Objective To investigate the clinical distribution of Streptococcus pneumoniae and its drug resistance to commonly used antibiotics and provide reference for clinical reasonable selection of antibiotics. Methods Retrospective analysis of the distribution of Streptococcus pneumoniae isolated in Tongji hospital affiliated to Tongji medical college Huazhong university of science and technology during 2011 to 2016 was carried out.Drug susceptibility test was conducted by K-B method except for penicillin and cefatriaxone by E-test method. Results A total of 1 046 strains of Streptococcus pneumonia were isolated from specimens in hospital during 2011 to 2016,among them 300 strains were from adults patients and the other 746 strains were from children patients.Sputum was the most common specimen type and its ratio was 62.3% in adults group,90.5% in children group.Totally,59.6% of the strains were from department of pediatrics.The antibiotics sensitivity results showed that the resistance rate of the isolates to erythromycin and clindamycin was higher in adults and children,more than 85.0%.The susceptible rates of penicillin (non-meningitis break point),moxifloxacin,levofloxacin and vancomycin were higher than 80.0%. Conclusion In the hospital the isolates of Streptococcus pneumonia is mainly from respiratory specimens and the resistance rate to erythromycin and clindamycin was higher.Erythromycin and clindamycin are not suitable for the treatment of Streptococcus pneumoniae infection.Clinicians should select antibiotics according to the results of drug sensitivity.
采用纸片扩散法进行,质控菌株ATCC25922,25923,27853,35218,700603每周做一次室内质控,药敏纸片均为英国OXOID公司产品,药敏试验操作及折点判读均采用临床实验室标准化协会(Clinical and Laboratory Standards Institute,CLSI)2016年标准[1]。青霉素和头孢曲松采用E试验,E试验条为英国OXOID公司产品。
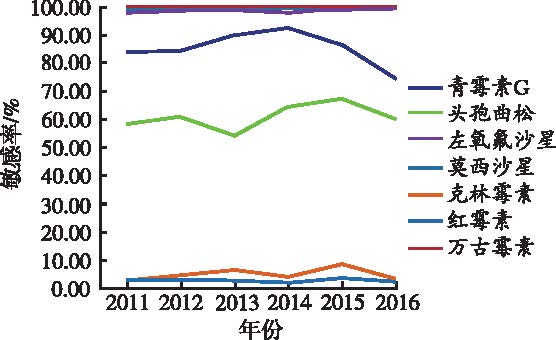
分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%。感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者。儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群。我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型。药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%。但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率。青霉素按照CLSI的判读标准,有3种折点。口服青霉素折点、脑膜炎折点和非脑膜炎折点。此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大。所以按照非脑膜炎折点进行判读,结果较可靠。按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择。头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用。因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗。2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势。肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动。重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6]。近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜。研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E)。黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7]。而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8]。国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9]。国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10]。本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究。预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施。来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11]。儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14]。本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中。鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染。
The authors have declared that no competing interests exist.
Clinical and Laboratory StandardsInstitute.2016.Performance standards for antimicrobial susceptibility testing :26th informational supplement,M100-S26[S].Clin Lab Stan Ins,Wayne,PA.
MEHLA,ASVOLD BO,LYDERSENS,et al.Burden of bloodstream infection in an area of Mid-Norway 2002-2013:a prospective population-based observational study[J].BMC Infect Dis,2017,17(1):205-208.
Studies from several countries indicate that the incidence and mortality of bloodstream infection (BSI) have been increasing over time. We studied the burden of disease and death related to BSI in a defined geographical area of Mid-Norway, where BSI episodes were prospectively recorded by the same microbiological department during 12 consecutive years. Death from BSI was defined as death within 3002days of BSI detection. Age and sex standardized incidence and mortality rates and case fatality rates were calculated. Between 2002 and 2013, 1995 episodes of BSI in 1719 patients aged 16 to 9902years were included. The overall incidence of BSI was 215 per 100,000 person-years. The incidence increased exponentially with age, particularly in males. The incidence increased from 205 to 223 per 100,000 person-years from 2002–07 to 2008–13.Escherichia coliwas the most frequently isolated infective agent, followed byStreptococcus pneumoniaeandStaphylococcus aureus. The rate ofS. pneumoniaeBSI decreased over time in males (on average by 9.2% annually), but not in females. The total rate of BSI microbes with acquired resistance increased slightly over time, but did not exceed 2 episodes per 100,000 person-years. The mortality of BSI was 32 per 100,000 person-years, higher in males than in females (36 vs. 28 per 100,000 person-years) and was significantly higher in old age, particularly in males. The total BSI mortality was similar in the first and second halves of the study period, but the mortality ofS. pneumoniaeBSI decreased in males (15.0% annually). The crude case fatality decreased from the first to the second half of the study period (17.2% to 13.1%;p65=0.014). The rate of blood culture sampling increased more than twofold during the study period. The mortality of BSI remained stable during 2002–2013. At the same time, BSI incidence increased and case fatality rate decreased, perhaps because an increased rate of blood culture sampling may have led to improved detection of milder BSI episodes. Very low, yet slightly increasing rates of microbes with acquired resistance were observed. The online version of this article (doi:10.1186/s12879-017-2291-2) contains supplementary material, which is available to authorized users.
GERGOVA RT,PETROVAG,GERGOVS,et al.Microbiological features of upper respiratory tract infections in bulgarian children for the period 1998-2014[J].Balkan Med J,2016,33(6):675-680.
Abstract BACKGROUND: Across the globe, upper respiratory tract infections (URTIs) are the most prevalent cause of morbidity in childhood. AIMS: The aim of our study is to analyze the incidence and etiology of bacterial URTIs in Bulgarian children, as well as the increasing antimicrobial resistance to the most common etiologic agents over a period of 17 years. STUDY DESIGN: Retrospective study. METHODS: The study material comprised the data from 4768 patients (aged 1-16 years) with URTI during the period from 1998-2014. Specific microbiology agent detection was performed by culture examination. Susceptibilities to the investigated pathogens were determined by the disk diffusion method and minimal inhibitory concentration according to the criteria of the Clinical and Laboratory Standards Institute (CLSI). Polymerase chain reaction was used to detect the presence of 尾-lactam resistance genes. RESULTS: We identified the following as the most common URTI bacterial pathogens: Streptococcus pneumoniae (40.94%), Streptococcus pyogenes (34.16%), Haemophilus influenzae (44.23%), Moraxella catarrhalis (39.19%) and Staphylococcus aureus (23.88%). In more than 70% of cases, a polymicrobial etiology was found. The most commonly affected individuals were pre-school-aged children, which accounted for more than 36% of all patients. During the study period, a dramatic increase in resistance to antibiotic agents was observed. The most frequent types of resistance were the enzymatic inactivation of penicillins and cephalosporins (close to 100% in staphylococci and moraxellae) and inducible macrolide-lincozamide resistance (about 20% of Gram-positive cocci). CONCLUSION: Due to mandatory immunization against pneumococci and H. influenzae in Bulgaria and the vast expanding resistance to the most popular antimicrobial agents changes in the etiology of URTI have recently been noted. Regular analysis of this etiological dynamic and the antimicrobial resistance of respiratory pathogens is important for choosing the correct therapy and successful treatment.
EL ASHKARS,OSMANM,RAFEIR,et al.Molecular detection of genes responsible for macrolide resistance among Streptococcus pneumoniae isolated in North Lebanon[J].J Infect Pub Health,2017,10(6):745-748.
In recent years, the increased use of macrolides was linked with the emergence of resistance Streptococcus pneumoniae worldwide. The main aim of this study was to determine the prevalence of S. pneumoniae resistant to macrolides and to identify the macrolide resistance genotypes among clinical isolates collected in North Lebanon. Disk diffusion susceptibility method was performed for 132 strains of S. pneumoniae isolated over a period of 5 years in North Lebanon. Polymerase Chain Reaction followed by pyrosequencing was carried out for confirmation of phenotypic diagnosis. The macrolide resistance genotypes were also identified by using PCR amplification of genes implicated in this resistance: erm (A), erm (B), erm (C), msr (A), lin (A) and mef (A/E). Macrolide resistance was found in 34.1% of S. pneumoniae isolates. We observed that the cMLS B phenotype (31/45, 68.9%) was the most common in these pneumococci and erm (B) was the most common resistance gene (32/45, 71.1%). This study shows that macrolide resistance in S. pneumoniae in North Lebanon is mainly related to target site modification with predominance of cMLSb phenotype but is also mediated by efflux pumps. lin (A) gene was reported for the first time in one S. pneumoniae strain in combination with erm (B) and mef (A/E) genes.
CARDOSO NT,SANTOS BA,BARBOSA AV,et al.Serotypes,antimicrobial resistance and genotypes of Streptococcus pneumoniae associated with infections in cancer patients in Brazil[J].Diag Micr Inf Dis,2017,87(3):281-285.
Abstract We sought to characterize pneumococcal isolates associated with bacteremia, pneumonia and meningitis in cancer patients and to estimate the coverage of the available pneumococcal vaccines. Fifty isolates recovered from 49 patients attending a cancer reference center over a 1-year period were analyzed. The prevalent serotypes were: 23F (12%), 6A (8%), 3, 4, 20, and 23A (6% each). All isolates were susceptible to chloramphenicol, levofloxacin, rifampicin, and vancomycin. Resistance or reduced susceptibility to penicillin made up 14%, and one isolate was also intermediately resistant to ceftriaxone. The three (6%) erythromycin-resistant isolates presented the M or cMLS B phenotypes and harbored the mef(A/E) gene exclusively or along with the erm(B) gene. Twenty-two (44%) isolates were closely related to 11 international clones, being strongly associated with penicillin non-susceptibility. Combined immunization with the 13-valent conjugate and the 23-valent polysaccharide vaccines might contribute to reduce (76%) the burden of the pneumococcal infections in the population investigated. Copyright 脗漏 2016 Elsevier Inc. All rights reserved.
KOBAYASHIM,CONKLIN LM,BIGOGOG,et al.Pneumococcal carriage and antibiotic susceptibility patterns from two cross-sectional colonization surveys among children aged <5 years prior to the introduction of 10-valent pneumococcal conjugate vaccine - Kenya,2009-2010[J].BMC Infect Dis,2017,17(1):25-29.
BACKGROUND: Pneumococci are spread by persons with nasopharyngeal colonization a necessary precursor to invasive disease. Pneumococcal conjugate vaccines can prevent colonization with vaccine serotype strains. In 2011 Kenya became one of the first African countries to introduce the 10-valent pneumococcal conjugate vaccine (PCV10) into its national immunization program. Serial cross-sectional colonization surveys were conducted to assess baseline pneumococcal colonization antibiotic resistance patterns and factors associated with resistance. METHODS: Annual surveys were conducted in one urban and one rural site during 2009 and 2010 among children aged /=1 antibiotics (i.e. penicillin chloramphenicol levofloxacin erythromycin tetracycline cotrimoxazole and clindamycin); multidrug resistance (MDR) was defined as nonsusceptibility to >/=3 antibiotics. Weighted analysis was conducted when appropriate. Modified Poisson regression was used to calculate factors associated with antibiotic nonsusceptibility. RESULTS: Of 1087 enrolled (Kibera: 740 Lwak: 347) 90.0% of these were colonized with pneumococci and 37.3% were colonized with PCV10 serotypes. There were no differences by survey site or year. Of 657 (of 730; 90%) isolates tested for antibiotic susceptibility nonsusceptibility to cotrimoxazole and penicillin was found in 98.6 and 81.9% of isolates respectively. MDR was found in 15.9% of isolates and most often involved nonsusceptibility to cotrimoxazole and penicillin; 40.4% of MDR isolates were PCV10 serotypes. In the multivariable model PCV10 serotypes were independently associated with penicillin nonsusceptibility (Prevalence Ratio: 1.2 95% CI 1.1-1.3) but not with MDR. CONCLUSIONS: Before PCV10 introduction nearly all Kenyan children aged <5 years were colonized with pneumococci and PCV10 serotype colonization was common. PCV10 serotypes were associated with penicillin nonsusceptibility. Given that colonization with PCV10 serotypes is associated with greater risk for invasive disease than colonization with other serotypes successful PCV10 introduction in Kenya is likely to have a substantial impact in reducing vaccine-type pneumococcal disease and drug-resistant pneumococcal infection.
SAID WF,SUKOTOE,KHOERI MM,et al.Serotype distribution and antimicrobial susceptibility of Streptococcus pneumoniae isolates from adult patients in Jakarta,Indonesia[J].J Infec Publ Heal,2017,10(6):833-835.
Currently, the data on pneumococcal invasive disease in the Indonesian population are limited. In this study, we investigated the serotype distribution and antimicrobial susceptibility ofStreptococcus pneumoniae.These samples were isolated from the sputum of adult patients with non-specific clinical symptoms aged 18鈥87 years in Jakarta, Indonesia, from August to October 2014. Of the 349 sputum specimens, thirteen isolates were identified asS. pneumoniaestrains (4%), with two strains each for serotype 19F, 3, and 15A, and one strain each for serotype/serogroup 13, 23A, 6, 34, 17F, 16F, and untypeable. Resistance to tetracycline was most common with only 5 of 13 strains being susceptible. In conclusion, these data provide an initial in the surveillance of invasive pneumococcus in the Indonesia population.
OUSMANES,DIALLO BA,OUEDRAOGOR,et al.Serotype distribution and antimicrobial sensitivity profile of Streptococcus pneumoniae carried in healthy toddlers before PCV13 Introduction in Niamey,Niger[J].PLoS One,2017,12(1):e0169547.
To mitigate the burden of pneumococcal infections in Niger, a 13-valent pneumococcal vaccine, PCV13, was introduced for routine child vaccination in July 2014. In order to provide pre-vaccine baseline data and allow appreciation of changes on carriage due to vaccination, we analyzed retrospectively pneumococcal isolates obtained from healthy, 0 to 2 year old children prior to the vaccine introduction. From June 5, 2007, to May 26, 2008, 1200 nasopharyngeal swabs were collected from healthy 0 to 2 year old children and analyzed by standard microbiological methods. Serotyping was done by SM-PCR and the data were analyzed with R version 2.15.0 (2012-03-30). Streptococcus pneumoniaewas detected in 654/1200 children (54.5%) among whom 339 (51.8%) were males. The ages of the study subjects varied from few days to 26 months (mean = 7.1, median = 6, 95% CI [6.8鈥7.4]). Out of 654 frozen isolates, 377 (54.8%) were able to be re-grown and analyzed. In total, 32 different serogroups/serotypes were detected of which, the most prevalent were 6/(6A/6B/6C/6D) (15.6%), 23F (10.6%), 19F (9.3%), 14 (9%), 19A (5.6%), 23B (4.0%), 25F/38 (3.7%), 18/(18A/18B/18C/18F) (2.9%) and PCR non-typeable (16.4%). Eleven serogroups/serotypes accounting for 57.3% (216/377) were of PCV13 types. Of the 211/377 (56%) isolates tested for drug sensitivity, 23/211 (10.9%), 24/211 (11.4%), 9/211(4.3%) and 148/210 (70.5%) were respectively resistance to oxacillin, chloramphenicol, erythromycin and tetracycline. Thirteen of the oxacillin resistant isolates were additionally multidrug-resistant. No resistance was however detected to gentamycin500渭gand to fluoroquinolones (酶 Norfloxacin5渭g<7mm). Age > 3 months and presence in family of more than one sibling aged < 6 years were significant risk factors for carriage. A global rate of 54.5% pneumococcal carriage was detected in this study. The introduced PCV13 vaccine should cover 57.3% (216/377) of circulating serogroups/serotypes, among which were those resistant to antibiotics. Age > 3 months and presence in family of children aged < 6 years were significant factors for pneumococcal carriage. The present data should help understanding post vaccine introduction changes in pneumococcal carriage and infections for better action.
MANOHARANA,MANCHANDAV,BALASUBRAMANIANS,et al.Invasive pneumococcal disease in children aged younger than 5 years in India:a surveillance study[J].Lanc Infect Dis,2017,17(3):305-312.
Invasive pneumococcal disease continues to be a major cause of morbidity and mortality among children younger than 5 years of age in India. We aimed to provide nationally representative data for the pattern of disease due toStreptococcus pneumoniae, trends in the serotype of invasive pneumococci, and invasive pneumococci antimicrobial resistance patterns, in India. In this prospective hospital-based and retrospective laboratory-based surveillance study, we prospectively enrolled children aged younger than 5 years with suspected or proven invasive pneumococcal disease from 18 hospitals or institutional centres and retrospectively included laboratory-confirmed pneumococcal isolates from ten sentinel laboratories, together representing 11 states in India. Eligibility criteria were fever higher than 38掳C without localising symptoms, clinical presentation of suspected meningitis or pneumonia, and evidence of radiographic pneumonia. We cultured blood and other normally sterile body fluids, reconfirmed and serotyped pneumococcal isolates, and established antimicrobial susceptibility using standard study protocols. Between Jan 1, 2011, and June 30, 2015, we enrolled 4377 patients. Among 361 (8%) patients with culture-proven pneumococcal disease, all clinical data were known for 226 (63%); among these patients, 132 (58%) presented with pneumonia, 78 (35%) presented with meningitis, and 16 (7%) had other clinical conditions. 131 (3%) died overall and 29 (8%) patients with invasive pneumococcal disease died. Serotypes 14 (52 [14%] of 361), 1 (49 [14%]), 5 (37 [10%]), and 19F (33 [9%]) were the most common. Penicillin non-susceptibility occurred in isolates from 29 (8%) patients, co-trimoxazole resistance occurred in 239 (66%), erythromycin resistance occurred in 132 (37%), and chloramphenicol resistance occurred in 33 (9%). We found multidrug resistance in 33 (9%) of 361 patients. The proportion of positive blood cultures, number of isolates, geographical representation, and data generated over the 4路5 years of the study are representative of data for most of India. Continued surveillance is warranted as the decision to introduce protein conjugated vaccine in India is made. GlaxoSmithKline India.
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Molecular detection of genes responsible for macrolide resistance among isolated in North Lebanon
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Serotypes,antimicrobial resistance and genotypes of associated with infections in cancer patients in Brazil
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
2012至2014年山西省儿童医院住院部肺炎链球菌分离株耐药性分析
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
接受连续性静脉-静脉血液滤过患者左氧氟沙星抗感染方案的优化
1
2016
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Pneumococcal carriage and antibiotic susceptibility patterns from two cross-sectional colonization surveys among children aged <5 years prior to the introduction of 10-valent pneumococcal conjugate vaccine - Kenya,2009-2010
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Serotype distribution and antimicrobial susceptibility of isolates from adult patients in ,
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Serotype distribution and antimicrobial sensitivity profile of carried in healthy toddlers before PCV13 Introduction in Niamey,Niger
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...
Invasive pneumococcal disease in children aged younger than 5 years in India:a surveillance study
1
2017
... 分离株的科室分布显示,我院分离的肺炎链球菌主要来自儿科,占59.6%,其次为呼吸科,占7.6%.感染人群年龄的分布,儿童患者占71.3%,表明我院分离的肺炎链球菌主要来自儿童患者.儿童由于自身的免疫力和对病原菌的抵抗力均弱于成人,所以儿童是肺炎链球菌的主要感染人群.我院分离的肺炎链球菌主要来自呼吸道标本,呼吸道感染是肺炎链球菌的主要感染类型.药敏监测数据显示,成人组和儿童组的分离株对喹诺酮类药物,莫西沙星和左氧氟沙星均保持了极高的敏感性,敏感率均超过98.0%.但对红霉素和克林霉素,两组患者耐药率均高于89.0%,对万古霉素均保持了100.0%的敏感率.青霉素按照CLSI的判读标准,有3种折点.口服青霉素折点、脑膜炎折点和非脑膜炎折点.此次的监测数据显示,分离自脑脊液的标本在成人组和儿童组中的比例分别为1.3%和0.7%,故按照脑膜炎折点判读,偏差较大.所以按照非脑膜炎折点进行判读,结果较可靠.按照非脑膜炎折点判读,青霉素的敏感率在成人组和儿童组均高于80.0%,且青霉素价格低廉,不良反应少,表明青霉素依然是肺炎链球菌感染的最佳选择.头孢曲松的敏感率在成人组和儿童组的分离株之间存在较大差异,在成人组敏感率为71.9%,而儿童组为56.5%,差异的原因可能与头孢曲松在儿童患者中使用广泛引起的选择性压力有关,很多抗生素如喹诺酮类和氨基苷类等由于不良反应不适合儿童患者使用.因此头孢曲松做为青霉素的补充治疗药物,若患者对青霉素过敏,临床医师可根据药敏结果合理使用头孢曲松进行治疗.2011—2016年我院的监测数据显示,肺炎链球菌的敏感率无明显变化趋势.肺炎链球菌对为莫西沙星、左氧氟沙星和万古霉素几乎为100.0%敏感,青霉素的敏感率在70%~100%,头孢曲松在50%~70%,而红霉素和克林霉素均在0%~10%之间波动.重庆地区2009—2014年肺炎链球菌的药敏监测数据显示,肺炎链球菌对常用抗菌药物的药敏结果也没有显著性的变化趋势,可能与每个地区长期比较稳定的用药习惯有关[6].近年来,由于大环内酯类药物的广泛使用,肺炎链球菌对大环内酯类药物产生耐药性的报道屡见不鲜.研究表明,肺炎链球菌对大环内酯类抗菌药物耐药性的产生主要是因为耐药基因的表达,如erm(A),erm(B),erm(C),msr(A),lin(A) and mef(A/E).黎巴嫩5年的一项研究显示,erm(B)是肺炎链球菌对大环内酯类抗菌药物的主要耐药机制[7].而来自巴西的一项研究显示,mef A/E和erm(B)是肺炎链球菌对红霉素的主要耐药基因[8].国内的研究报道,来自山西儿童医院住院儿童超过95%的肺炎链球菌分离株对万古霉素、利奈唑胺、左氧氟沙星、青霉素、头孢曲松、头孢噻肟的敏感率均高于75%,<20%患儿的肺炎链球菌对红霉素、克林霉素和四环素敏感[9].国内外的研究数据均表明肺炎链球菌对大环内酯类药物的耐药现象较严重[10].本地区肺炎链球菌对大环内酯类抗菌药物耐药机制的报道较少,期待日后进行更深入的研究.预防儿童感染肺炎链球菌,接种疫苗是一项非常有效的措施.来自肯尼亚的研究数据显示,90%的5岁以下儿童呼吸道均定植了肺炎链球菌,且对磺胺类药物和青霉素的耐药率均超过了80%[11].儿童鼻咽部肺炎链球菌的定植率,不同国家地区有不同的报道,如印度5岁以下儿童为8%,尼日尔2岁以下儿童的携带率高达54.5%,可能与不同国家的疫苗接种率不同有关[12,13,14].本地区关于肺炎链球菌的携带率报道的数据非常有限,目前世界上许多国家已经将肺炎链球菌疫苗列入国家的免疫计划中,但中国还未将其列入其中.鉴于此次的数据分析和全球不同地区对肺炎链球菌的携带率及高耐药现象的报道,希望更多的儿童去接种肺炎链球菌疫苗,远离或避免肺炎链球菌引起的呼吸道感染. ...

 , 田磊, 陈中举, 管青
, 田磊, 陈中举, 管青
{kind=link}
{kind=link}