed by the inhaled route using unlicensed formulations, presumably on the physician's own responsibility; these include a variety of antibiotic agents and recently the diuretic agents frusemide (34) and amiloride (35). It is the responsibility of all medical practitioners to find out the physico-chemical characteristics and the actual components of the medications they prescribe, in order to minimize the occurrence of the adverse reactions reviewed above.
[本文引用:1]
|
| [76] |
Inhalation therapy has been employed as the mainstay of the treatment in chronic respiratory diseases such as asthma and chronic obstructive pulmonary disease (COPD). Beta-2 agonists, anticholinergic bronchodilators, inhaled corticosteroids, and sodium cromoglycate are often used alone or in combination in an inhaled form. Studies have shown that inhaled drugs used in the treatment have some adverse effects on the oral health based on their dosage, frequency, and duration of use. Several oral conditions such as xerostomia, dental caries, candidiasis, ulceration, gingivitis, periodontitis, and taste changes have been associated with inhalation therapy. Since the prevalence of chronic respiratory diseases is rising, it is important to provide optimal oral care to the individuals receiving inhalation therapy. This article will review the influence of inhaled drugs on the oral health of individuals and adequate management and prevention of the same.
[本文引用:1]
|
| [77] |
DOI:10.2147/COPD
URL
[本文引用:1]
|
| [78] |
|
| [79] |
|
| [80] |
Highlights of the National Asthma Education and Prevention Program's Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Full Report 2007 are presented in this EPR-3 summary report. The updated guidelines emphasize the importance of asthma control. Asthma control is the degree to which the manifestations of asthma are minimized by therapeutic intervention and the goals of therapy are met. Because asthma is highly variable, the level of control must be monitored on a periodic basis to determine whether therapy should be maintained or adjusted (stepped up if necessary, stepped down if possible). On the other hand, asthma severity is the intrinsic intensity of the disease process, most easily and directly measured in a patient not receiving long-term control therapy. For managing asthma, the recommendation is to assess severity to initiate therapy and assess control to adjust therapy. Recommendations for managing asthma include an expanded section on childhood asthma with addition of an age group 5 to 11 years old (earlier guidelines combined this group with adults). The guidelines provide new recommendations on patient education in settings beyond the physician's office, and new advice for controlling environmental factors that can cause asthma symptoms.The concepts of current impairment (frequency and intensity of symptoms, low lung function, and limitations of daily activities) and future risk (likelihood of exacerbations, progressive loss of lung function, or adverse side effects from medications) support a new approach to assessing and monitoring the patient's level of asthma control through use of multiple measures. The guidelines stress that some patients can still be at high risk for frequent exacerbations even if they have few day-to-day effects of asthma.Moreover, EPR-3 confirms the importance of teaching patients skills to self-monitor and manage asthma and to use a written asthma action plan, which should include instruction
[本文引用:1]
|
| [81] |
|
| [82] |
Background: Inhaled corticosteroids are recommended as first-line therapy for pregnant women with moderate to severe asthma, although the effects on pregnancy outcome are uncertain. A low compliance with the recommendations might lead to inadequate control of asthma, which has been associated with adverse outcomes both for the mother and the infant. Objective: To investigate whether the reported use of inhaled budesonide (Pulmicort) during pregnancy influences birth outcome. Methods: Data were derived from the Swedish Medical Birth Register, which includes 99% of births in Sweden. During 1995 to 1998, 293,948 newborn infants were identified. Pregnancy outcomes were compared for mothers in Sweden reporting asthma medication usage with those reporting no asthma medication usage. Results: The 2968 mothers who reported use of inhaled budesonide during early pregnancy gave birth to infants of normal gestational age, birth weight, and length, with no increased rate of stillbirths or multiple births. The rate of caesarean births was higher among mothers who used asthma medication during their pregnancy than among the control group. Conclusions: The use of inhaled budesonide in Sweden is not linked with any clinically relevant effects associated with pregnancy outcome.
[本文引用:1]
|
| [83] |
|
| [84] |
@@
[本文引用:1]
|
| [85] |
气道高反应性( B H R ) 是目前临床上很多疾病的常见症状, 且没有良好的治疗方法, 发病率高, 长期导致患者病情加重, 严重影响患者生存质量, 目前临床治疗 B H R疾病主要通过雾化吸入方式, 如糖皮质激素类药物布地奈德、 β受体激动剂沙丁胺醇和抗胆碱能药物异丙托溴铵; 口服平滑肌松弛类药物茶碱类和抗白三烯类药物孟鲁司特钠等方法控制B H R疾病.糖皮质激素是控制气道高反应性疾病相对有效的方法, 中药在缩短病程, 治疗病因方面有独特的优势.本文总结了针对气道高反应性疾病临床研究情况, 阐述了各类药物在治疗该疾病中的优劣势, 以期对此类疾病的治疗提供参考.
[本文引用:1]
|
| [86] |
气道高反应性(AHR)为支气管哮喘的共同病理生理特征,然而出现AHR者并非都是支气管哮喘,慢性阻塞性肺疾病、病毒性上呼吸道感染、支气管扩张、肺结核等也可出现AHR。现对AHR的发生机制及与之相关临床疾病作一综述。
[本文引用:1]
|
| [87] |
气道高反应性是由于各种物理或者化学刺激引起的支气管强烈收缩,且病理生理特征以小支气管明显痉挛收缩为主。临床上用于治疗呼吸道疾病最有效的抗炎药物是糖皮质激素,局部应用可以作用于气道内几乎所有的细胞,并且抑制气道炎症或阻止炎症细胞进入气道。吸入性糖皮质激素作为局部气道用药可通过减少免疫炎症介质的生成,抑制炎症因子产生,降低气道高反应。糖皮质激素通过某些机制来调节基因转录进而影响大多数炎症介质产生和释放。通过吸入的糖皮质激素对于大多数患者非常有效且全身不良反应少。
[本文引用:1]
|
| [88] |
\0
[本文引用:1]
|
| [89] |
To identify Mycobacterium tuberculosis virulence factors, we integrated comparative genomics and epidemiologic data analysis to investigate the relationship between certain genomic insertions and deletions in the phospholipase-C gene D (plcD) with the clinical presentation of tuberculosis (TB). Four hundred ninety-six well-characterized M. tuberculosis clinical isolates were studied. Approximately 30% (147) of the isolates had an interruption of the plcD gene. Patients infected with the plcD mutant were twice as likely to have extrathoracic disease as those infected by a strain without an interruption (adjusted odds ratio, 2.19; 95% confidence interval, 1.27, 3.76). When we limited the analysis to the 275 isolates with distinct DNA fingerprint patterns, we observed the same association (adjusted odds ratio, 2.74; 95% confidence interval, 1.35, 5.56). Furthermore, the magnitude of the association appeared to differ with the type of extrathoracic TB. Our findings suggest that the plcD gene of M. tuberculosis is potentially involved in the pathogenesis of TB, and the clinical presentation of the disease may be influenced by the genetic variability of the plcD region.
[本文引用:0]
|
| [90] |
|

{kind=link}
{kind=link}