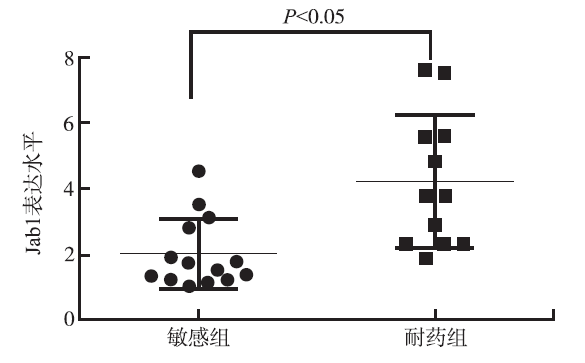
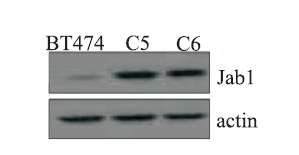
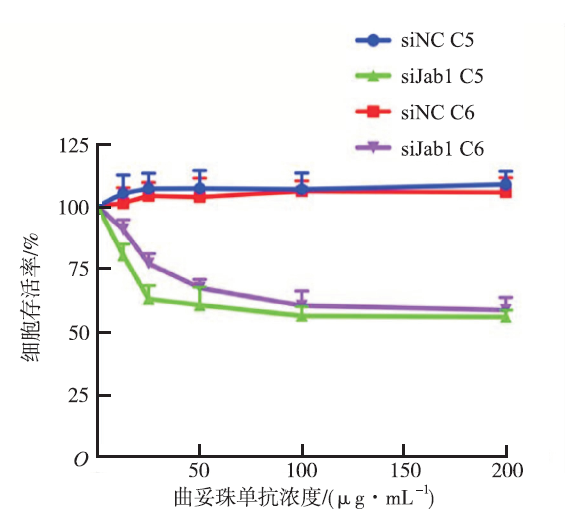
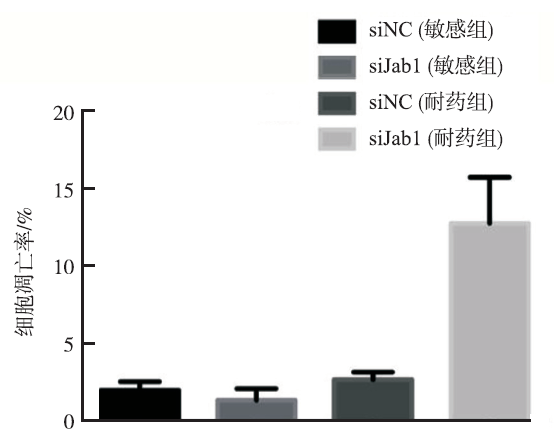
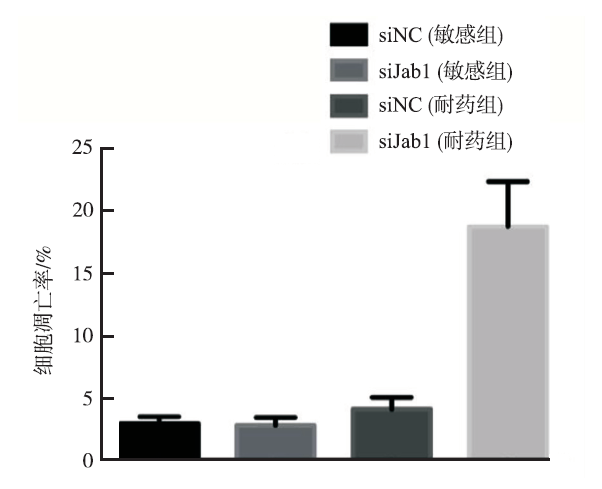
Objective To investigate the effect of Jab1 on trastuzumab (Ttzm) treatment sensitivity in HER2 positive breast cancer. Methods q-PCR was performed to detect the expression of Jab1 in 26 HER2 positive breast cancer patient with Ttzm treatment 14 patients were sensitive to Ttzm, while 12 patients were were Ttzm-resistant. The expression of Jab1 was examined by Western blotting in Ttzm-sensitive and resistant breast cancer cell lines. With the knockdown of Jab1 by siRNA, the sensitivity to the drug and the Ttzm-induced apoptosis were measured in related cell lines. Results The expression of Jab1 in Ttzm resistant breast cancer patient was significantly higher than these Ttzm sensitive patient(P<0.05). In Ttzm-sensitive breast cancer cell line C5 and C6, the expression of Jab1 was significantly lower than that in the Ttzm-resistant cells. After konckdown of Jab1 in Ttzm-resistant cells, C5 and C6 cells were re-sensitive to the Ttzm treatment, and the Ttzm-induced apoptosis was observed to be more obvious. In C5 cell line, after 24 hours of Ttzm treatment, the apoptotic rates in Jab1 knockdown group and the control group were (12.8±2.9)% and (2.7±0.5)%(P<0.05), while in the C6 cell line, the apoptosic rates were (18.8±3.6)% and (4.1±1.1)%(P<0.05), respectively. Conclusion Up-regulated expression of Jab1 is associated with the reduction of Ttzm treatment sensitivity in breast cancer cells. Knockdown of Jab1 might be a potential mechanism to antagonize the Ttzm-resistance.
Key words:
Jab1
;
Trastuzumab
;
Drug resistance
;
Breast cancer
;
Human epidermal growth factor receptor-2
DI COSIMOS,BASELGAJ.Management of breast cancer with target agents:importance of heterogeneity[J].Nat Rev Clin Oncol,2010,7(3):139-147.
Breast cancer is a heterogeneous disease with different molecular drivers regulating its growth, survival and response to therapy. Breast cancer is divided in three major subtypes based on the pattern of expression of hormone receptors and HER2: luminal tumors (or HR positive), HER2 amplified tumors, and the remaining subtypes being collectively referred to as triple-negative breast cancer. While tumors within these subtypes have similar gene-expression patterns, clinical outcomes, and response to therapy, this division is far from perfect and subgroups within these groups are beginning to be identified. In terms of therapy, an increasingly rational drug development effort has resulted in agents against new molecular targets that are active against only those tumors with the targeted molecular alteration or phenotype. These agents include receptor and non-receptor tyrosine kinase inhibitors (HER1, HER2, HER3, insulin-like growth factor receptor, c-met, fibroblast growth factor receptor and HSP 90 inhibitors), intracellular signaling pathways (PI3K, AKT, mTOR), angiogenesis inhibitors and agents that interfere with DNA repair (PARP inhibitors). Thus, the overall management of breast cancer will increasingly require an understanding of breast cancer heterogeneicity, the biological nature of any given tumor as well the existence of increased personalized treatment options.
YARDENY,PINESG.The ERBB network:at last,cancer therapy meets systems biology[J].Nat Rev Caner,2012,12(4):553-563.
Although it is broadly agreed that the improved treatment of patients with will depend on a deeper molecular understanding of the underlying , only a few examples are already available. This Timeline article focuses on the (also known as HER) network of receptor tyrosine kinases (RTKs), which exemplifies how a constant dialogue between basic research and medical oncology can translate into both a sustained pipeline of novel drugs and ways to overcome acquired treatment resistance in patients. We track the key early discoveries that linked this RTK family to , the course of pioneering clinical research and their merger into a systems-biology framework that is likely to inspire further generations of effective therapeutic strategies.
LI CI,URIBE DJ,DALING JR.Clinical characteristics of different histologic types of breast cancer[J].Br J Cancer,2005,93(8):1046-1052.
Breast cancer is a heterogeneous disease, though little is known about some of its rarer forms, including certain histologic types. Using Surveillance, Epidemiology, and End Results Program data on 13565157 invasive breast cancer cases diagnosed from 1992 to 2001, relationships between nine histologic types of breast cancer and various tumour characteristics were assessed. Among women aged 50–89 years at diagnosis, lobular and ductal/lobular carcinoma cases were more likely to be diagnosed with stage III/IV, 825.065cm, and node-positive tumours compared to ductal carcinoma cases. Mucinous, comedo, tubular, and medullary carcinomas were less likely to present at an advanced stage. Lobular, ductal/lobular, mucinous, tubular, and papillary carcinomas were less likely, and comedo, medullary, and inflammatory carcinomas were more likely to be oestrogen receptor (ER) negative/progesterone receptor (PR) negative and high grade (notably, 68.2% of medullary carcinomas were ER61/PR61 vs 19.3% of ductal carcinomas). In general, similar differences were observed among women diagnosed at age 30–49 years. Inflammatory carcinomas are associated with more aggressive tumour phenotypes, and mucinous, tubular, and papillary tumours are associated with less aggressive phenotypes. The histologic types of breast cancer studied here differ greatly in their clinical presentations, and the differences in their hormone receptor profiles and grades point to their likely different aetiologies.
SLAMON DJ,LEYLB,JONESS,et al.Use of chemothera-py plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2[J].N Engl J Med,2001,344(11):783-792.
YEON CH,PEGRAM MD.Anti-erbB-2 antibody trastuzu-mab in the treatment of HER2-amplified breast cancer[J].Inv New Drugs,2005,23(3):391-409.
Human epidermal growth factor receptor-2 (HER2/erbB-2) is a member of a family of four transmembrane receptor tyrosine kinases that regulate cell growth, survival and differentiation via multiple signal transduction pathways. Amplification of the HER2 gene occurs in 20 25% of human breast cancers. This amplification event is an independent adverse prognostic factor as well as a predictive factor for increased response to doxorubicin-based combination chemotherapy, response to trastuzumab and decreased response to hormonal therapy. Methods for detecting protein overexpression or gene amplification in clinical tumor specimens include immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) techniques, with the latter considered by some to be more accurate. Trastuzumab (Herceptin) is a recombinant humanized monoclonal antibody which targets an epitope in the extracellular domain of the HER2 protein. Preclinical models demonstrated that this antibody has significant anti-tumor activity as a single agent and has synergy with certain chemotherapeutic drugs. Phase II and III clinical trials performed in women with metastatic breast cancer that overexpress HER2 have shown that trastuzumab has clinical activity when used as first-, second- or third-line monotherapy, and improves survival when used as first-line therapy in combination with chemotherapy. Newer combinations with numerous chemotherapeutic drugs have also shown significant clinical activity in phase II studies. In all of these trials, trastuzumab was generally well-tolerated, but cardiac toxicity (particularly when the antibody was combined with anthracyclines) was an unexpected adverse effect. Although trastuzumab is currently usually administered on a weekly intravenous schedule, evidence suggests that a triple dose of the drug given once every three weeks has a pharmacokinetic profile expected to be equally efficacious. Neither the optimal schedule nor the optimal duration of trastuzumab therapy has yet been clearly defined in controlled clinical trials. Current clinical investigations of trastuzumab include its use in both the adjuvant and neoadjuvant settings as well as in combination with other chemotherapy drugs or new biologic targeted agents.
ARTEAGA CL,SLIWKOWSKI MX,OSBORNE CK,et al.Treatment of HER2-positive breast cancer:current status and future perspectives[J].Nat Rev Clin Oncol,2012,9(1):16-32.
The advent of HER2-directed therapies has significantly improved the outlook for patients with HER2-positive early stage breast cancer. However, a significant proportion of these patients still relapse and die of breast cancer. Trials to define, refine and optimize the use of the two approved HER2-targeted agents (trastuzumab and lapatinib) in patients with HER2-positive early stage breast cancer are ongoing. In addition, promising new approaches are being developed including monoclonal antibodies and small-molecule tyrosine kinase inhibitors targeting HER2 or other HER family members, antibodies linked to cytotoxic moieties or modified to improve their immunological function, immunostimulatory peptides, and targeting the PI3K and IGF-1R pathways. Improved understanding of the HER2 signaling pathway, its relationship with other signaling pathways and mechanisms of resistance has also led to the development of rational combination therapies and to a greater insight into treatment response in patients with HER2-positive breast cancer. Based on promising results with new agents in HER2-positive advanced-stage disease, a series of large trials in the adjuvant and neoadjuvant settings are planned or ongoing. This Review focuses on current treatment for patients with HER2-positive breast cancer and aims to update practicing clinicians on likely future developments in the treatment for this disease according to ongoing clinical trials and translational research.
THUY VU,SLIWKOWSKI MX,CLARET FX.Personali-zed drug combinations to overcome trastuzumab resistance in HER2-positive breast cancer[J].Biochim Biophysica Acta,2014,10(3):353-365.
[本文引用:1]
[8]
MARIA LC,PAULA GT,YOLANDA FP,et al.Mechan-isms behind the resistance to trastuzumab in HER2-amplied breast cancer and strategies to overcome it[J].Clin Med Ins:Oncol,2016,10(Suppl 1):21-30.
Purpose of review: This review discusses the mechanisms of anti-human epidermal growth factor receptor 2 (HER2) resistance in breast cancer patients, detailing possible predictive biomarkers of therapy benefit that could implement novel therapeutic strategies. Recent findings: Despite a remarkable improvement in survival over the past two decades, up to 30% of early-stage HER2+ breast... [Show full abstract]
HSU MC,CHANG HC,HUNG WC.HER-2/neu transcrip-tionally activates Jab1 expression via the AKT/beta-catenin pathway in breast cancer cells[J].Endocr Relat Cancer,2007,14(3):655-667.
Jab1 is a co-activator of activating protein-1 (AP-1) transcription factor and the fifth subunit of the constitutive photomorphogenesis 9 (COP9) signalosome, which has been shown to mediate nuclear exportation and ubiquitin-dependent degradation of the tumor suppressor p27(Kip1). Jab1 is overexpressed in several types of human cancer. However, de-regulation of Jab1 gene expression in cancer cells is largely unclear. In this study, we reported that expression of Jab1 was stimulated by HER-2/neu oncogene via transcriptional activation. Promoter deletion and mutation analysis indicated that HER-2/neu stimulated Jab1 via the T cell factor (TCF) binding site located at the -380/-368 region of the human Jab1 promoter. DNA affinity precipitation assay and chromatin immunoprecipitation assay verified that binding of beta-catenin and TCF-4 to this consensus site was increased by HER-2/neu. In addition, dominant-negative mutant of TCF significantly attenuated the stimulatory effect of HER-2/neu. We also demonstrated that HER-2/neu increased beta-catenin/TCF-mediated Jab1 expression via the AKT signaling pathway because chemical inhibitor or dominant-negative mutant of AKT effectively attenuated the stimulatory action of HER-2/neu. IGF-I, which is a well-known AKT activator, also up-regulated the expression of Jab1 in NIH/3T3 and MCF-7 cells. Knockdown of Jab1 by small interfering RNA (siRNA) preferentially inhibited proliferation of HER-2/neu-overexpressing breast cancer cells. Taken together, our results suggest that HER-2/neu transcriptionally activates Jab1 expression to promote proliferation of breast cancer cells.

 , 刘勇
, 刘勇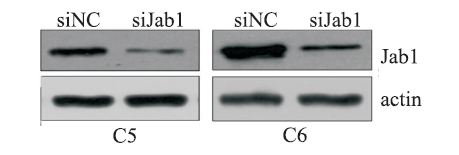

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}