中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

目的 系统评价二肽基肽酶-4抑制药对2型糖尿病患者血脂的影响。方法 利用计算机检索建库至2017年2月PubMed、Cochrane Library、中国生物医学文献数据库(CBM)、中国期刊全文数据库(CNKI)及万方期刊数据库,选择符合纳入及排除标准的随机对照试验,采用RevMan 5.0版和Stata12.0版软件进行Meta分析。结果 共38篇随机对照试验研究纳入分析。Meta分析结果显示:与对照组比较,二肽基肽酶-4抑制药单独或联合使用能够降低2型糖尿病患者血清总胆固醇[
Objective To evaluate the effects of dipeptidyl peptidase-4 inhibitors on serum lipids in patients with type 2 diabetes mellitus. Methods Randomized controlled trials of related articles from inception to February 2017 were searched from PubMed,Cochrane Library,CBM,CNKI and
近几十年来,全球范围内糖尿病患病率正快速上升,预计到2035年2型糖尿病患者将增加到5.92亿例[1,2],将给社会和个人带来沉重的负担。血脂异常在2型糖尿病患者中非常普遍,72%~85%患者存在不同程度血脂异常[3,4]。2型糖尿病患者发生心血管事件的风险很高,血脂异常是2型糖尿病患者发生心血管疾病一个非常重要的危险因素[5],调节血脂紊乱能够显著降低2型糖尿患者心血管疾病风险[6,7]。为了给糖尿病患者寻求更有效、更安全的治疗方法,新的降糖药物不断涌现。在使用降糖药物时,不仅关注降糖效果,更希望它们具有减少心血管疾病风险(糖尿病患者的主要死因[8])的作用。从2008年12月开始,美国食品药品管理局(FDA)要求申请上市降糖药物必须进行心血管安全性评价。二肽基肽酶-4(dipeptidyl peptidase-4,DPP-4)抑制药作为治疗2型糖尿病的新药,在临床上应用时间不长,无论是单用还是联合使用都能达到相应的血糖控制目标。除了良好的血糖控制效果,DPP-4抑制药还表现出额外的血脂益处,但是诸多研究的结果并不一致。本研究旨在通过Meta分析探讨DPP-4抑制药对2型糖尿病患者血脂的影响。
计算机检索Cochrane Library、Pubmed、中国生物医学文献数据库(CBM)、中国期刊全文数据库(CNKI)和万方期刊数据库(WF),检索时限均为建库至2017年2月。英文检索词包括:dipeptidyl-peptidase IV inhibitors,sitagliptin,saxagliptin,vildagliptin,linagliptin,dutogliptin,alogliptin,anagliptin,omarigliptin,teneligliptin,diabetes mellitus,humans,randomized controlled trial;中文检索词包括:DPP-4抑制药、二肽基肽酶-4抑制药、西他列汀、维格列汀、沙格列汀、2型糖尿病、随机对照试验、临床试验等。
纳入标准:① 研究设计,均为临床随机对照试验(randomized controlled trials,RCT);②试验对象,2型糖尿病患者;③干预措施,试验组采用DPP-4抑制药单药或联合其他降糖药治疗,对照组为空白对照或其他降糖药单药或联合用药治疗;④结局指标,血清总胆固醇(total cholesterol,TC)、三酰甘油(triglyceride,TG)、低密度脂蛋白胆固醇(low-density lipoprotein cholesterol,LDL-C)、高密度脂蛋白胆固醇(high-density lipoprotein cholesterol,HDL-C)。排除标准:无法提取数据的文献、综述和摘要等。
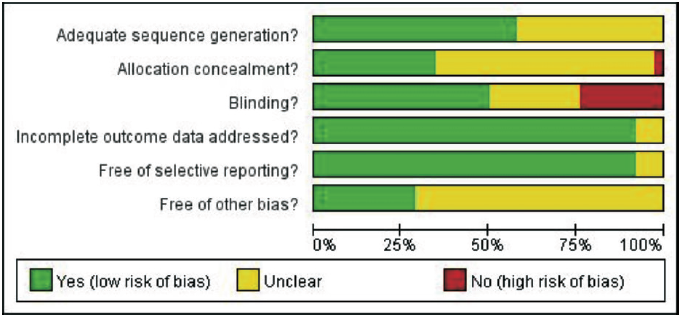
由2名研究者独立地进行资料提取和质量评价,若遇分歧,则由两人讨论后解决。采用自制的资料提取表提取资料,提取内容包括研究的一般信息、纳入对象的一般特征、干预方案及结局指标等。本研究采用Cochrane handbook for systematic reviews of intervention推荐的偏倚风险评估工具对纳入的RCT进行质量评价:①随机序列生成;②分配隐藏;③盲法;④结果数据不完整;⑤选择性报告;⑥其他偏倚。
采用RevMan 5.0版和Stata12.0版软件进行Meta分析。结局指标的合并效应采用加权均数差(weighted mean difference,
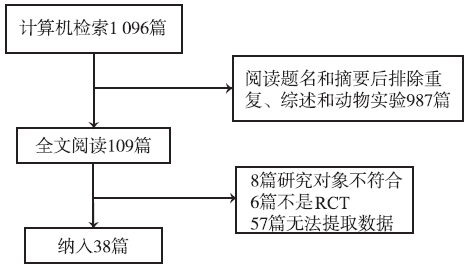
初步筛检获得相关文献1 096篇。阅读题名和摘要后排除重复、动物实验、非随机对照试验及综述987篇,剩下109篇阅读全文复筛,其中,8篇研究对象不合适,6篇不是RCT,57篇无法提取血脂数据,最终纳入38篇文献。文献筛选流程见
研究的基本特征见
表1 纳入研究的基本特征
Tab.1 Basic characteristics of the included studies
续表1 纳入研究的基本特征
Tab.1 Basic characteristics of the included studies
32篇文献比较DPP-4抑制药对血清TC的影响,结果见
亚组分析的结果见

图4 DPP-4抑制药对2型糖尿病患者血清三酰甘油的影响
Fig.4 Effect of DPP-4 inhibitors on serum TG in patients with type 2 diabetes mellitus
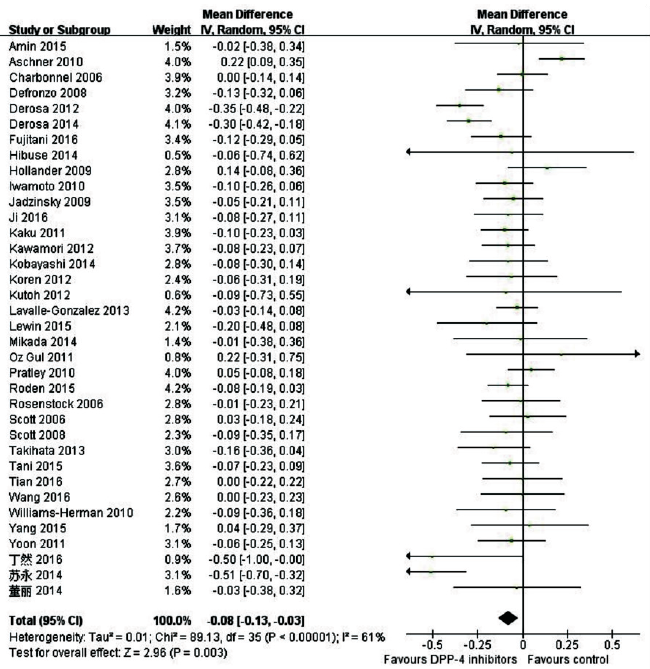
图5 DPP-4抑制药对2型糖尿病患者血清低密度脂蛋白胆固醇的影响
Fig.5 Effect of DPP-4 inhibitors on serum LDL-C in patients with type 2 diabetes mellitus
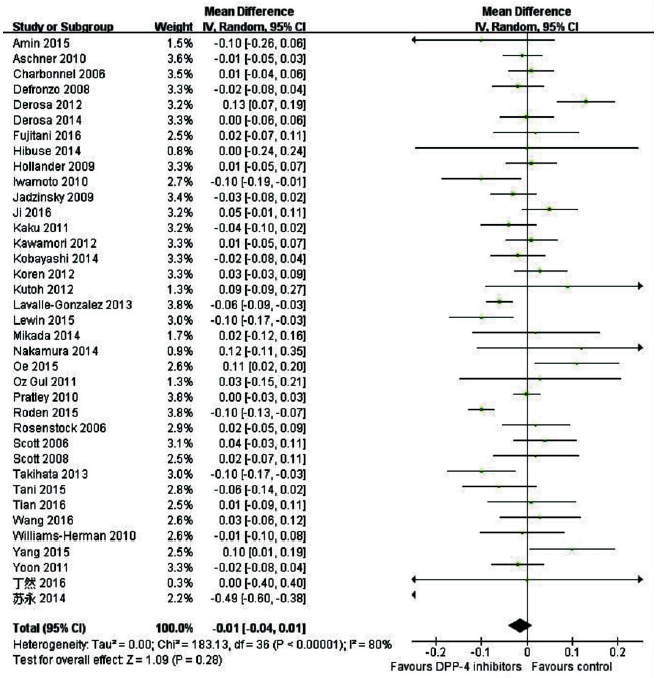
图6 DPP-4抑制药对2型糖尿病患者血清高密度脂蛋白胆固醇的影响
Fig.6 Effect of DPP-4 inhibitors on serum HDL-C in patients with type 2 diabetes mellitus
表2 血脂的亚组分析结果
Tab.2 Subgroup analysis on serum lipids
糖尿病是心血管疾病的重要危险因素,2型糖尿病患者发生致死和非致死性心血管事件的风险是正常人2~4倍[47,48]。血脂异常是导致2型糖尿病患者心血管疾病风险增加的主要因素[49,50]。TC、TG、LDL-C增高及HDL-C降低是2型糖尿病患者血脂异常的常见表现[51]。降低血脂水平能够显著降低2型糖尿病患者的心血管疾病风险,进而降低心血管疾病的病死率[52]。临床研究表明,DPP-4抑制药能够降低TC、TG和LDL-C水平[53,54]。 Meta分析结果显示DPP-4抑制药单用或者联合使用能够降低2型糖尿病患者TC、TG和LDL-C,但对HDL-C影响。目前尚不清楚DPP-4抑制药对血脂有利作用的机制,可能与其延缓胃排空、控制食欲有关。
LDL-C被认为是评价心血管疾病风险最有效的脂质指标,经常作为心血管疾病研究的主要终点,是2型糖尿病患者控制血脂的主要目标。控制LDL-C水平能够降低2型糖尿病患者心血管风险[55]。FAN等[56]研究最早上市的DPP-4抑制药西他列汀对血脂的影响,其Meta分析结果提示西他列汀对LDL-C无影响。本研究结果显示DPP-4抑制药治疗2型糖尿病患者时,能够降低患者LDL-C水平。亚组分析提示DPP-4抑制药联合用药相比单药降低LDL-C作用更明显;DPP-4抑制药这一类药中,西他列汀对LDL-C无影响,这与FAN等[56]研究一致,但阿格列汀、维达列汀和利格列汀显示出降低LDL-C的作用。
本研究还发现DPP-4抑制药有降低TC和TG的作用,这与MONAMI等[57]研究结果一致,亚组分析也显示出联合用药相比单独用药的优势,新型药物阿格列汀在这两个指标上都显示出了作用,这进一步提示联合用药可能会给患者带来更大的收益。FAN等[56]研究发现西他列汀能够升高患者的HDL-C,但本研究没有发现DPP-4抑制药对HDL-C作用,亚组分析也没有发现西他列汀对高密度脂蛋白的影响,MONAMI等[57]研究也没有发现DPP-4抑制药对HDL-C的影响,本研究结果与其一致。阿格列汀作为新的DPP-4抑制药,显示出较强的降低TC、TG和LDL-C的作用,但这都是基于亚组分析的结果,并且纳入的研究有限,还需要对阿格列汀进行更多的临床研究。
本研究的局限性主要在于以下几点;首先,纳入分析的大部分研究主要是为了评估DPP-4抑制药对血糖的影响,血脂指标不是主要的结局指标;其次,部分研究没有详细报道试验期间患者降脂治疗的情况,这可能会影响最终的效应;第三,潜在的发表偏倚不能排除,大部分相关的研究没有详细报道血脂的变化;最后,纳入分析的新型的DPP-4抑制药的研究较少,需要更多的研究去评估。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
Diabetes: a 21st century challenge
[本文引用:1]
|
| [3] |
|
| [4] |
La population étudiée peut être considérée comme représentative des patients diabétiques de type 209gés autonomes. Son suivi pendant cinq ans devrait permettre de préciser le lien entre l’équilibre glycémique et la morbi-mortalité.
[本文引用:1]
|
| [5] |
|
| [6] |
Background Patients with diabetes mellitus are at increased risk of developing cardiovascular disease. Controlling lipid levels has a preventive effect on the occurrence of major cardiovascular and cerebrovascular events. Individual trials have shown varying data on the efficacy of treatment with lipid-lowering statin therapy in the primary prevention of such events in diabetes. Objective The objective of this study was to assess the efficacy of statins in the primary prevention of the first-time occurrence of a major cardiovascular or cerebrovascular event in diabetic patients. Secondary endpoints were fatal/non-fatal stroke, fatal/non-fatal myocardial infarction and all-cause mortality. Methods A systematic search for trial reports was conducted in PubMed, EMBASE, The Cochrane library and clinicaltrials.gov for the years 1966–2011. Reference lists of reviews and meta-analyses of related subjects were searched. High-quality, randomized, double-blinded clinical trials comparing a statin with placebo for the primary prevention of major cardiovascular and cerebrovascular events in diabetic patients were selected. Only large studies with a minimum of 500 diabetic participants followed-up for at least 2 years were included. Endpoints were major cardiovascular and cerebrovascular events. Trial and patient characteristics were extracted by three researchers. The quality of the included studies was tested with the Jadad score. The combined effect on primary as well as secondary endpoints was measured with a fixed-effect model. Publication bias was examined with a funnel plot. Results Four trials were included, for a total of 10 187 participants. Treatment with statins in the primary prevention of major cardiovascular and cerebrovascular events in diabetic patients resulted in a significant relative risk (RR) reduction in the first-time occurrence of major cardiovascular or cerebrovascular events (RR 0.75, 95% CI 0.67–0.85), fatal/non-fatal stroke (RR 0.69, 95% CI 0.51–0.92) and fatal/non-fatal myocardial infarction (RR 0.70, 95% CI 0.54–0.90) and a non-significant RR reduction in all-cause mortality (RR 0.84, 95% CI 0.65–1.09). Among the studies there was non-significant heterogeneity in the individual effect estimates and no publication bias. Limitations Exclusion criteria and endpoints varied slightly between studies. The type and dosing of statin therapy differed between studies. Non-compliance in the statin treatment group and the use of statin treatment in the placebo group could have led to lower risk reductions. Conclusion Treatment with statins in primary prevention among diabetic patients has a significant beneficial effect on event rates of the first-time occurrence of a major cardiovascular or cerebrovascular event, fatal/non-fatal stroke and fatal/non-fatal myocardial infarction. There was a non-significant RR reduction in all-cause mortality.
[本文引用:1]
|
| [7] |
Although statin therapy reduces the risk of occlusive vascular events in people with diabetes mellitus, there is uncertainty about the effects on particular outcomes and whether such effects depend on the type of diabetes, lipid profile, or other factors. We undertook a prospective meta-analysis to help resolve these uncertainties. We analysed data from 1864686 individuals with diabetes (1466 with type 1 and 1764220 with type 2) in the context of a further 7164370 without diabetes in 14 randomised trials of statin therapy. Weighted estimates were obtained of effects on clinical outcomes per 1·0 mmol/L reduction in LDL cholesterol. During a mean follow-up of 4·3 years, there were 3247 major vascular events in people with diabetes. There was a 9% proportional reduction in all-cause mortality per mmol/L reduction in LDL cholesterol in participants with diabetes (rate ratio [RR] 0·91, 99% CI 0·82–1·01; p=0·02), which was similar to the 13% reduction in those without diabetes (0·87, 0·82–0·92; p<0·0001). This finding reflected a significant reduction in vascular mortality (0·87, 0·76–1·00; p=0·008) and no effect on non-vascular mortality (0·97, 0·82–1·16; p=0·7) in participants with diabetes. There was a significant 21% proportional reduction in major vascular events per mmol/L reduction in LDL cholesterol in people with diabetes (0·79, 0·72–0·86; p<0·0001), which was similar to the effect observed in those without diabetes (0·79, 0·76–0·82; p<0·0001). In diabetic participants there were reductions in myocardial infarction or coronary death (0·78, 0·69–0·87; p<0·0001), coronary revascularisation (0·75, 0·64–0·88; p<0·0001), and stroke (0·79, 0·67–0·93; p=0·0002). Among people with diabetes the proportional effects of statin therapy were similar irrespective of whether there was a prior history of vascular disease and irrespective of other baseline characteristics. After 5 years, 42 (95% CI 30–55) fewer people with diabetes had major vascular events per 1000 allocated statin therapy. Statin therapy should be considered for all diabetic individuals who are at sufficiently high risk of vascular events.
[本文引用:1]
|
| [8] |
ObjectiveTo assess associations between risks of cardiovascular disease, heart failure, and all cause mortality and different diabetes drugs in people with type 2 diabetes, particularly newer agents, including gliptins and thiazolidinediones (glitazones). DesignOpen cohort study. Setting1243 general practices contributing data to the QResearch database in England. Participants469 688 people with type 2 diabetes aged 25-84 years between 1 April 2007 and 31 January 2015. ExposuresDiabetes drugs (glitazones, gliptins, metformin, sulphonylureas, insulin, other) alone and in combination. Main outcome measureFirst recorded diagnoses of cardiovascular disease, heart failure, and all cause mortality recorded on the patients鈥 primary care, mortality, or hospital record. Cox proportional hazards models were used to estimate hazard ratios for diabetes treatments, adjusting for potential confounders. ResultsDuring follow-up, 21 308 patients (4.5%) received prescriptions for glitazones and 32 533 (6.9%) received prescriptions for gliptins. Compared with non-use, gliptins were significantly associated with an 18% decreased risk of all cause mortality, a 14% decreased risk of heart failure, and no significant change in risk of cardiovascular disease; corresponding values for glitazones were significantly decreased risks of 23% for all cause mortality, 26% for heart failure, and 25% for cardiovascular disease. Compared with no current treatment, there were no significant associations between monotherapy with gliptins and risk of any complications. Dual treatment with gliptins and metformin was associated with a decreased risk of all three outcomes (reductions of 38% for heart failure, 33% for cardiovascular disease, and 48% for all cause mortality). Triple treatment with metformin, sulphonylureas, and gliptins was associated with a decreased risk of all three outcomes (reductions of 40% for heart failure, 30% for cardiovascular disease, and 51% for all cause mortality). Compared with no current treatment, monotherapy with glitazone was associated with a 50% decreased risk of heart failure, and dual treatment with glitazones and metformin was associated with a decreased risk of all three outcomes (reductions of 50% for heart failure, 54% for cardiovascular disease, and 45% for all cause mortality); dual treatment with glitazones and sulphonylureas was associated with risk reductions of 35% for heart failure and 25% for cardiovascular disease; triple treatment with metformin, sulphonylureas, and glitazones was associated with decreased risks of all three outcomes (reductions of 46% for heart failure, 41% for cardiovascular disease, and 56% for all cause mortality). ConclusionsThere are clinically important differences in risk of cardiovascular disease, heart failure, and all cause mortality between different diabetes drugs alone and in combination. Overall, use of gliptins or glitazones was associated with decreased risks of heart failure, cardiovascular disease, and all cause mortality compared with non-use of these drugs. These results, which do not account for levels of adherence or dosage information and which are subject to confounding by indication, might have implications for prescribing of diabetes drugs.
[本文引用:1]
|
| [9] |
Aim To investigate the efficacy and safety of ertugliflozin, in a phase II dose-ranging study, in patients with type 2 diabetes mellitus (T2DM) inadequately controlled on metformin. Methods A total of 328 patients [mean T2DM duration, 6.365years; mean glycated haemoglobin (HbA1c), 8.1%] were randomized to once-daily ertugliflozin (1, 5, 10, 2565mg), sitagliptin (10065mg) or placebo, for 1265weeks. The primary efficacy endpoint was change from baseline to week 12 in HbA1c concentration and the secondary efficacy endpoints were changes from baseline to week 12 in body weight, fasting plasma glucose (FPG) and systolic/diastolic blood pressure (SBP/DBP). Safety and tolerability were also monitored. Results Ertugliflozin (1–2565mg/day) produced significant reductions in HbA1c concentration [placebo-corrected least-squares mean (LSM) 610.45% (165mg) to 610.72% (2565mg); p65≤650.002, similar to sitagliptin (610.76%; p65=650.0001)], FPG (LSM 611.17 to 611.9065mmol/l; p65 Conclusion Ertugliflozin (1–2565mg/day) improved glycaemic control, body weight and blood pressure in patients with T2DM suboptimally controlled on metformin, and was well tolerated.
[本文引用:0]
|
| [10] |
Aim: To compare the efficacy and safety of monotherapy with sitagliptin and metformin in treatment-na0104ve patients with type 2 diabetes. Methods: In a double-blind study, 1050 treatment-na0104ve patients (i.e. not taking an antihyperglycaemic agent for 09090616 weeks prior to study entry) with type 2 diabetes and an HbA 1c 6.50900099% were randomized (1:1) to treatment with once-daily sitagliptin 100 mg (N = 528) or twice-daily metformin 1000 mg (N = 522) for 24 weeks. Metformin was up-titrated from 500 to 2000 mg per day (or maximum tolerated daily dose 0909061000 mg) over a period of 5 weeks. The primary analysis used a per-protocol (PP) approach to assess whether sitagliptin was non-inferior to metformin based on HbA 1c change from baseline at week 24. Non-inferiority was to be declared if the upper boundary of the 95% confidence interval (CI) for the between-group difference in this endpoint was <0.40%. Results: From a mean baseline HbA 1c of 7.2% in the PP population, HbA 1c change from baseline was 0908080.43% with sitagliptin (n = 455) and 0908080.57% with metformin (n = 439). The between-group difference (95% CI) was 0.14% (0.06, 0.21), thus confirming non-inferiority. Baseline HbA 1c influenced treatment response, with larger reductions in HbA 1c observed in patients with baseline HbA 1c 0909068% in the sitagliptin (0900091.13%; n = 74) and metformin (0900091.24%; n = 73) groups. The proportions of patients at week 24 with HbA 1c values at the goals of <7 or <6.5% were 69 and 34% with sitagliptin and 76 and 39% with metformin, respectively. Fasting plasma glucose changes from baseline were 09080811.5 mg/dL (0900090.6 mmol/l) and 09080819.4 mg/dl (0900091.1 mmol/l) with sitagliptin and metformin, respectively (difference in LS mean change from baseline [95% CI] = 8.0 mg /dl [4.5,11.4]). Both treatments led to similar improvements from baseline in measures of homeostasis model assessment-0205 cell function (HOMA-0205) and insulin resistance (HOMA-IR). The incidence of hypoglycaemia was 1.7% with sitagliptin and 3.3% with metformin (p = 0.116). The incidence of gastrointestinal-related adverse experiences was substantially lower with sitagliptin (11.6%) compared with metformin (20.7%) (difference in incidence [95% CI] = 0908089.1% [09080813.6,0908084.7]), primarily because of significantly decreased incidences of diarrhoea (3.6 vs. 10.9%; p < 0.001) and nausea (1.1 vs. 3.1%; p = 0.032). Body weight was reduced from baseline with both sitagliptin (LS mean change [95% CI] = 0908080.6 kg [0908080.9,0908080.4]) and metformin (0900091.9 kg [0900092.2, 0908081.7]) (p < 0.001 for sitagliptin vs. metformin). Conclusions: In this 24-week monotherapy study, sitagliptin was non-inferior to metformin in improving HbA 1c in treatment-na0104ve patients with type 2 diabetes. Although both treatments were generally well tolerated, a lower incidence of gastrointestinal-related adverse experiences was observed with sitagliptin.
[本文引用:0]
|
| [11] |
DOI:10.2337/dc06-0706
URL
[本文引用:0]
|
| [12] |
OBJECTIVE: To evaluate the dipeptidyl peptidase-4 (DPP-4) inhibitor alogliptin in drug-naive patients with inadequately controlled type 2 diabetes. RESEARCH DESIGN AND METHODS: This double-blind, placebo-controlled, multicenter study included 329 patients with poorly controlled diabetes randomized to once-daily treatment with 12.5 mg alogliptin (n = 133), 25 mg alogliptin (n = 131), or placebo (n = 65) for 26 weeks. Primary efficacy end point was mean change from baseline in A1C at the final visit. RESULTS: At week 26, mean change in A1C was significantly greater (P < 0.001) for 12.5 mg (-0.56%) and 25 mg (-0.59%) alogliptin than placebo (-0.02%). Reductions in fasting plasma glucose were also greater (P < 0.001) in alogliptin-treated patients than in those receiving placebo. Overall, incidences of adverse events (67.4-70.3%) and hypoglycemia (1.5-3.0%) were similar across treatment groups. CONCLUSIONS: Alogliptin monotherapy was well tolerated and significantly improved glycemic control in patients with type 2 diabetes, without raising the incidence of hypoglycemia.
[本文引用:0]
|
| [13] |
Abstract The aim of this study was to evaluate whether the positive effects of sitagliptin on glycemic control and insulin resistance were maintained also after 2years of therapy and whether sitagliptin could be effective also in improving lipid profile. In this randomized, double-blind, placebo-controlled trial, 205 patients with type 2 diabetes in therapy with different antidiabetic drugs were randomized to add sitagliptin 100mg once a day or placebo to their current therapy. We evaluated at the baseline and after 6, 12, 18, and 24months the following parameters: body mass index, glycated hemoglobin (HbA 1c ), fasting plasma glucose (FPG), postprandial plasma glucose (PPG), fasting plasma insulin (FPI), homeostasis model assessment insulin resistance index (HOMA-IR), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (Tg). Sitagliptin, added to previously taken antidiabetic agents, proved to be effective in improving glycemic profile, reducing HbA 1c by 6117.5%, FPG by 6112.7%, PPG by 6120.5%. Regarding insulin resistance, sitagliptin decreased FPI by 618.3% and HOMA-IR by 6120.0%, confirming that what have been already reported in short-term studies can be applied also after 2years of treatment. Sitagliptin also reduced body weight by 614.3%. Our study also showed the positive effect of sitagliptin on lipid profile; in particular, sitagliptin decreased TC by 6113.3%, LDL-C by 6120.4%, and Tg by 6132.3%, and also increased HDL-C by+13.6%. Sitagliptin proved to be effective on glycemic profile and insulin resistance even after 2years of therapy and to be effective in improving body weight and lipid profile.
[本文引用:0]
|
| [14] |
Abstract Aims To compare the effects of vildagliptin with those of glimepiride on glycaemic control, fat tolerance and inflammatory markers in people with Type 2 diabetes mellitus receiving metformin treatment. Methods A total of 167 participants were randomized to vildagliptin 5002mg twice a day or glimepiride 202mg three times a day, for 602months. We evaluated the following variables: BMI; glycaemic control; fasting plasma insulin; homeostatic model assessment of insulin resistance index; fasting plasma proinsulin; glucagon; lipid profile; adiponectin; high-sensitivity C-reactive protein; interleukin-6; and tumour necrosis factor-α. A euglycaemic-hyperinsulinaemic clamp procedure and an oral fat load test were also performed. Results Despite a similar decrease in HbA1c levels ( P02 = 02 0.009, and P02 = 02 0.008, respectively), body weight increased with glimepiride ( P02 = 02 0.048 vs baseline) and decreased with vildagliptin ( P02 = 02 0.041 vs baseline and vs glimepiride). Fasting plasma insulin and homeostatic model assessment of insulin resistance index were significantly lower with vildagliptin compared with glimepiride ( P02 = 02 0.035 and 0.047). M value, an index of insulin sensitivity, increased with vildagliptin, both compared with baseline and with glimepiride ( P02 = 02 0.028 and 0.039, respectively). Vildagliptin improved all post-oral fat load peaks of lipid profile compared with glimepiride. Adiponectin levels were higher ( P02 = 02 0.035) and high-sensitivity C-reactive protein levels were lower ( P02 = 02 0.038) with vildagliptin vs glimepiride. During the oral fat load test, interleukin-6, high-sensitivity C-reactive protein and tumour necrosis factor-α peaks were lower and adiponectin peak was higher in the vildagliptin group than in the glimepiride group. There was a higher dropout rate as a result of hypoglycaemia in the glimepiride group than in the vildagliptin group. Conclusions Vildagliptin was more effective than glimepiride in reducing post-oral fat load peaks of lipid-trafficking adipocytokines and inflammatory markers.
[本文引用:0]
|
| [15] |
|
| [16] |
Background The dipeptidyl-peptidase-IV (DPP-4) inhibitors, including sitagliptin, are used for the treatment of type 2 diabetes mellitus (T2DM). Adiponectin, an adipocyte-derived circulating protein, has anti-atherosclerotic and anti-diabetic properties and is effectively elevated in bloodstream by thiazolidinediones, an insulin sensitizer. However, the effect of sitagliptin treatment on serum adiponectin level in T2DM has not fully elucidated in Japanese T2DM patients. The aim of the present study was to examine the effect of sitagliptin treatment on serum adiponectin levels in T2DM subjects. Methods Twenty-six consecutive Japanese T2DM outpatients were recruited between April 2011 and March 2013, and randomized into the control (conventional treatment, n???=???10) group and sitagliptin treatment group (n???=???16). Serum adiponectin was measured by enzyme-linked immunosorbent assay. Results Indices of glycemic control, such as hemoglobin A1c, glycated albumin, and 1.5-anhydro-D-glucitol, were significantly improved after the three-month treatment in both the control and sitagliptin groups. Serum adiponectin level was significantly increased in sitagliptin group from 6.7 0.8 to 7.4 1.0 g/mL without change of body mass index (p???=???0.034), while serum adiponectin level was not altered in the control group (p???=???0.601). Conclusion In Japanese T2DM patients, serum adiponectin level was elevated by three-month treatment with sitagliptin without change of body weight. Trial registration UMIN000004721
[本文引用:0]
|
| [17] |
Due to the natural progression of type 2 diabetes (T2D), most patients require combination therapy to maintain glycemic control.Our objective was to evaluate efficacy and safety of saxagliptin plus thiazolidinedione (TZD) in patients with T2D and inadequate glycemic control on TZD monotherapy.The study was a multicenter, randomized, double-blind, placebo (PBO)-controlled phase 3 trial conducted from March 13, 2006, to October 15, 2007.Patients were recruited from 172 outpatient centers.Patients with inadequately controlled T2D [glycosylated hemoglobin (HbA(1c)) 7.0-10.5%], 18-77 yr, receiving stable TZD monotherapy (pioglitazone 30 or 45 mg or rosiglitazone 4 or 8 mg) for at least 12 wk before screening were eligible.A total of 565 patients were randomized and treated with saxagliptin (2.5 or 5 mg) or PBO, once daily, plus stable TZD dose for 24 wk.Primary outcome was change in HbA(1c) from baseline to wk 24. Secondary outcomes were change from baseline to wk 24 in fasting plasma glucose, proportion of patients achieving HbA(1c) less than 7.0%, and postprandial glucose area under the curve.At 24 wk, saxagliptin (2.5 and 5 mg) plus TZD demonstrated statistically significant adjusted mean decreases vs. PBO in HbA(1c) [-0.66% (P = 0.0007) and -0.94% (P < 0.0001) vs. -0.30%] and fasting plasma glucose [-0.8 mmol/liter (P = 0.0053) and -1 mmol/liter (P = 0.0005) vs. -0.2 mmol/liter]. Proportion of patients achieving HbA(1c) less than 7.0% was greater for saxagliptin (2.5 and 5 mg) plus TZD vs. PBO [42.2% (P = 0.001) and 41.8% (P = 0.0013) vs. 25.6%]. Postprandial glucose area under the curve was significantly reduced [-436 mmol x min/liter (saxagliptin 2.5 mg plus TZD) and -514 mmol x min/liter (saxagliptin 5 mg plus TZD) vs. -149 mmol x min/liter (PBO)]. Saxagliptin was generally well tolerated; adverse event occurrence and reported hypoglycemic events were similar across all groups.Saxagliptin added to TZD provided statistically significant improvements in key parameters of glycemic control vs. TZD monotherapy and was generally well tolerated.
[本文引用:0]
|
| [18] |
Objective: To compare the efficacy and safety of sitagliptin (a dipeptidyl peptidase-4 inhibitor) and voglibose (an 02± -glucosidase inhibitor) monotherapy in Japanese patients with type 2 diabetes who have inadequate glycaemic control (HbA1c 0909066.5% and <10.0%) on diet and exercise. Methods: In a multi-center, randomized, double-blind, parallel-group study, 319 patients were randomized (1:1) to 12-week treatment with sitagliptin 50 mg once daily or voglibose 0.2 mg thrice daily before meals. The primary analysis assessed whether sitagliptin was non-inferior to voglibose in lowering HbA1c. Results: After 12 weeks, sitagliptin was non-inferior to voglibose for HbA1c-lowering efficacy. Furthermore, sitagliptin was superior to voglibose, providing significantly greater reductions in HbA1c from baseline [least squares mean changes in HbA1c [95% confidence intervals (CI)] = 0908080.7% (0908080.8 to 0908080.6) and 0908080.3% (0908080.4 to 0908080.2), respectively; between-group difference = 0908080.4% (0908080.5 to 0908080.3), p < 0.001]. Sitagliptin was also superior to voglibose on other key efficacy endpoints, including change from baseline in 2-h postmeal glucose (0908082.8 mmol/l vs. 0908081.8 mmol/l, p < 0.001) and fasting plasma glucose (0908081.1 mmol/l vs. 0908080.5 mmol/l, p < 0.001). After 12 weeks, the incidences of clinical adverse experiences (AEs), drug-related AEs and gastrointestinal AEs in the sitagliptin group (48.5, 10.4 and 18.4%, respectively) were significantly (p < 0.05) lower than those in the voglibose group (64.7, 26.3 and 34.6%, respectively). The incidences of hypoglycaemia, serious AEs and discontinuations due to AEs were low and similar in both groups. Conclusions: In Japanese patients with type 2 diabetes, once-daily sitagliptin monotherapy showed greater efficacy and better tolerability than thrice-daily voglibose over 12 weeks.
[本文引用:0]
|
| [19] |
Aim: The study aim was to evaluate the efficacy and safety of initial combination therapy with saxagliptin + metformin vs. saxagliptin or metformin monotherapy in treatment-na0104ve patients with type 2 diabetes (T2D) and inadequate glycaemic control. Methods: In this multicentre, randomized, double-blind, active-controlled phase 3 trial, 1306 treatment-na0104ve patients with T2D 09090618 to 0909¤77 years, glycosylated haemoglobin (HbA1c) 0909068 to 0909¤12%, fasting C-peptide concentration 0909061.0 ng/ml, body mass index 0909¤40 kg/m 2 were randomized to receive saxagliptin 5 mg + metformin 500 mg, saxagliptin 10 mg + metformin 500 mg, saxagliptin 10 mg + placebo or metformin 500 mg + placebo for 24 weeks. From weeks 10900095, metformin was uptitrated in 500-mg/day increments to 2000 mg/day maximum in the saxagliptin 5 mg + metformin, saxagliptin 10 mg + metformin and metformin + placebo treatment groups. The main outcome measure was HbA1c change from baseline to week 24. Selected secondary outcomes included change from baseline to week 24 in fasting plasma glucose (FPG), proportion of patients achieving HbA1c <7% and postprandial glucose area under the curve (PPG-AUC). Results: At 24 weeks, saxagliptin 5 mg + metformin and saxagliptin 10 mg + metformin demonstrated statistically significant adjusted mean decreases vs. saxagliptin 10 mg and metformin monotherapies in HbA1c (0908082.5 and 0908082.5% vs. 0908081.7 and 0908082.0%, all p < 0.0001 vs. monotherapy) and FPG (09080860 and 09080862 mg/dl vs. 09080831 and 09080847 mg/dl, both p < 0.0001 vs. saxagliptin 10 mg; p = 0.0002 saxagliptin 5 mg + metformin vs. metformin; p < 0.0001 saxagliptin 10 mg + metformin vs. metformin). Proportion of patients achieving an HbA1c <7% was 60.3 and 59.7%, respectively, for saxagliptin 5 mg + metformin and saxagliptin 10 mg + metformin (all p < 0.0001 vs. monotherapy). PPG-AUC was significantly reduced [09080821 080 mg00·min/dl (saxagliptin 5 mg + metformin) and 09080821 336 mg00·min/dl (saxagliptin 10 mg + metformin) vs. 09080816 054 mg00·min/dl (saxagliptin 10 mg) and 09080815 005 mg00·min/dl (metformin), all p < 0.0001 vs. monotherapy]. Adverse event occurrence was similar across all groups. Hypoglycaemic events were infrequent. Conclusion: Saxagliptin + metformin as initial therapy led to statistically significant improvements compared with either treatment alone across key glycaemic parameters with a tolerability profile similar to the monotherapy components.
[本文引用:0]
|
| [20] |
Abstract To compare the therapeutic effects of different regimens in Chinese obese type 2 diabetic mellitus (T2DM) patients. From October 2013 to July 2014, a total of 166 T2DM outpatients who attended the Shanghai Changhai Hospital and the Yijishan Hospital of Wannan Medical College were randomly assigned into an experimental sitagliptin/metformin combined with low caloric diet group (n090000=090000115) and an insulin glargine combined with metformin control group (n090000=09000051). Inclusion criteria were body mass index (BMI) 090906 25090000kg/m and diagnosed with T2DM with glycosylated hemoglobin (glycated hemoglobin A1C [HbA1c]) >9%. Main outcome parameters were fasting plasma glucose, postprandial plasma glucose, BMI, HbA1c, fasting C-peptide, 2-h postprandial C-peptide, triglyceride (TG), total cholesterol (TC), high-density cholesterol (HDL-C), and low-density cholesterol (LDL-C), which were determined by the 75090000g steamed-bun meal tolerance test before and 4, 8, 12, and 24 weeks after the treatment started. Treatment costs and life quality were also assessed. BMI, HbA1C, TG, TC, and LDL were significantly more reduced (P0900009%, oral sitagliptin/metformin combined with a low caloric diet effectively and economically maintained glycemic control and significantly improved life quality.
[本文引用:0]
|
| [21] |
|
| [22] |
|
| [23] |
DOI:10.1111/dom.12264
URL
[本文引用:0]
|
| [24] |
This study evaluated the effect of sitagliptin versus glibenclamide on arterial stiffness, blood pressure, lipid profile, oxidative stress, and high-sensitivity C-reactive protein (hsCRP) in type 2 diabetes mellitus patients.Forty diabetes patients, inadequately controlled on metformin, were randomly assigned to either sitagliptin (10065mg/day) or glibenclamide (565mg/day) for 3 months. Following a 1-month washout period, a crossover switch from glibenclamide to sitagliptin and vice versa was performed for an additional 3 months. Arterial stiffness, 24-h ambulatory blood pressure monitoring, lipids, hsCRP, glycated hemoglobin, fasting glucose, STAT-8-isoprostane (a measure of oxidative stress), body mass index (BMI), and waist circumference were measured at baseline and at 3 months with each of the study drugs.Thirty-four patients completed the study. Glibenclamide had a better glucose-lowering effect than sitagliptin, but this was associated with more hypoglycemic events. BMI increased following glibenclamide treatment, whereas sitagliptin proved weight-neutral. Mean BMI gain was +0.5±1.065kg/m(2) for glibenclamide versus -0.01±0.965kg/m(2) for sitagliptin (P<0.001). Triglyceride levels significantly dropped following sitagliptin, although they remained unaltered after glibenclamide treatment. Mean triglyceride decrease was -18.4±4565mg/mL after sitagliptin but -0.2±5765mg/dL following glibenclamide treatment (P=0.018). There was no change in low-density lipoprotein, high-density lipoprotein, arterial stiffness, blood pressure monitoring, hsCRP, or STAT-8-isoprostane with each of the study drugs.Sitagliptin, but not glibenclamide, demonstrated a significant beneficial effect on BMI and triglyceride levels. However, arterial stiffness, blood pressure, oxidative stress, and inflammatory status were not significantly affected by adding sitagliptin or glibenclamide to metformin-treated type 2 diabetes patients.
[本文引用:0]
|
| [25] |
Abstract The objectives of this study is to evaluate the efficacy and safety of alogliptin versus very low fat/calorie traditional Japanese diet (non-inferiority trial) as an initial therapy for newly diagnosed, drug na07ve subjects with type 2 diabetes (T2DM). Study design was prospective, randomized, non-double-blind, controlled trial. The study was conducted at outpatient units of municipal hospital. Patients were newly diagnosed, drug na07ve patients who visited the outpatient units. The patients randomly received 12.5-2502mg/day alogliptin (n02=0225) or severe low calorie traditional Japanese diet (n02=0226). The procedure of this trial was assessed by the consolidated standards of reporting trials statement. The primary end point was the change of HbA1c at 302months. Secondary end points included the changes of fasting blood glucose, insulin, homeostasis model assessment-R (HOMA-R), HOMA-B, body mass index (BMI), and lipid parameters. Similar, significant reductions of HbA1c levels were observed in both groups (from 10.51 to 8.74% for alogliptin and from 10.01 to 8.39% for traditional Japanese diet) without any clinically significant adverse events. In the alogliptin group, some subjects (16%) had mild hypoglycemic evens which could be managed by taking glucose drinks by themselves. HOMA-B significantly increased in both groups with varying degrees, whereas HOMA-R significantly decreased only in the Japanese diet group. Atherogenic lipids, such as, total cholesterol, non-high density lipoprotein cholesterol, and low density lipoprotein cholesterol levels significantly decreased in both groups. BMI had no change in the alogliptin group, whereas it significantly decreased in the Japanese diet group. (1) Concerning its glycemic efficacy, alogliptin is effective and non-inferior to traditional Japanese diet as an initial therapeutic option for newly diagnosed T2DM. However, regarding the reductions of body weight and insulin resistance, traditional Japanese diet is superior. (2) Both alogliptin and traditional Japanese diet have favorable effects on atherogenic lipid profiles.
[本文引用:0]
|
| [26] |
Aims/hypothesis The aim of this work was to evaluate the efficacy and safety of canagliflozin vs placebo and sitagliptin in patients with type 2 diabetes who were being treated with background...
[本文引用:0]
|
| [27] |
DOI:10.2337/dc14-2365
URL
[本文引用:0]
|
| [28] |
|
| [29] |
Alpha glucosidase inhibitor (GI) attenuates postprandial hyperglycemia (PPH) and reduces the risk of cardiovascular events in patients with impaired glucose tolerance or type 2 diabetes. Dipeptidyl peptidase 4 (DPP-4) inhibitors also attenuate PPH. PPH is one of the factors leading to endothelial dysfunction which is an early event in the pathogenesis of atherosclerosis. Furthermore, DPP-4 inhibitors protect endothelial function through a GLP-1-dependent mechanism. However, the impact of these two types of drugs on endothelial dysfunction in patients with type 2 diabetes has not been fully elucidated. We compared the effects of sitagliptin, a DPP-4 inhibitor, and voglibose, an alpha GI, on endothelial function in patients with diabetes. We conducted a randomized prospective multicenter study in 66 patients with type 2 diabetes who did not achieve the treatment goal with sulfonylurea, metformin or pioglitazone treatment; 31 patients received sitagliptin treatment and 35 patients, voglibose treatment. The flow-mediated dilatation (FMD) of the brachial artery was measured in the fasting state at baseline and after 12weeks of treatment. The primary endpoint was a change in FMD (FMD) from the baseline to the end of follow-up. The effects of sitagliptin and voglibose on FMD were assessed by ANCOVA after adjustment for the baseline FMD, age, sex, current smoking, diabetes duration and body mass index. Secondary efficacy measures included changes in HbA1c, GIP, GLP-1, C-peptide, CD34, lipid profile, oxidative stress markers, inflammatory markers and eGFR and any adverse events. FMD was significantly improved after 12weeks of treatment in both groups, and there was no significant difference in FMD between the two groups. There were no significant differences in changes in HbA1c, GIP, GLP-1, C-peptide, lipid profile, oxidative stress marker, inflammatory marker and eGFR between the two groups. Compared with voglibose, sitagliptin significantly increased the circulating CD34, a marker of endothelial progenitor cells. Adverse events were observed in 5 patients in only the voglibose group (diarrhea 1, nausea 1, edema 2 and abdominal fullness 1). Sitagliptin improved endothelial dysfunction just as well as voglibose in patients with type 2 diabetes. Sitagliptin had protective effects on endothelial function without adverse events. registered at http://www.umin.ac.jp/ctrj/ under UMIN000003951
[本文引用:0]
|
| [30] |
Background Left ventricular (LV) diastolic dysfunction is frequently observed in patients with type 2 diabetes. Dipeptidyl peptidase-4 inhibitor (DPP-4i) attenuates postprandial hyperglycemia (PPH) and may have cardio-protective effects. It remains unclear whether DPP-4i improves LV diastolic function in patients with type 2 diabetes, and, if so, it is attributable to the attenuation of PPH or to a direct cardiac effect of DPP-4i. We compared the effects of the DPP-4i, sitagliptin, and the alpha-glucosidase inhibitor, voglibose, on LV diastolic function in patients with type 2 diabetes. Methods We conducted a prospective, randomized, open-label, multicenter study of 100 diabetic patients with LV diastolic dysfunction. Patients received sitagliptin (50mg/day) or voglibose (0.6mg/day). The primary endpoints were changes in the e’ velocity and E/e’ ratio from baseline to 24weeks later. The secondary efficacy measures included HbA1c, GLP-1, lipid profiles, oxidative stress markers and inflammatory markers. Results The study was completed with 40 patients in the sitagliptin group and 40 patients in the voglibose group. There were no significant changes in the e’ velocity and E/e’ ratio from baseline to 24weeks later in both groups. However, analysis of covariance demonstrated that pioglitazone use is an independent factor associated with changes in the e’ and E/e’ ratio. Among patients not using pioglitazone, e’ increased and the E/e’ ratio decreased in both the sitagliptin and voglibose groups. GLP-1 level increased from baseline to 24weeks later only in the sitagliptin group (4.865±654.7 vs. 7.365±655.5 pmol/L, p 65<650.05). The reductions in HbA1c and body weight were significantly greater in the sitagliptin group than in the voglibose group (610.765±650.6% vs. 610.365±650.4, p 65<650.005; 611.365±653.2kg vs. 0.465±652.8kg, p 65<650.05, respectively). There were no changes in lipid profiles and inflammatory markers in both groups. Conclusions Our trial showed that sitagliptin reduces HbA1c levels more greatly than voglibose does, but that neither was associated with improvement in the echocardiographic parameters of LV diastolic function in patients with diabetes. Trial registration Registered at http://67www.67umin.67ac.67jp under UMIN000003784
[本文引用:0]
|
| [31] |
Abstract AIM: Sitagliptin is not associated with weight gain and has neutral effects on body weight. It is unclear whether sitagliptin treatment alters serum ghrelin levels in people with type 2 diabetes. METHODS: Forty-four subjects with type 2 diabetes were randomly assigned to receive sitagliptin or medical nutrition therapy (MNT) for 12 weeks. Changes in anthropometric variables, glycemic control, insulin resistance, lipid parameters, and total ghrelin levels were evaluated at baseline and following 12 weeks of treatment. RESULTS: Significant decreases in body weight and body mass index were observed over the entire study period in both treatment groups. Glycosylated hemoglobin and postprandial plasma glucose levels were statistically significant decreased in the groups receiving sitagliptin compared with baseline values (p=0.021 and p=0.021, respectively), while they were unchanged in the groups receiving MNT. There was a significant decrease in total ghrelin in the groups receiving sitagliptin (p=0.04) compared with baseline values but not in the groups receiving MNT (p=0.46) at the end of the 12 weeks. CONCLUSIONS: In this study of patients with type 2 diabetes, treatment with sitagliptin was associated with a significant decrease in serum ghrelin levels. These results suggest that the neutral effect of sitagliptin on weight might be associated with the suppression of fasting serum ghrelin levels. Copyright 2011 Elsevier Ireland Ltd. All rights reserved.
[本文引用:0]
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
Abstract AIM: To assess the addition of sitagliptin to ongoing metformin therapy in patients with type 2 diabetes who were inadequately controlled [haemoglobin A(1c) (HbA(1c)) 7-11%] on metformin monotherapy. METHODS: Patients (n = 273) on metformin (>/=1500 mg/day) were randomized to receive the addition of once-daily placebo, sitagliptin 100 mg or rosiglitazone 8 mg in a 1 : 1 : 1 ratio for 18 weeks. The efficacy analysis was based on the all-patients-treated population using an analysis of co-variance with change in HbA(1c) from baseline as the primary endpoint. RESULTS: The mean baseline HbA(1c) was 7.7% for the entire cohort. After 18 weeks, both active add-on therapies led to greater improvements in HbA(1c) from baseline: -0.73% for sitagliptin (p < 0.001 vs. placebo) and -0.79% for rosiglitazone compared with -0.22% for placebo. No difference was observed between the sitagliptin and rosiglitazone treatments (0.06% [95% confidence interval (CI): -0.14 to 0.25]). The proportion of patients achieving an HbA(1c) < 7% was greater with sitagliptin (55%) and rosiglitazone (63%) compared with placebo (38%). Body weight increased from baseline with rosiglitazone (1.5 kg) compared with body weight reduction with sitagliptin (-0.4 kg) and placebo (-0.8 kg). The difference in body weight between the sitagliptin and rosiglitazone groups was 1.9 kg (95% CI: 1.3-2.5). In a prespecified analysis, the proportion of patients experiencing a greater than 3-kg increase in body weight was 21% in the rosiglitazone group compared with 2% in both the sitagliptin and placebo groups. Both active treatments were generally well tolerated, with no increased risk of hypoglycaemia or gastrointestinal adverse events compared with placebo. CONCLUSIONS: In this 18-week study, the addition of sitagliptin was effective and well tolerated in patients with type 2 diabetes inadequately controlled with metformin monotherapy. Treatment with sitagliptin produced similar reductions in HbA(1c) compared with the addition of rosiglitazone.
[本文引用:0]
|
| [37] |
Abstract AIMS: To compare the efficacy and safety of these two agents and the impact on surrogate markers related to diabetic complications in Japanese type 2 diabetic patients. METHODS: In a multicenter, open-label trial, 130 patients whose diabetes had been inadequately controlled (HbA1c, 6.9-9.5%) with metformin and/or sulphonylurea were randomly assigned to a sitagliptin group (50 mg/day) or a pioglitazone group (15 mg/day) and were followed up for 24 weeks. At 16 weeks, if the patient's HbA1c level was ≥6.5%, the dose of sitagliptin or pioglitazone was increased up to 100 or 30 mg/day, respectively. Main outcome measure was the difference in the mean changes in the HbA1c level from baseline at 24 weeks between these two groups. RESULTS: Of the 130 patients who were enrolled, 115 subjects (sitagliptin group: 58 patients, pioglitazone group: 57 patients) completed this trial. At 0 weeks, the mean HbA1c level was 7.4765±650.66% in the sitagliptin group and 7.4065±650.61% in the pioglitazone group. At 24 weeks, the mean changes in the HbA1c level from baseline were -0.8665±650.63% versus -0.5865±650.68% (p65=650.024). Hypoglycaemia (2 patients, 3.4% vs. 2 patients, 3.5%), gastrointestinal symptoms (3 patients, 5.2% vs. 1 patient, 1.8%) and pretibial oedema (0 patients, 0% vs. 39 patients, 68.4%, p65<650.001) were observed for 24 weeks. CONCLUSIONS: Sitagliptin was not only more tolerable, but also more effective than pioglitazone in Japanese type 2 diabetic patients who had been treated with metformin and/or sulphonylurea. 08 2012 Blackwell Publishing Ltd.
[本文引用:0]
|
| [38] |
Dipeptidyl peptidase-4 (DPP-4) inhibitors may affect the serum levels of plasminogen activator inhibitor-1 (PAI-1) associated with triglyceride (TG) metabolism, which is a prognostic factor for cardiovascular disease, in diabetic patients. We conducted an 8-week, prospective, randomized study in which we assigned type 2 diabetic patients who were inadequately controlled with antidiabetic therapy to the vildagliptin group (5002mg bid, n02=0249) or the control group (n02= 49). The primary efficacy parameter was the change in the serum level of PAI-1, and the secondary end point was the change in the serum levels of TG-rich lipoproteins. In the vildagliptin group, significant decrease of the serum PAI-1 level by 16.3% (p <0.0001) and significant decreases of the serum TG, remnant-like particle cholesterol, and apolipoprotein B levels by 12.1% (p02= 0.002), 13.9% (p02= 0.003), and 9.5% (p <0.0001), respectively, were observed. No such changes were observed in the control group. Multivariate regression analyses identified the absolute change from the baseline (Δ) of the PAI-1, but not that of the fasting blood glucose or hemoglobin A1c, as independent predictors of the ΔTG, Δ remnant-like particle cholesterol, and Δ apolipoprotein B. In conclusion, treatment of type 2 diabetes with vildagliptin might prevent the progression of atherosclerotic cardiovascular disease in diabetic patients by decreasing the serum PAI-1 levels and improving TG metabolism.
[本文引用:0]
|
| [39] |
Abstract OBJECTIVE: Zinc-02±2-glycoprotein (ZAG) has recently been characterized as a potent metabolic regulator. However, the effects of anti-diabetic agents on circulating ZAG levels in humans remain largely unknown. To explore the possible mechanisms by which the dipeptidyl peptidase-IV (DPP-IV) inhibitor improves insulin resistance, we investigated the effect of sitagliptin, a DPP-IV inhibitor, on circulating cytokine levels in newly diagnosed type 2 diabetes (nT2DM) patients. DESIGN AND METHODS: A subset of 141 subjects with nT2DM were assigned to receive placebo (n=47) or sitagliptin (n=94) for 3 months. Before and after treatment, subjects received a 75 g oral glucose tolerance test, euglycemic-hyperinsulinemic clamp (EHC), and measurement of ZAG and adiponectin (ADI) concentrations. RESULTS: Circulating ZAG levels were lower in nT2DM than in control individuals (P<0.01). After 3 months of sitagliptin treatment, HbA1c, fasting plasma glucose, postprandial glucose, 2-h insulin after glucose overload, triglycerides, and homeostasis model assessment of insulin resistance (HOMA-IR) were decreased significantly compared with pre-treatment (P<0.05 or P<0.01), whereas the glucose infusion rate during the stable period of the clamp (M values) during EHC were significantly increased (P<0.01). In addition, circulating ZAG and ADI concentrations were significantly increased along with improved glucose metabolism and insulin sensitivity compared with pre-treatment (both P<0.01) and the change of ZAG (0200ZAG) was positively associated with 0200ADI, 0200HOMA-IR, 0200BMI, 0200fasting insulin and negatively associated with 0200 tumor necrosis factor-02± (TNF-02±). Furthermore, sitagliptin treatment resulted in significantly lowered plasma TNF-02± level (P<0.05). CONCLUSION: A low level of circulating ZAG is associated with insulin resistance and sitagliptin treatment significantly increases circulating ZAG levels. These observations have implications in relation to the mode of action of the DPP-IV inhibitor as an insulin sensitizing agent. 0008 2016 European Society of Endocrinology.
[本文引用:0]
|
| [40] |
Abstract BACKGROUND: Despite increasing prevalence of type 2 diabetes mellitus (T2DM) in Asia, clinical trials for glucose-lowering therapies are often dominated by Caucasian/Western populations. This phase III, randomized, placebo-controlled, double-blind, 24-week study (NCT01215097) evaluated the efficacy and safety of the DPP-4 inhibitor linagliptin added to metformin in Asian T2DM patients. METHODS: Enrolled patients were aged 18-80 years with HbA1c ≥7.0 to ≤10.0% on metformin therapy. Antidiabetes drugs other than metformin were washed out prior to randomization (2:1) to either linagliptin 5 mg daily or placebo added to metformin. A total of 306 Asian patients (China, n = 265; Malaysia, n = 17; the Philippines, n = 24) were randomized. The primary endpoint was change from baseline in mean HbA1c after 24 weeks. RESULTS: Baseline characteristics were well matched between groups (overall mean ± SD HbA1c, 8.0 ± 0.8%). Adjusted mean ± SE HbA1c decreased by -0.66 ± 0.05% in the linagliptin group and -0.14 ± 0.07% in the placebo group (placebo-corrected difference, -0.52 ± 0.09%; 95% CI: -0.70, -0.34; P < 0.0001). In patients with baseline HbA1c ≥8.5%, the placebo-corrected decrease in HbA1c was -0.89 ± 0.17% (P < 0.0001). Adverse events occurred in similar proportions of linagliptin and placebo patients (27.3% and 28.0%, respectively) and few were considered drug-related (2.4% and 0.0%, respectively). Hypoglycemia occurred in 1.0% of patients in both groups. Linagliptin therapy was weight neutral. CONCLUSIONS: In summary, linagliptin 5 mg was efficacious and well tolerated over 24 weeks in Asian patients with T2DM inadequately controlled by metformin. This article is protected by copyright. All rights reserved.
[本文引用:0]
|
| [41] |
|
| [42] |
Abstract The aim of this study was to evaluate the efficacy and safety of anagliptin in drug-na0104ve patients with type 2 diabetes in a double-blind randomized placebo-controlled study. A total of 109 patients were randomized to 100 mg (n=37) or 200 mg (n=33) anagliptin twice daily or placebo (n=39). The primary objective was to alter HbA1c levels from baseline at a 24-week endpoint. The overall baseline mean age and body mass index were 56.20 00± 9.77 years and 25.01 00± 2.97 kg/m(2), respectively, and the HbA1c level was of 7.14 00± 0.69 %. Anagliptin at 100 mg and 200 mg produced significant reductions in HbA1c (-0.50 00± 0.45 % and -0.51 00± 0.55%, respectively), and the placebo treatment resulted in an increase in HbA1c by 0.23 00± 0.62 %. Both doses of anagliptin produced significant decreases in fasting plasma glucose (-0.53 00± 1.25 mmol/L and -0.72 00± 1.25 mmol/L, respectively) and the proinsulin/insulin ratio (-0.04 00± 0.15 and -0.07 00± 0.18, respectively) compared with placebo. No meaningful body weight changes from baseline were observed in three groups. Plasma dipeptidyl peptidase (DPP)-4 activity was significantly inhibited after 24 weeks of anagliptin treatment, and >75% and >90% inhibitions were observed during the meal tolerance tests with 100 mg and 200 mg anagliptin, respectively. The incidences of adverse or serious adverse events were similar among the three study groups. Twice-daily anagliptin therapy effectively inhibited DPP-4 activity and improved glycemic control and was well-tolerated in patients with type 2 diabetes.
[本文引用:0]
|
| [43] |
SummaryAim/hypothesis: To assess the safety and efficacy of initial combination therapy with sitagliptin and pioglitazone compared with pioglitazone monotherapy in drug-na0104ve patients with type 2 diabetes.Methods: A total of 520 patients were randomised to initial combination therapy with sitagliptin 100 mg q.d. and pioglitazone 30 mg q.d. or pioglitazone 30 mg q.d. monotherapy for 24 weeks.Results: Initial combination therapy with sitagliptin and pioglitazone led to a mean reduction from baseline in A1C of 0908082.4% compared with 0908081.5% for pioglitazone monotherapy (p < 0.001). Mean reductions from baseline were greater in patients with a baseline A1C 090906 10% (0908083.0% with combination therapy vs. 0908082.1% with pioglitazone monotherapy) compared with patients with a baseline A1C < 10% (0908082.0% with combination therapy vs. 0908081.1% with pioglitazone monotherapy). Sixty percent of patients in the combination therapy group vs. 28% in the pioglitazone monotherapy group had an A1C of < 7% at week 24 (p < 0.001). Fasting plasma glucose decreased by 09080863.0 mg/dl (0908083.5 mmol/l) in the combination therapy group compared with 09080840.2 mg/dl (0908082.2 mmol/l) for pioglitazone monotherapy (p < 0.001), and 2-h post meal glucose decreased by 090808113.6 mg/dl (0908086.3 mmol/l) with combination therapy compared with 09080868.9 mg/dl (0908083.8 mmol/l) for pioglitazone monotherapy (p < 0.001). Measures related to 0205-cell function also improved significantly with combination therapy compared with pioglitazone monotherapy. Combination therapy was generally well-tolerated compared with pioglitazone monotherapy, with similar incidences of hypoglycemia (1.1% and 0.8%, respectively), gastrointestinal adverse events (5.7% and 6.9%, respectively), and oedema (2.7% and 3.5%, respectively).Conclusion/interpretation: Initial combination therapy with sitagliptin and pioglitazone substantially improved glycemic control and was generally well-tolerated compared with pioglitazone monotherapy.
[本文引用:0]
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
Background Uncertainties persist about the magnitude of associations of diabetes mellitus and fasting glucose concentration with risk of coronary heart disease and major stroke subtypes. We aimed to quantify these associations for a wide range of circumstances. Methods We undertook a meta-analysis of individual records of diabetes, fasting blood glucose concentration, and other risk factors in people without initial vascular disease from studies in the Emerging Risk Factors Collaboration. We combined within-study regressions that were adjusted for age, sex, smoking, systolic blood pressure, and body-mass index to calculate hazard ratios (HRs) for vascular disease. Findings Analyses included data for 698 782 people (52 765 non-fatal or fatal vascular outcomes; 8·49 million person-years at risk) from 102 prospective studies. Adjusted HRs with diabetes were: 2·00 (95% CI 1·83—2·19) for coronary heart disease; 2·27 (1·95—2·65) for ischaemic stroke; 1·56 (1·19—2·05) for haemorrhagic stroke; 1·84 (1·59—2·13) for unclassified stroke; and 1·73 (1·51—1·98) for the aggregate of other vascular deaths. HRs did not change appreciably after further adjustment for lipid, inflammatory, or renal markers. HRs for coronary heart disease were higher in women than in men, at 40—59 years than at 70 years and older, and with fatal than with non-fatal disease. At an adult population-wide prevalence of 10%, diabetes was estimated to account for 11% (10—12%) of vascular deaths. Fasting blood glucose concentration was non-linearly related to vascular risk, with no significant associations between 3·90 mmol/L and 5·59 mmol/L. Compared with fasting blood glucose concentrations of 3·90—5·59 mmol/L, HRs for coronary heart disease were: 1·07 (0·97—1·18) for lower than 3·90 mmol/L; 1·11 (1·04—1·18) for 5·60—6·09 mmol/L; and 1·17 (1·08—1·26) for 6·10—6·99 mmol/L. In people without a history of diabetes, information about fasting blood glucose concentration or impaired fasting glucose status did not significantly improve metrics of vascular disease prediction when added to information about several conventional risk factors. Interpretation Diabetes confers about a two-fold excess risk for a wide range of vascular diseases, independently from other conventional risk factors. In people without diabetes, fasting blood glucose concentration is modestly and non-linearly associated with risk of vascular disease.
[本文引用:1]
|
| [48] |
Background The extent to which diabetes mellitus or hyperglycemia is related to risk of death from cancer or other nonvascular conditions is uncertain. Methods We calculated hazard ratios for cause-specific death, according to baseline diabetes status or fasting glucose level, from individual-participant data on 123,205 deaths among 820,900 people in 97 prospective studies. Results After adjustment for age, sex, smoking status, and body-mass index, hazard ratios among persons with diabetes as compared with persons without diabetes were as follows: 1.80 (95% confidence interval [CI], 1.71 to 1.90) for death from any cause, 1.25 (95% CI, 1.19 to 1.31) for death from cancer, 2.32 (95% CI, 2.11 to 2.56) for death from vascular causes, and 1.73 (95% CI, 1.62 to 1.85) for death from other causes. Diabetes (vs. no diabetes) was moderately associated with death from cancers of the liver, pancreas, ovary, colorectum, lung, bladder, and breast. Aside from cancer and vascular disease, diabetes (vs. no diabetes) was also associated with death from renal disease, liver disease, pneumonia and other infectious diseases, mental disorders, nonhepatic digestive diseases, external causes, intentional self-harm, nervous-system disorders, and chronic obstructive pulmonary disease. Hazard ratios were appreciably reduced after further adjustment for glycemia measures, but not after adjustment for systolic blood pressure, lipid levels, inflammation or renal markers. Fasting glucose levels exceeding 100 mg per deciliter (5.6 mmol per liter), but not levels of 70 to 100 mg per deciliter (3.9 to 5.6 mmol per liter), were associated with death. A 50-year-old with diabetes died, on average, 6 years earlier than a counterpart without diabetes, with about 40% of the difference in survival attributable to excess nonvascular deaths. Conclusions In addition to vascular disease, diabetes is associated with substantial premature death from several cancers, infectious diseases, external causes, intentional self-harm, and degenerative disorders, independent of several major risk factors. (Funded by the British Heart Foundation and others.)
[本文引用:1]
|
| [49] |
We assessed the association between different blood lipid measures and risk of fatal/nonfatal coronary heart disease (CHD).We conducted an observational study of patients with type 2 diabetes from the Swedish National Diabetes Register. Baseline LDL cholesterol, non-HDL cholesterol, ratio of non-HDL to HDL cholesterol (non-HDL:HDL), and ratio of triacylglycerol to HDL cholesterol (TG:HDL) was measured in 18,673 patients aged 30-70 years, followed for a mean of 4.8 years from 2003 to 2007.Hazard ratios (HRs) for CHD per 1-SD increment in lipid measures were 1.23 with non-HDL:HDL, 1.20 with non-HDL cholesterol, 1.17 with LDL cholesterol, and 1.15 with TG:HDL (all P < 0.001 when adjusted for clinical characteristics and nonlipid risk factors). The best global model fit was found with non-HDL:HDL. When patients within the lowest tertile of a lipid measure were compared with those with all lipid measures within the highest tertile, the adjusted HR for CHD was 0.62 with non-HDL:HDL <3.5 mmol/L, 0.65 with non-HDL cholesterol <3.3 mmol/L, and 0.70 with LDL cholesterol <2.5 mmol/L (all P < 0.001). The lowest tertile of LDL and non-HDL cholesterol corresponded with treatment targets according to U.S. and European guidelines. HRs for CHD were 0.52, 0.62, and 0.66 with the lowest deciles of non-HDL:HDL, non-HDL cholesterol, and LDL cholesterol 1.8 mmol/L (all P < 0.001). Mean TG:HDL was considerably lower in patients within the lowest tertile of non-HDL:HDL, 0.82 0.47, than in those within the lowest tertile of LDL cholesterol (<2.5 mmol/L), 1.49 1.03.Non-HDL:HDL had a stronger effect on CHD risk than LDL cholesterol, and low TG:HDL values were more often seen within the lowest non-HDL:HDL tertile than within the lowest LDL cholesterol tertile. LDL cholesterol was not the best predictor of CHD risk in type 2 diabetes.
[本文引用:1]
|
| [50] |
To examine demographic, socioeconomic, and biological risk factors for all-cause, cardiovascular, and noncardiovascular mortality in patients with type 2 diabetes over 8 years and to construct mortality prediction equations.Beginning in 2000, survey and medical record information was obtained from 8,334 participants in Translating Research Into Action for Diabetes (TRIAD), a multicenter prospective observational study of diabetes care in managed care. The National Death Index was searched annually to obtain data on deaths over an 8-year follow-up period (2000-2007). Predictors examined included age, sex, race, education, income, smoking, age at diagnosis of diabetes, duration and treatment of diabetes, BMI, complications, comorbidities, and medication use.There were 1,616 (19%) deaths over the 8-year period. In the most parsimonious equation, the predictors of all-cause mortality included older age, male sex, white race, lower income, smoking, insulin treatment, nephropathy, history of dyslipidemia, higher LDL cholesterol, angina/myocardial infarction/other coronary disease/coronary angioplasty/bypass, congestive heart failure, aspirin, -blocker, and diuretic use, and higher Charlson Index.Risk of death can be predicted in people with type 2 diabetes using simple demographic, socioeconomic, and biological risk factors with fair reliability. Such prediction equations are essential for computer simulation models of diabetes progression and may, with further validation, be useful for patient management.
[本文引用:1]
|
| [51] |
Dyslipidemia is one of the key risk factors for cardiovascular disease (CVD) in diabetes mellitus. Despite the mounting clinical trial data, the management of dyslipidemia other than lowering the low density lipoprotein cholesterol (LDL-c) continues to be controversial. The characteristic features of diabetic dyslipidemia are high plasma triglyceride concentration, reduced high density lipoprotein cholesterol (HDL-c) concentration, and increased concentration of small dense LDL particles. These changes are caused by increased free fatty acid flux secondary to insulin resistance and aggravated by increased inflammatory adipokines. The availability of several lipid-lowering drugs and nutritional supplements offers novel and effective options for achieving target lipid levels in people with diabetes. While initiation of drug therapy based on differences in the lipid profile is an option, most practice guidelines recommend statins as first-line therapy. Although the evidence for clinical utility of combination of statins with fibrates or nicotinic acid in reducing cardiovascular events remains inconclusive, the preponderance of evidence suggests that a subgroup who have high triglycerides and low HDL-c levels may benefit from combination therapy of statins and fibrates. The goal of therapy is to achieve at least 30-40 % reduction in LDL-c levels. Preferably the LDL-c should be less than 100 mg/dL in low-risk people and less than 70 mg/dL in those at high risk, including people with established CVD.
[本文引用:1]
|
| [52] |
DOI:10.2337/dc14-S014
URL
[本文引用:1]
|
| [53] |
Abstract BACKGROUND: Animal studies have demonstrated that an inhibition of DPP-4 has an impact on the secretion of cholesterol and apoB by the small intestine. However, there is no consensus about the changes of the lipid profile following administration of sitagliptin. METHODS: Accordingly, we treated patients who had type 2 diabetes complicated by dyslipidemia with sitagliptin and evaluated its effects on the profile of lipid parameters. A total of 248 outpatients with type 2 diabetes complicated by dyslipidemia were treated with sitagliptin at a daily dose of 50 mg. The levels and percent changes of lipid and glucose metabolism markers were measured at baseline and at 12 weeks after the initiation of treatment. RESULTS: Both plasma glucose and HbA1c were significantly decreased. Among the lipid parameters, total cholesterol (TC) and non-high-density lipoprotein cholesterol (non-HDL-C) showed a significant decrease (TC 3.6±15.6%, non-HDL-C 2.9±19.7%; P < 0.05). Stratified analysis revealed a significant decrease of TC, low-density lipoprotein cholesterol (LDL-C) and non-HDL-C in the high triglyceride (TG) group (≥ 150 mg/dL) (P < 0.05). Analysis stratified by demographic factors demonstrated significant differences in the changes of TC, LDL-C and non-HDL-C. Multivariate analysis showed a significant decrease of the TC, LDL-C and non-HDL-C levels in the high TG group (≥ 150 mg/dL), as well as a significant decrease of TC and LDL-C in patients using strong statins. CONCLUSIONS: The results suggested that sitagliptin caused a significant decrease of TC, LDL-C and non-HDL-C, particularly in patients with high baseline TG levels and those using strong statins.
[本文引用:1]
|
| [54] |
Weight loss in patients with type 2 diabetes can improve glycemic control, lower blood pressure, and improve dyslipidemia. Glucagon-like peptide (GLP-1) receptor agonists are associated with weight loss and have potentially beneficial effects on cardiovascular risk biomarkers; however, there is limited information to indicate whether these effects remain outside of clinical trials. Medical records from the General Electric Centricity research database were analyzed retrospectively to evaluate the relationship between weight loss and glycemic control and changes in blood pressure and lipids in patients with type 2 diabetes initiating therapy with exenatide, sitagliptin, or insulin. Baseline and follow-up (90–365 days after the index date) for weight, A1C, fasting blood glucose (FBG), blood pressure, triglycerides, and LDL, HDL, and total cholesterol were assessed. A total of 6,280, 5,861, and 32,398 patients receiving exenatide, sitagliptin, or insulin, respectively, were included in the analysis. Exenatide-treated patients lost a mean ± SD of 3.0 ± 7.33 kg, sitagliptin-treated patients lost 1.1 ± 5.39 kg, and insulin-treated patients gained 0.6 ± 9.49 kg. There was a significant association between weight loss and a reduction in A1C and FBG with exenatide only and a reduction in blood pressure for all therapies. Weight loss was associated with some improvements in lipids, primarily in the GLP-1 receptor agonist group, with little association in the insulin group. Weight reduction with GLP-1 receptor agonists was associated with a shift toward a more favorable cardiovascular risk profile. Outcome trials are needed to determine whether improvement in biomarkers translates into a reduction in cardiovascular events in patients with type 2 diabetes.
[本文引用:1]
|
| [55] |
Abstract BACKGROUND: Although there is overwhelming evidence that reducing low-density lipoprotein cholesterol (LDL-C) with statins leads to reductions in cardiovascular disease, less is known about the effects in persons with type 2 diabetes mellitus (T2DM) without pre-existing vascular events. METHODS AND RESULTS: Using the UK-based General Practice Research Database we conducted a retrospective cohort study of 21,998 T2DM patients aged 35-69 with ≥2 prescriptions for lipid-modifying therapy (2000-2009). We categorized LDL-C change (mmol/l) between last available and baseline lipid values as reduction (≥3.0, 2.0-2.9, 1.0-1.9, 0.3-0.9), no-change (±0.2 of baseline), or increase (>0.2). Outcomes were incident composite cardiovascular (n65=65621) and cerebrovascular events (n65=65274). We estimated hazard ratios (HRs) of study outcomes and 95% confidence intervals (CIs) for LDL-C change compared with the no-change group. Compared to no changes, adjusted HRs of cardiovascular events for a reduction ≥3.0 and a reduction between 2.0-2.9 were 0.41 (95% CI: 0.23-0.71) and 0.51 (95% CI: 0.34-0.76) (p for linear trend <0.001). LDL-C reduction yielded a decreased cerebrovascular event risk compared to no change, even with the smallest reduction (adjusted HR65=650.59, 95% CI: 0.36-0.98). CONCLUSIONS: Decreasing LDL-C is associated with a reduced risk of cardiovascular and cerebrovascular events among T2DM patients without such pre-existing events. The magnitude of the protective effect on cerebrovascular events is less certain, and further studies are warranted. 08 The European Society of Cardiology 2013 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav.
[本文引用:1]
|
| [56] |
Abstract BACKGROUND: Animal studies have demonstrated that an inhibition of DPP-4 has an impact on the secretion of cholesterol and apoB by the small intestine. However, there is no consensus about the changes of the lipid profile following administration of sitagliptin. METHODS: Accordingly, we treated patients who had type 2 diabetes complicated by dyslipidemia with sitagliptin and evaluated its effects on the profile of lipid parameters. A total of 248 outpatients with type 2 diabetes complicated by dyslipidemia were treated with sitagliptin at a daily dose of 50 mg. The levels and percent changes of lipid and glucose metabolism markers were measured at baseline and at 12 weeks after the initiation of treatment. RESULTS: Both plasma glucose and HbA1c were significantly decreased. Among the lipid parameters, total cholesterol (TC) and non-high-density lipoprotein cholesterol (non-HDL-C) showed a significant decrease (TC 3.6±15.6%, non-HDL-C 2.9±19.7%; P < 0.05). Stratified analysis revealed a significant decrease of TC, low-density lipoprotein cholesterol (LDL-C) and non-HDL-C in the high triglyceride (TG) group (≥ 150 mg/dL) (P < 0.05). Analysis stratified by demographic factors demonstrated significant differences in the changes of TC, LDL-C and non-HDL-C. Multivariate analysis showed a significant decrease of the TC, LDL-C and non-HDL-C levels in the high TG group (≥ 150 mg/dL), as well as a significant decrease of TC and LDL-C in patients using strong statins. CONCLUSIONS: The results suggested that sitagliptin caused a significant decrease of TC, LDL-C and non-HDL-C, particularly in patients with high baseline TG levels and those using strong statins.
[本文引用:3]
|
| [57] |
Introduction Lipid profile is an important determinant of cardiovascular risk in type 2 diabetic patients. Available glucose-lowering agents can affect lipid levels. Dipeptidyl peptidase-4 (DPP-4)...
[本文引用:2]
|


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}