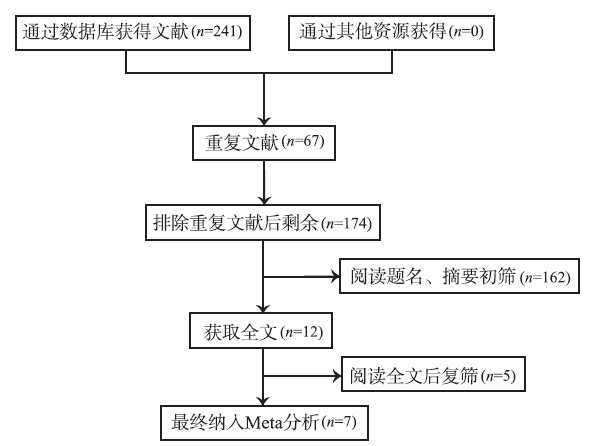
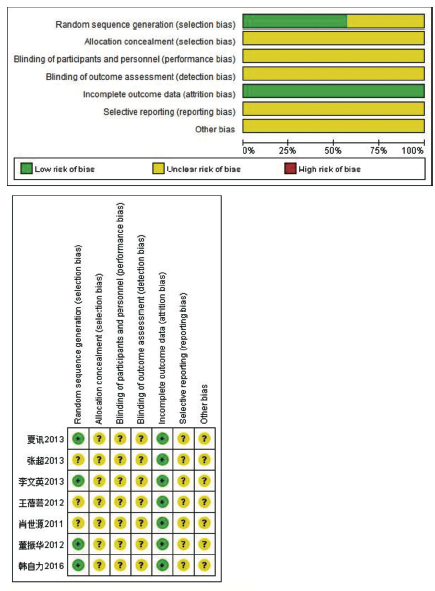
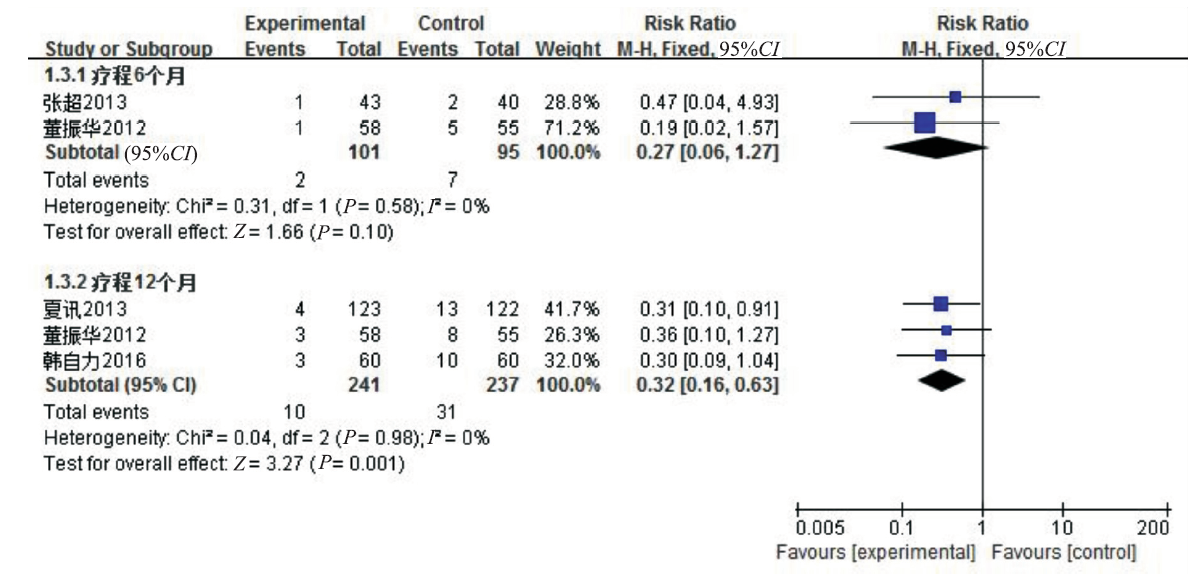
Objective To evaluate the efficacy and safety of oral ginkgo biloba extract EGB761 in patients with mild cognitive impairment. Methods They searched PubMed,Embase,the Cochrane Library ,CNKI,Wanfang and VIP databases for randomly controlled trials of oral ginkgo biloba extract for mild cognitive impairment.After assessed the quality of studies included,RevMan5.2 software was used to analyze data. Results Seven studies which including 815 patients were involved by our inclusion criteria.The results of meta-analysis showed,compared with the control group,ginkgo biloba was superior in improving mild cognitive impairment patients' MMSE level[MD=1.81,95%CI(0.02,3.60),P=0.05;MD=1.96,95%CI(1.48,2.43),P<0.000 01;MD=1.79,95%CI(0.99,2.58),P<0.000 1] after treated three months、six months and twelve months. Ginkgo biloba was also superior in improving mild cognitive impaimant patients.CDT level[MD=0.43,95%CI(0.30,0.57),P<0.000 01;MD=0.57,95%CI(0.39,0.75),P<0.000 01] after treated six months and twelve months.The effect of preventing MCI patients into dementia was better than that of the control group[RR=0.27,95%CI(0.06,1.27),P=0.10;RR=0.32,95%CI(0.16,0.63),P=0.001]after treated six months and twelve months. Conclusion Oral preparation of ginkgo biloba extract in the treatment of MCI clinical efficacy and prevention of dementia occurrence rate was better than that of blank control group.
MAGAKIS,MUELLERC,DICKSONC,et al.Increased production of inflammatory cytokines in mild cognitive impairment[J].Expgerontol,2007,42(3):233-240.
Recent studies indicate that chronic inflammation plays a pathogenic role in both the central nervous system (CNS) and periphery in Alzheimer's disease (AD). We have screened for cytokines differentially produced by peripheral blood mononuclear cells (PBMCs) isolated from subjects with mild cognitive impairment (MCI) and mild AD subjects who had progressed from MCI using a commercially available cytokine array. Following determination of expressed cytokines, we quantified levels of the proinflammatory cytokines TNF-alpha, IL-6, and IL-8, and the anti-inflammatory cytokine IL-10 using flow cytometry. We have found a significant increase in the levels of IL-6, IL-8, and IL-10 produced by PBMCs stimulated for 24 h with phytohemagglutinin (PHA) in MCI subjects compared to healthy elderly controls. However, in PBMCs stimulated for 48 h with lipopolysaccharide (LPS), lower TNF-alpha/IL-10, IL-6/IL-10, and IL-8/IL-10 ratios were seen in MCI subjects. There were no differences in plasma levels of IL-8 between aged controls, MCI, and mild AD, and the levels of circulating IL-6 and IL-10 were below detection limits. Our data indicate that changes in cytokine production by PBMCs may be detected early in MCI, and an alteration of the immune response may precede clinical AD.
Early identification of those at higher risk of dementia may play a part in secondary prevention and has received great clinical and research interest. Mild cognitive impairment (MCI) is a construct originally proposed to identify those who fall between normal cognitive aging and dementia. Clinical and research utility and validity of MCI are hotly debated. New MCI criteria proposed include the recent construct of mild neurocognitive disorder in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders, MCI criteria proposed by the National Institute on Aging-Alzheimer's Society and criteria elaborated by the International Working Group. This article aims to discuss whether these definitions provide clearer conceptualization of MCI and to highlight implications for research.
NIEH,XUY,LIUB,et al.The prevalence or mild cognitive impairment about elderly population in china:a meta-analysis[J].Int J Geriatr Psych,2011,26(6):558-563.
Dementia has been a major public health problem and mild cognitive impairment is considered the pre-dementia syndrome in recent years. However, there has not yet been a systematic analysis of the prevalence of mild cognitive impairment in China.The aim of this study was to analyse the prevalence of mild cognitive impairment among the population aged 60 years and older in China.Epidemiological investigations on mild cognitive impairment in China published in journals were identified manually and online by using CBMDISK, ChongqingVIP database and CNKI database. Those reported in English journals were identified using MEDLINE. Selected studies had to describe an original study defined by strict screening and diagnlstic criteria. The fixed effects model or random effects model was employed according to statistical test for homogeneity.Twenty-two studies were selected, the statistical information of which was collected for systematic analysis. The results showed that the pooled prevalence of MCI for the elderly population was 12.7% (95% CI: 9.7-16.5%). In eastern and western China, the prevalence of MCI was 9.6 and 14.7%, respectively. There was a higher prevalence of MCI in the illiterate elderly population than in those who received years of education.The prevalence of MCI affected by sex, age,education, which was lower in eastern than that in western China.
STEVENT,ANNETTEF,DIANEG,et al.The Ginkgo evaluation of memory(GEM) study :design and baseline data of a randomized trial of Ginkgo biloba extract in prevention of dementia[J].Contemp Clin Trials,2006,27(3):238-253.
The epidemic of late life dementia, prominence of use of alternative medications and supplements, and initiation of efforts to determine how to prevent dementia have led to efforts to conduct studies aimed at prevention of dementia. The GEM (Ginkgo Evaluation of Memory) study was initially designed as a 5-year, randomized double-blind, placebo-controlled trial of Ginkgo biloba , administered in a dose of 120 mg twice per day as EGb761, in the prevention of dementia (and especially Alzheimer's disease) in normal elderly or those with mild cognitive impairment. The study anticipates 8.5 years of participant follow-up. Initial power calculations based on estimates of incidence rates of dementia in the target population (age 75+) led to a 3000-person study, which was successfully recruited at four clinical sites around the United States from September 2000 to June 2002. Primary outcome is incidence of all-cause dementia; secondary outcomes include rate of cognitive and functional decline, the incidence of cardiovascular and cerebrovascular events, and mortality. Following screening to exclude participants with incident dementia at baseline, an extensive neuropsychological assessment was performed and participants were randomly assigned to treatment groups. All participants are required to have a proxy who agreed to provide an independent assessment of the functional and cognitive abilities of the participant. Assessments are repeated every 6months. Significant decline at any visit, defined by specific changes in cognitive screening scores, leads to a repeat detailed neuropsychological battery, neurological and medical evaluation and MRI scan of the brain. The final diagnosis of dementia is achieved by a consensus panel of experts. Side effects and adverse events are tracked by computer at the central data coordinating center and unblinded data are reviewed by an independent safety monitoring board. Studies such as these are necessary for this and a variety of other potential protective agents to evaluate their effectiveness in preventing or slowing the emergence of dementia in the elderly population.
HIGGINS J P T,GREEN S.Cochrane handbook for systematic reviews of interventions version 5.1.0 [EB/OL].The Cochrane Collaboration,2011(2011-03)[2015-1-4]..
HALILM,CANKURTARANM,YAVUZ BB,et al.No alteration in the PFA-100 in vitro bleeding time induced by the ginkgo biloba special,EGB761,in elderly patients with mild cognitive impairment[J].Blood Coagul Fibbin,2005,16(5):349-353.
EGb 761 is widely used in the management of mild cognitive impairment in the elderly population. Elucidation of the effects of EGb 761 on primary haemostasis via PFA-100 could represent an important step for better understanding of the haemostatic safety of EGb 761. The purpose of this prospective study is to assess the effects of Ginkgo biloba special extract, EGb 761, on PFA-100 in vitro bleeding time in elderly patients with mild cognitive impairment. A total of 40 elderly patients aged 65-79 years who were referred for geriatric assessment and who were diagnosed as having mild cognitive impairment were included. Patients were started on 80 mg EGb-761 three times daily. The complete set of PFA-100 in vitro bleeding time and coagulation parameters including prothrombin time, activated partial thromboplastin time and International Normalized Ratio were assessed before and on the seventh day of treatment with EGb 761. There was no statistically significant prolongation in PFA-100 in vitro bleeding time or coagulation parameters in patients receiving EGb 761 after 7 days. The data about the safety of EGb 761 from the point of primary haemostasis in our elderly patient population with mild cognitive impairment casts hope for the future management of this 'difficult-to-treat' population with the promising Ginkgo extracts.
GAVRILOVA SI,PREUSS UW,WONG J W M,et al.Efficacy and safety of Ginkgo biloba extract EGB761 in mild cognitive impairment with neuropsychiatric symptoms:a randomized,placebo-controlled,double-blind,multi-center trial[J].Int J Geriatr Psych,2014,29(10):1087-1095.
The study was conducted to explore the effects of EGb 761 (Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany) on neuropsychiatric symptoms (NPS) and cognition in patients with mild cognitive impairment (MCI).One hundred and sixty patients with MCI who scored at least 6 on the 12-item Neuropsychiatric Inventory (NPI) were enrolled in this double-blind, multi-center trial and randomized to receive 24065mg EGb 761 daily or placebo for a period of 2465weeks. Effects on NPS were assessed using the NPI, the state sub-score of the State-Trait Anxiety Inventory and the Geriatric Depression Scale. Further outcome measures were the Trail-Making Test (A/B) for cognition and global ratings of change. Statistical analyses followed the intention-to-treat principle.The NPI composite score decreased by 7.065±654.5 (mean, standard deviation) points in the EGb 761-treated group and by 5.565±655.2 in the placebo group (p65=650.001). Improvement by at least 4 points was found in 78.8% of patients treated with EGb 761 and in 55.7% of those receiving placebo (p65=650.002). Superiority of EGb 761 over placebo (p65<650.05) was also found for the State-Trait Anxiety Inventory score, the informants' global impression of change, and both Trail-Making Test scores. There were statistical trends favoring EGb 761 in the Geriatric Depression Scale and the patients' global impression of change. Adverse events (all non-serious) were reported by 37 patients taking EGb 761 and 36 patients receiving placebo.EGb 761 improved NPS and cognitive performance in patients with MCI. The drug was safe and well tolerated.
TAN MS,YU JT,TAN CC,et al.Efficacy and adverse effects of ginkgo biloba for cognitive impairment and aementia:a systematic review and meta-analysis[J].JAD,2015,43(2):589-603.
[本文引用:1]
Increased production of inflammatory cytokines in mild cognitive impairment
Efficacy and safety of Ginkgo biloba extract EGB761 in mild cognitive impairment with neuropsychiatric symptoms:a randomized,placebo-controlled,double-blind,multi-center trial

 , 黎红丹
, 黎红丹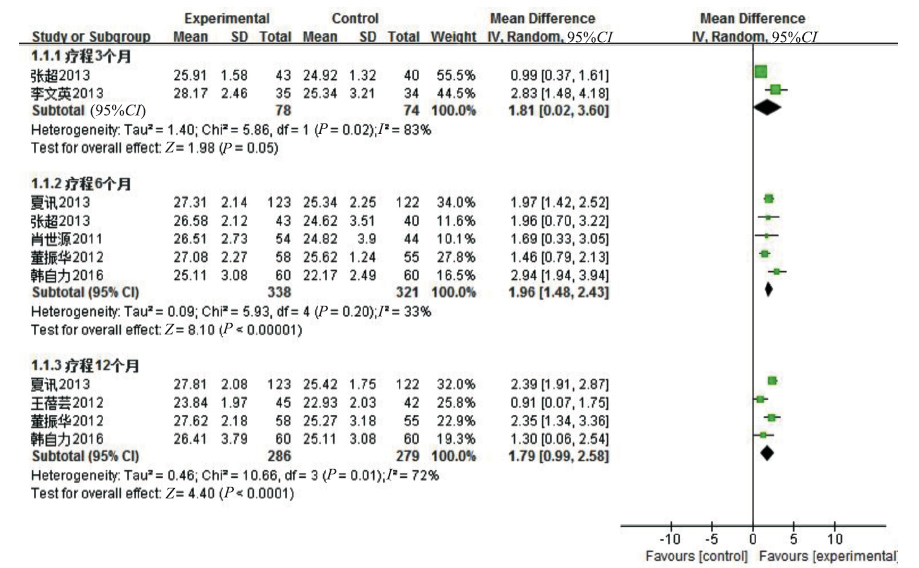


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}