Objective To develop a rapid ultra high performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) for determination of rivaroxaban in human plasma. Methods Sample treatment procedure was based on the use of the protein precipitation technique with acetonitrile.D4-rivaroxaban was selected as internal standard.The chromatographic separation was performed with a Thermo Hypersil Gold C18 analytical column (2.1 mm×100 mm, 1.9 μm) and a gradient mobile phase \[acetonitrile and water containing 0.1% formic acid and 5 mmol·L -1 ammonium acetate\].API 4000+ triple-quadrapole MS/MS detection coupled with UPLC LC-30AD was operated in a positive mode by multiple reaction monitoring.Ion transitions at m/z 436.1→m/z 145.1 for rivaroxaban and m/z 440.2→m/z 145.0 for d4-rivaroxaban (internal standard) were used for the UPLC-MS/MS analysis, respectively. Results Good linearity was obtained for rivaroxaban within the range of 1-500 ng·mL-1 in human plasma.The lower limits of quantification of current method was 1 ng·mL-1 for rivaroxaban.The intra- and inter-day precision was <8%.The absolute recoveries ranged from 90.09% to 95.23% and the matrix effects were 93.50%~100.09%.The sample concentration was not changed significantly under the following condition: 20 ℃ for 4 h, at 4 ℃ for 24 h, at -80 ℃ for 50 days, freezing and thawing 3 circles. Conclusion Precision, accuracy, recovery, matrix effect and stability for rivaroxaban are excellent within a wide calibration range.The established method is easy and rapid.It could be applied to the quantification of rivaroxaban in human plasma and contribute to clinical drug-drug interaction study as well as individualized medication.
Key words:
Rivaroxaban
;
Chromatography-tandem mass spectrometry
;
ultra high performance liquid
;
Plasma concentration
Fig.1
UPLC-MS/MS chromatograms of rivaroxaban and rivaroxaban in human plasma at d4 A.blank plasma; B.blank plasma spiked with rivaroxaban at 1 ng·mL-1 and d4- rivaroxaban
PERZBORNE,ROEHRIGS,STRAUBA,et al.Rivaroxaban:a new oral factor Xa inhibitor[J].Arterioscler Thromb Vasc Biol,2010,30(3):376-381.
Currently available anticoagulants utilized for venous thromboembolism (VTE) treatment and prevention and stroke prevention in patients with atrial fibrillation (AF) have proven effectiveness but are not optimally utilized because of barriers such as the need for subcutaneous administration and requisite routine laboratory monitoring. Rivaroxaban, a novel oral Xa inhibitor, is an alternative to standard therapies utilized for VTE prevention after elective orthopedic surgery, primary and secondary stroke prevention in nonvalvular AF, VTE treatment after an acute VTE event, and secondary prevention after the acute coronary syndromes (ACS). This article reviews the pharmacology, efficacy, and tolerability of rivaroxaban for VTE prophylaxis in post rthopedic surgery and medically ill patients, stroke prevention in nonvalvular AF, adjunctive therapy in patients with ACS, and VTE treatment. International Pharmaceutical Abstracts and EMBASE were searched for English-only clinical trials and reviews published between 1970 and March 15, 2012. PubMed was searched for articles published between 1970 and June 30, 2012. Additional trials and reviews were identified from the citations of published articles. Eighty-nine publications were identified: 10 clinical trials and 1 meta-analysis were used to obtain efficacy and tolerability data, and 1 analysis of pooled data from the clinical trials was included; 17 pharmacokinetic, pharmacodynamic, and drug rug interaction studies were included; and 5 cost-analyses were reviewed. These data showed rivaroxaban to be noninferior to enoxaparin for thromboprophylaxis of VTE after total knee and total hip replacement surgery. It was also shown to be noninferior to vitamin K antagonist therapy for primary and recurrent stroke prevention in nonvalvular AF as well as for the treatment of VTE after an acute deep vein thrombosis or pulmonary embolism. It also showed benefit in lowering the risk for major adverse cardiovascular events after ACS. Differences in major bleeding rates were not statistically significant between rivaroxaban and comparators across the various studies, with the exception of ACS, in which there were higher rates of non oronary artery bypass graft surgery related bleeding and intracranial hemorrhage. Based on the findings of the studies reported in this review, rivaroxaban is an effective option for the prevention of VTE after orthopedic surgery, stroke prevention for nonvalvular AF, and treatment of VTE. At this time, rivaroxaban cannot be recommended for secondary risk reduction after ACS because of the increased bleeding risk.
EINSTEIN-PEINVESTIGATORS,BULLER HR,PRINS MH,et al.Oral rivaroxaban for the treatment of symptomatic pulmonary embolism[J].N Engl J Med,2012,366(14):1287-1297.
[本文引用:1]
[3]
EINSTEININVESTIGATORS,BAUERSACHSR,BERKO-WITZ S D,et al.Oral rivaroxaban for symptomatic venous thromboembolism[J].N Engl J Med,2010,363(26):2499-2510.
WONG KS,HU DY,OOMMANA,et al.Rivaroxaban for stroke prevention in East Asian patients from the ROCKET AF trial[J].Stroke,2014,45(6):1739-1747.
Background and Purpose-In Rivaroxaban Once Daily Oral Direct Factor Xa Inhibitor Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) trial, rivaroxaban was noninferior to dose-adjusted warfarin in preventing stroke or systemic embolism among patients with nonvalvular atrial fibrillation at moderate to high stroke risk. Because of differences in patient demographics, epidemiology, and stroke risk management in East Asia, outcomes and relative effects of rivaroxaban versus warfarin were assessed to determine consistency among East Asians versus other ROCKET AF participants.<br/>Methods-Baseline demographics and interaction of treatment effects of rivaroxaban and warfarin among patients within East Asia and outside were assessed.<br/>Results-A total of 932 (6.5%) ROCKET AF participants resided in East Asia. At baseline, East Asians had lower weight, creatinine clearance, and prior vitamin K antagonist use; higher prevalence of prior stroke; and less congestive heart failure and prior myocardial infarction than other participants. Despite higher absolute event rates for efficacy and safety outcomes in East Asians, the relative efficacy of rivaroxaban (20 mg once daily; 15 mg once daily for creatinine clearance of 30-49 mL/min) versus warfarin with respect to the primary efficacy end point (stroke/systemic embolism) was consistent among East Asians and non-East Asians (interaction P=0.666). Relative event rates for the major or nonmajor clinically relevant bleeding in patients treated with rivaroxaban and warfarin were consistent among East Asians and non-East Asians (interaction P=0.867).<br/>Conclusions-Observed relative efficacy and safety of rivaroxaban versus warfarin were similar among patients within and outside East Asia. Rivaroxaban, 20 mg once daily, is an alternative to warfarin for stroke prevention in East Asians with nonvalvular atrial fibrillation.
ASMIS LM,ALBERIOL,ANGELILLO-SCHERRERA,et al.Rivaroxaban:quantification by anti-FXa assay and influence on coagulation tests:a study in 9 Swiss laboratories[J].Thromb Res,2012,129(4):492-498.
Introduction: Rivaroxaban (RXA) is licensed for prophylaxis of venous thromboembolism after major orthopaedic surgery of the lower limbs. Currently, no test to quantify RXA in plasma has been validated in an inter-laboratory setting.<br/>Our study had three aims: to assess i) the feasibility of RXA quantification with a commercial anti-FXa assay, ii) its accuracy and precision in an inter-laboratory setting, and iii) the influence of 10 mg of RXA on routine coagulation tests.<br/>Methods: The same chromogenic anti-FXa assay (Hyphen BioMed) was used in all participating laboratories. RXA calibrators and sets of blinded probes (aim ii.) were prepared in vitro by spiking normal plasma. The precise RXA content was assessed by high-pressure liquid chromatography-tandem mass spectrometry. For ex-vivo studies (aim iii), plasma samples from 20 healthy volunteers taken before and 2 - 3 hours after ingestion of 10 mg of RXA were analyzed by participating laboratories.<br/>Results: RXA can be assayed chromogenically. Among the participating laboratories, the mean accuracy and the mean coefficient of variation for precision of RXA quantification were 7.0% and 8.8%, respectively. Mean RXA concentration was 114 +/- 43 mu g/L. RXA significantly altered prothrombin time, activated partial thromboplastin time, factor analysis for intrinsic and extrinsic factors. Determinations of thrombin time, fibrinogen, FXIII and D-Dimer levels were not affected.<br/>Conclusions: RXA plasma levels can be quantified accurately and precisely by a chromogenic anti-FXa assay on different coagulometers in different laboratories. Ingestion of 10 mg RXA results in significant alterations of both PT-and aPTT-based coagulation assays. (C) 2011 Elsevier Ltd. All rights reserved.
KOROSTELEVM,BIHANK,FERREOLL,et al.Simultaneous determination of rivaroxaban and dabigatran levels in human plasma by high-performance liquid chromatography-tandem mass spectrometry[J].J Pharm Biomed Anal,2014,100:230-235.
A sensitive and accurate liquid chromatography method with mass spectrometry detection was developed and validated for the quantification of dabigatran (Pradaxa03) and rivaroxaban (Xarelto03). 13C6-dabigatran and 13C6-rivaroxaban were used as the internal standard. A single-step protein precipitation was used for plasma sample preparation. This method was validated with respect to linearity, selectivity, inter- and intra-day precision and accuracy, limit of quantification and stability. The lower limit of quantification was 2.5ng/mL for both drugs in plasma.
AL-AIESHYF,MALMSTROM RE,ANTOVICJ,et al.Clinical evaluation of laboratory methods to monitor exposure of rivaroxaban at trough and peak in patients with atrial fibrillation[J].Eur J Clin Pharmacol,2016,72(6):671-679.
The one-dose daily regime of rivaroxaban could cause a pronounced variability in concentration and effect of which a deeper knowledge is warranted. This study aimed to evaluate the typical exposure range and effect of the direct factor Xa (FXa)-inhibitor rivaroxaban in a cohort of well-characterized patients with atrial fibrillation (AF). Seventy-one AF patients (72 卤 8 years, 55 % men) were treated with rivaroxaban 15 mg/20 mg (n = 10/61) OD. Trough (n = 71) and peak (n = 30) plasma concentrations determined by liquid chromatography-tandem mass-spectrometry (LC-MS/MS) were compared to the coagulation assays anti-FXa for rivaroxaban, prothrombin time-international normalized ratio (PT-INR) (venous samples and point-of-care assay (POC) CoaguChek XS Pro), and aPTT. Median rivaroxaban plasma concentrations by LC-MS/MS were 34 (range 5-84) and 233 ng/ml (range 120-375) at trough and peak, respectively. A strong correlation between LC-MS/MS and the anti-FXa assay was found (p < 0.001) for both trough (r (2) = 0.92) and peak (r (2) = 0.91) samples. PT-INR results from the POC assay, but not from the conventional PT assay, correlated significantly with LC-MS/MS in peak samples exclusively (r (2) = 0.41, p < 0.001). In "real-life" AF patients treated with rivaroxaban, we observed a pronounced variability in plasma concentrations at trough and to a lesser extent at peak measured by LC-MS/MS. The anti-FXa assay performed well upon rivaroxaban levels in a normal exposure range, although LC-MS/MS remains the only method that covers the whole concentration range with accuracy. Interestingly, the POC assay for PT-INR could be useful to indicate high exposure to rivaroxaban in emergency situations although further validation is required.
ZHAOX,SUNP,ZHOUY,et al.Safety,pharmacokinetics and pharmacodynamics of single/multiple doses of the oral,direct Factor Xa inhibitor rivaroxaban in healthy Chinese subjects[J].Br J Clin Pharmacol,2009,68(1):77-88.
WHAT IS ALREADY KNOWN ABOUT THIS SUBJECT 090004 Rivaroxaban is an oral, direct Factor Xa inhibitor in advanced clinical development for the prevention and treatment of thromboembolic disorders. 090004 In single- and multiple-dose Phase I studies in White subjects, rivaroxaban was safe and demonstrated predictable, dose-dependent pharmacokinetics and pharmacodynamics. WHAT THIS STUDY ADDS 090004 The Phase III programme with rivaroxaban is being conducted worldwide. 090004 Therefore, it is necessary to determine whether the pharmacokinetics, pharmacodynamics and tolerability of rivaroxaban are altered in patients of different ethnic origins. 090004 Dose-escalation studies were conducted to determine the safety, pharmacokinetics and pharmacodynamics of single and multiple doses of rivaroxaban in healthy Chinese subjects. AIMS To investigate the safety, pharmacokinetics and pharmacodynamics of rivaroxaban, an oral, direct Factor Xa (FXa) inhibitor, in healthy, male Chinese subjects. METHODS Two randomized, single-blind, placebo-controlled, dose-escalation studies were conducted in healthy Chinese men aged 1809000945 years. In the single-dose study, subjects received single, oral doses of rivaroxaban 2.5, 5, 10, 20 and 40 mg. In the multiple-dose study, oral rivaroxaban was administered in doses of 5, 10, 20 and 30 mg twice daily for 6 days. RESULTS Rivaroxaban, in single and multiple doses up to 60 mg, was well tolerated. Rapid absorption was observed in both studies (time to C max 1.250900092.5 h). In the multiple-dose study, rivaroxaban exposure increased dose-proportionally after the first dose and at steady state (for the 509000920-mg doses). The half-life of rivaroxaban was up to 7.9 h in the single-dose study. Maximal inhibition of FXa activity was achieved within 10900093 h of dosing in the single-dose study [at 20 mg FXa inhibition as a median percentage change from baseline, 45.92; 95% confidence interval (CI) 44.64, 50.70] and 20900093 h after administration at steady state in the multiple-dose study (at 20 mg median FXa inhibition as a median percentage change from baseline, 60.25; 95% CI 56.16, 63.05), in line with maximum rivaroxaban plasma concentrations. CONCLUSIONS Rivaroxaban demonstrated predictable pharmacokinetics and pharmacodynamics in healthy Chinese subjects, in line with findings observed previously in White subjects. This suggests that fixed doses of rivaroxaban may be administered to all patients, regardless of their ethnic origin.
BALDELLIS,CATTANEOD,PIGNATELLIP,et al.Validation of an LC-MS/MS method for the simultaneous quantification of dabigatran,rivaroxaban and apixaban in human plasma[J].Bioanalysis,2016,8(4):275-283.
Aim:Novel oral anticoagulants are characterized by a wide therapeutic window, yet the determination of their plasma–drug concentrations may be useful in some clinical conditions.Results:An LC–MS/MS method for the analysis of dabigatran, apixaban and rivaroxaban in human plasma has been successfully developed and validated. The analysis of plasma samples from patients given other concomitant drugs revealed no significant interference. By reanalysis of samples from patients on anticoagulant therapy, we found the percentage difference in results between the concentration of repeat and the original sample to be within the threshold limit of 20 in 60 of 63 specimens.Conclusion:The developed LC–MS/MS assay is easily applicable in the clinical management of patients on anticoagulation therapy.

 , 陈志青
, 陈志青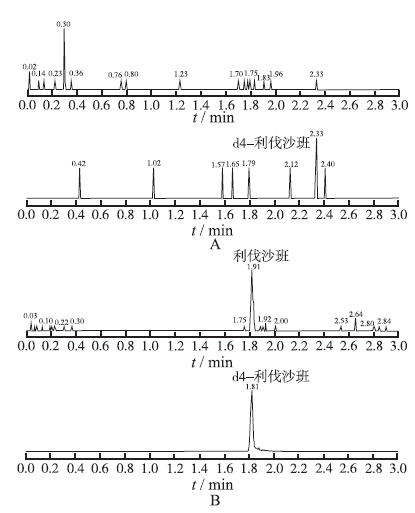

{kind=link}
{kind=link}