中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 吉红梅, 陈云, 宋丰宇
, JI Hongmei, CHEN Yun, SONG Fengyu
, 吉红梅, 陈云, 宋丰宇
, JI Hongmei, CHEN Yun, SONG Fengyu
目的 观察不同脂质含量的脂肪乳对局部麻醉药物的吸附效果,探讨脂肪乳救治局部麻醉药物中毒的机制。方法 定量的盐酸布比卡因、盐酸罗哌卡因溶液中分别加入10%,20%,30%脂肪乳,漩涡10 min后,37 ℃下恒温水浴振荡15 h,离心后取下清液采用高效液相色谱(HPLC)检测。色谱柱为Agilent HC-C18(4.6 mm×250 mm,5 μm),流动相为乙腈-10 mmol·L-1磷酸二氢钠缓冲溶液(25:75),用磷酸溶液调节pH值=3.5,流速1 mL·min-1,柱温30 ℃,检测波长210 nm。结果 盐酸布比卡因在0.3~3.0 μg·mL-1浓度范围内线性关系良好,线性方程为
Objective To research sorption of local anesthetic by fat emulsion with different content of lipid
脂肪乳救治局部麻醉药物中毒的机制尚不清楚,人们根据大量的实验研究把解毒机制归结为三点:脂质槽机制、代谢与分布机制、脂肪酸补充理论[6]。其中脂质槽理论研究最多,因此,本实验通过体外实验,初步研究不同脂质含量的脂肪乳对局部麻醉药物的吸附效果,以期为脂肪乳体内解毒机制的研究奠定基础,从而指导临床如何合理使用脂肪乳救治局部麻醉药物中毒,同时也为脂肪乳救治其他药物中毒或寻找其他局部麻醉药物解毒剂提供研究方向。
盐酸布比卡因(批号:C053-070801);盐酸罗哌卡因(批号:C013-060602);10%脂肪乳(批号:1003171)、20%脂肪乳(批号:1003083)、30%脂肪乳(批号:0910093)均购自西安力邦制药有限公司;乙腈为色谱纯;磷酸二氢钠为分析纯。
高效液相色谱仪(Waters Alliance 2695 System);Waters2996二极管阵列检测器;赛特湘仪台式高速离心机(湖南赛特湘仪离心机仪器有限公司,TG16A-WS);马尔文Zeta 激光粒度和ZETA电位仪;漩涡混合器(宁波新芝生物科技股份有限公司,XW-80A);恒温水浴振荡器(上海智城分析仪器制造有限公司,ZHWY-110X30)。
临床上常用的局部麻醉药物为酰胺类局部麻醉药物,尤其以布比卡因、罗哌卡因、普鲁卡因使用较多。布比卡因使用最多,脂溶性较大,作用时间较长,可带来较大的毒性,因此大部分实验在研究使用脂肪乳用于救治局部麻醉药物中毒时通常采用布比卡因。本实验同时选用罗哌卡因与布比卡因进行对比,以研究脂肪乳在提取引起中高毒性的局部麻醉药物的效果。
局部麻醉药物在溶剂环境中的解离程度、脂肪乳脂质含量、脂肪乳乳滴大小及脂肪乳稳定性均影响到脂肪乳对局部麻醉药物的提取效果。故本实验先考察了3种规格脂肪乳的粒径、电位和pH值。动态光散射仪分别测定10%,20%,30%脂肪乳的粒径和电位。pH计测定不同脂质含量脂肪乳的pH值。表征结果见
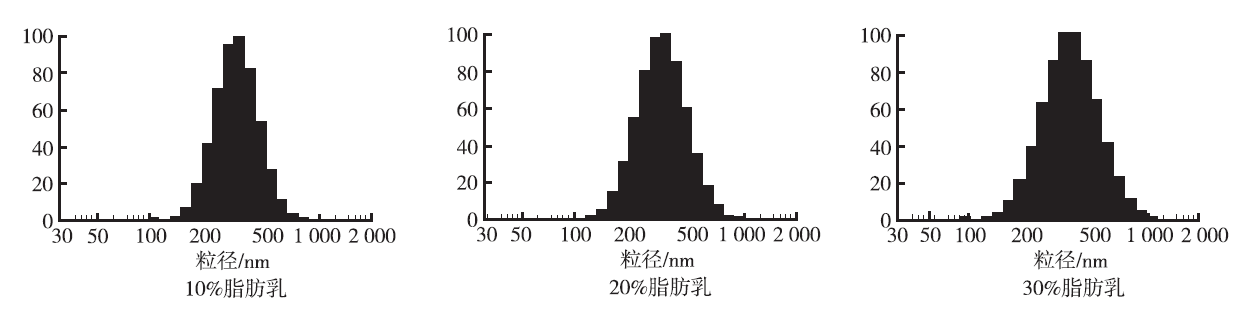
图1 10%,20%,30%脂肪乳粒径分布图
Fig.1 Distribution of partical size of 10%,20% and 30% lipid emulsion
表1 10%,20%,30%脂肪乳的表征结果
Tab.1 Physical properties of 10%,20% and 30% lipid emulsion
由以上结果可见,10%,20%,30%脂肪乳均呈现弱碱性,对局部麻醉药物解离程度的影响相近。3种规格脂肪乳的粒径随着脂质含量的增加略微增加。脂肪乳电位的大小直接影响脂肪乳的稳定性,从而影响脂肪乳是否能以乳滴形式存在起到脂质槽的作用,由以上数据可见3种脂肪乳均稳定存在。
2.3.1 色谱条件 色谱柱:Agilent HC-C18(4.6 mm×250 mm,5 μm);流动相:乙腈-磷酸二氢钠缓冲溶液10 mmol·L-1(25:75),用磷酸溶液调节pH值=3.5;流速:1 mL·min-1;柱温:30 ℃;进样量:20 μL;紫外检测,检测波长210 nm;单次时间20 min。
2.3.2 溶液配制
②盐酸布比卡因溶液的配制:精密称取盐酸布比卡因50 mg,置于100 mL量瓶中,加超纯水定容制得500 μg·mL-1盐酸布比卡因溶液。精密量取该溶液1 mL至10 mL量瓶中,加超纯水定容制得50 μg·mL-1的盐酸布比卡因溶液,同样稀释制得5 μg·mL-1的盐酸布比卡因溶液,置4 ℃冰箱保存备用。
精密量取50 μg·mL-1盐酸布比卡因溶液1 mL,置10 mL量瓶中,分别用10%,20%,30%脂肪乳定容至10 mL,则得到5 μg·mL-1盐酸布比卡因脂肪乳样品;取上述制备的脂肪乳样品5 mL置于10 mL离心管中,漩涡混合10 min;漩涡混合后置恒温水浴振荡器中,37 ℃下,200 r·min-1水浴振荡15h;然后10 000 r·min-1离心30 min,下清液逐滴滴出,记录下清液体积;取全部的脂肪乳样品离心下清液至5 mL量瓶中,用超纯水定容,高效液相色谱(HPLC)分析检测。盐酸罗哌卡因提取实验处理过程同盐酸布比卡因。每种浓度脂肪乳样品平行6个。空白样品的制备过程中把局部麻醉药物溶液换成1 mL的超纯水,其他步骤同上。
盐酸布比卡因、盐酸罗哌卡因出峰时间分别为15.8,9.6 min,见
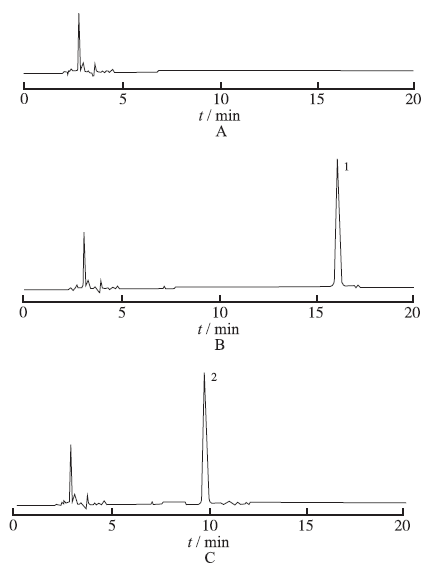
图2 脂肪乳提取局部麻醉药物色谱图 A.空白脂肪乳离心下清液;B.盐酸布比卡因脂肪乳下清液;C.盐酸罗哌卡因脂肪乳下清液;1.盐酸布比卡因;2.盐酸罗哌卡因
Fig.2 Chromatogram of local anesthetic extracted by fat emulsion A.centrifugal liquid below blank fat emulsion;B.centrifugal liquid below fat emulsion containing bupivacaine hydrochloride;C.centrifugal liquid below fat emulsion containing ropivacaine hydrochloride;1.bupivacaine hydrochloride;2.ropivacaine hydrochloride
精密量取5 μg·mL-1盐酸布比卡因溶液0.6,1,2,4,6 mL,置10 mL量瓶中,加超纯水至刻度,分别得到0.3,0.5,1,2,3 μg·mL-1盐酸布比卡因标准液。以样品吸收面积为纵坐标,盐酸布比卡因浓度为横坐标做标准曲线。结果线性方程为
取同一份样品分别于0,1,2,3,4,5 h时,按上述色谱条件进行,测定峰面积,分别计算出各个时间点游离浓度(μg·mL-1),结果见
表2 样品稳定性实验结果
Tab.2 Results of stability test on sample μg·mL-1
取同一份样品,平行进行5次,结果见
表3 样品重复性实验
Tab.3 Results of reproducibility test on sample μg·mL-1
HPLC检测下清液中盐酸布比卡因、盐酸罗哌卡因的峰面积记为S1、S2,代入标准曲线,算得游离盐酸布比卡因、盐酸罗哌卡因的含量,从而算得10%,20%,30%脂肪乳对等量盐酸布比卡因的吸附率,每种浓度脂肪乳样品制备6个,结果见
表4 不同脂质含量的脂肪乳对局部麻醉药物的吸附结果
Tab.4
Abosorption of local anesthetic by lipid emulsions with different lipid content
由以上结果可见,随着脂肪乳脂质含量的增加,对盐酸布比卡因、盐酸罗哌卡因的吸附均呈增加趋势,游离呈递减趋势。
自1998年WEINBERG等[7]首次报道了脂肪乳可成功救治大鼠局部麻醉药物过量使用后,2003年他们又报道了脂肪乳也可成功用于救治犬类局部麻醉药物过量使用[8]。2004年首次发表了脂肪乳可用于人体局部麻醉药物引起的心搏停止的治疗,并命名为“脂质救治”。ROSENBLATT等[9]2006年首次报道了1例腋路神经阻滞时发生局部麻醉药物中毒所致心搏骤停病例,经常规抢救无效使用脂肪乳剂后成功复苏。此后,一系列临床病例报道支持脂肪乳剂能够有效解救局部麻醉药物中毒所致的心血管毒性。基于这些动物实验和临床报道,2007年8月英国爱尔兰麻醉协会(Association of Anaesthetists of Great Britain and Ireland,AAGBI)发布了脂质救治局部麻醉药物中毒的指导方针,并指出所有的使用中毒剂量局部麻醉药物的部门都应该时刻备有脂肪乳。
脂肪乳是以大豆油为油相、卵磷脂为乳化剂形成的乳剂,人们推测脂肪乳在血液中形成脂质槽,与血液中的局部麻醉药物碰撞而将脂溶性局部麻醉药物吸附,从而能把局部麻醉药物从血浆中提取出来,使得局部麻醉药物不能到达其他易受损组织,或者迫使已经进入组织内的局部麻醉药物与高脂血浆重新分配,从而减少组织中局部麻醉药物的含量,达到解毒的作用。WEINBERG等[10]用放射线标记研究了20%含量脂肪乳对大鼠和猎犬的布比卡因中毒的救治,当脂肪乳和血浆混合后,布比卡因的体外脂肪乳/血浆分配系数为1.2,即布比卡因交换进入脂肪乳的能力要略微大于其在血浆中的溶解度,由此推测布比卡因完全可以被脂肪乳吸附从而不被组织吸收。并且脂肪乳可以加速大鼠体外心脏组织内的布比卡因的清除,降低布比卡因含量在心脏组织中的含量,解除布比卡因引起的心脏毒性。脂肪乳在解毒过程中以遍布血液的微小“脂肪库”捕捉局部麻醉药物,把脂溶性局部麻醉药物交换出受损组织,缓解甚至逆转其毒副作用。所以脂肪乳的解毒功效必然与血液中的脂肪乳乳滴的密度相关,实验数据显示脂肪乳用量增加,引起心搏暂停的布比卡因用量同比递增[10-11]。预注射脂肪乳还能提高布比卡因引起的心搏暂停的耐受量和动物苏醒成活率。
本实验采用10%,20%,30%脂肪乳对等量的盐酸布比卡因、盐酸罗哌卡因吸附效果进行了研究。在3种脂肪乳pH值均呈弱碱性、乳滴稳定的情况下,随着脂肪乳中脂质含量的增加,对局部麻醉药物吸附率也增加,但对盐酸布比卡因的吸附率略低于盐酸罗哌卡因。这说明脂肪乳能够吸附局部麻醉药物,且脂质含量越多,吸附能力越强。这也解释了动物与临床试验中脂肪乳可成功救治局部麻醉药物中毒。但是脂肪乳如何解救局部麻醉药物中毒?至今尚无定论,仅仅用脂质槽能捕捉局部麻醉药物来解释尚过于简单,脂肪乳救治局部麻醉药物中毒的效果可能不仅仅与脂质含量有关。体外实验存在缺陷,它是在忽略了体内环境的基础上进行的,但体内环境复杂,脂肪乳进入体内后与局部麻醉药物的作用过程受多方面因素影响。体外实验为体内实验提供了一定的理论基础,但不能代替体内实验,人们仍需进一步进行体内实验研究脂肪乳救治局部麻醉药物中毒的机制,从而很好地指导脂肪乳救治局部麻醉药物中毒,同时也为脂肪乳救治其他药物中毒或寻找其他局部麻醉药物解毒剂提供研究方向。
The authors have declared that no competing interests exist.

{kind=link}
{kind=link}
{kind=link}
{kind=link}