中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

 , 岳源
, YUE Yuan
, 岳源
, YUE Yuan
目的 探讨γ-氨基丁酸(GABA)改善2,4,6-三硝基苯磺酸(TNBS) -乙醇诱导的结肠炎肠黏膜屏障损伤作用。方法 SD大鼠随机分为正常对照组,TNBS-乙醇溶液模型对照组,造模后GABA 200,100,50 mg·kg-1治疗组。造模后连续14 d,观察记录体质量变化、疾病活动指数(DAI);造模第15天,每组取5只,进行伊文思蓝染色。大鼠取结肠,组织学损伤评分,同时量取结肠长度、称重。通过WB法观察实验性结肠炎各组大鼠肠黏膜屏障连接蛋白及LC3表达情况。结果 GABA增加Caco-2细胞单层模型细胞电阻,减少FD4的渗透,降低单层模型通透性。GABA改善实验性结肠炎引起的体质量下降,增加DAI,降低结肠指数。另外,GABA降低实验性结肠炎大鼠伊文思蓝渗透性及结肠病理变化,显著提高大鼠Occludin、Claudin-4、ZO-1蛋白表达。实验性结肠炎大鼠肠细胞出现过度自噬,GABA抑制过度自噬。结论 GABA通过改善肠黏膜屏障损伤,缓解TNBS-乙醇溶液诱导的实验性结肠炎,故改善肠黏膜屏障损伤可能是治疗炎症性肠病(IBD)的新方法。
Objective To investigate the protective effects of GABA against experimental inflammatory bowel disease (IBD) by enhanced intestinal barrier function and explore its underlying mechanisms. Methods Forty SD rats were randomly divided into normal control group, TNBS-alcohol model control group, 200, 100, 50 mg·kg-1 GABA treatment group.After modeling for 14 days, the changes of body weight and disease activity indexes (DAI) were observed.On the 15th day after modeling, 5 rats in each group were subjected to Evans blue staining.For the remaining rats, colon was collected and evaluated with histological injury score; the length and weight of the colon was determined.The intestinal mucosal barrier connexin and LC3 expression in rats with experimental colitis were observed by WB method. Results The cell resistance of Caco-2 monolayer models was increased and the infiltration of FD4 and the monolayer permeability was reduced by GABA.GABA also improved body mass, increased DAI, and lowered colon index.In addition, GABA decreased the Evans blue permeability and pathological changes in rats with experimental colitis, and significantly increased the Occludin, Claudin-4 and ZO-1 protein expression in the rats.Intestinal autophagy appeared in experimental colitis rats, GABA inhibited excessive autophagy. Conclusion GABA could relieve TNBS-ethanol-induced experimental colitis, and the mechanism might be related to the improvement of intestinal mucosal barrier injury.
炎症性肠病(inflammatory bowel disease,IBD)是一种病因和发病机制尚不十分确定的慢性肠道非特异性炎症疾病[1]。目前采用的治疗药物有效率低,治疗现状不理想。因此,突破原有治疗限制,寻找新的治疗策略值得探索。研究表明,IBD患者一般有肠黏膜通透性增高[2]。肠上皮细胞的黏膜屏障的破坏使肠内潜在免疫抗原被大量摄取,从而导致无节制的免疫反应[3]。肠黏膜通透性增高可能是IBD 的原发因素[4,5]。因此,增加肠黏膜屏障可能为防治IBD提供新的治疗手段。γ-氨基丁酸(gamma-aminobutyric acid,GABA)在中枢神经系统中是最主要的抑制性神经递质。GABA在实验性结肠炎致黏膜屏障损伤中的研究尚未见报道。本研究建立Caco-2黏膜屏障单层模型,进行GABA对体外肠黏膜屏障模型的作用及机制研究。 同时探讨 GABA 对于 2,4,6-三硝基苯磺酸(2,4,6,-trinitrobenzene sulfonic acid,TNBS) -乙醇诱导的结肠炎肠黏膜屏障损伤的干预作用。
SD 大鼠,SPF 级,体质量 200~250 g,40只,雄性,由武汉大学动物实验中心提供,动物生产许可证号:SCXK(鄂)2014-0004;动物合格证编号:00017226。在武汉大学动物实验中心饲养,动物房通风良好,室温(22±2) ℃,光照时间12 h、自由进食及饮水,实验前适应5 d。动物实验依据ARRIVE指南(Animal Research:Reporting In Vivo Experiments)进行,经武汉大学动物实验中心动物保健和使用委员会 (Institutional Animal Care and Use Committee,IACUC)批准。
TNBS (美国Sigma公司,批号:111M5001V);脂多糖 (lipopolysaccharides,LPS,美国Sigma公司,批号:L-2880,规格:50 μg);磷酸缓冲盐溶液(phosphate buffer saline,PBS,杭州吉诺生物医药技术有限公司);γ-氨基丁酸(γ-aminobutyrie acid,GABA,国药集团化学试剂有限公司,规格:500 g);RIPA 裂解液(碧云天生物技术研究所,批号:P0013B);增强化学发光法(enhanced chemiluminescence,ECL)试剂盒(碧云天生物技术研究所,批号:P0018);二喹啉甲酸法(bicinchoninic acid,BCA)蛋白浓度试剂盒(南京建成生物制品研究所,批号:2017110337)。
Milicell-ERS型电阻测定仪(美国Millipore公司)。DF-540 型荧光分光光度计(日本岛津)。倒置显微镜(重庆广电仪器有限公司)。蛋白凝胶电泳(上海天能科技有限公司)。DU800型紫外-可见分光光度计(Beckman公司)。
Caco-2细胞(购自中国典型培养物保藏中心,CCTCC 编号:GDC153)以含10%FBS,1%非必需氨基酸,1%
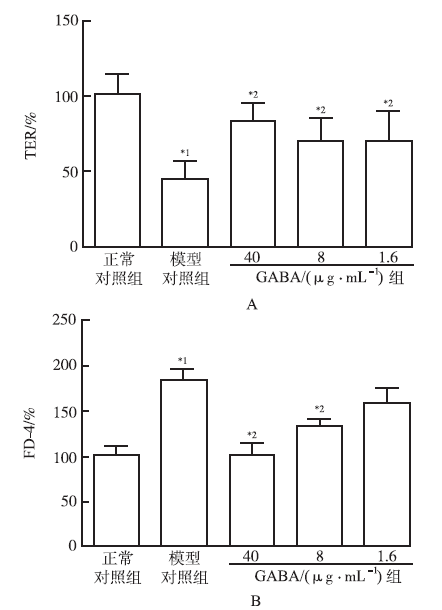
当细胞达到80%融合后,以0.5×106·(cm2)-1细胞接种于24孔板的Transwell聚碳酸酯膜(直径12 mm,孔径0.4 μm)小室中。细胞培养期间用Milicell-ERS电阻测定仪测定单层Caco-2细胞的跨上皮电阻(transepithelial electrical resistance,TER)。细胞培养至10~11 d,TER在1 000~1 200 Ω·(cm2)-1时,进行下一步实验[6]。在Caco-2细胞培养液中加入LPS(50 μg·mL-1),同时加入PBS,不同浓度GABA(用PBS溶解配置 400,80,16 μg·mL-1 浓度梯度的 GABA 溶液,加入至培养液中使 GABA 的终浓度为40,8,1.6 μg·mL-1),平行设置空白对照组(不加LPS及药物,加入等体积PBS),共同孵育培养24 h,测定单层Caco-2细胞的跨上皮电阻。同时,给药后21 h时向细胞培养液中加入荧光素标记葡聚糖(FITC-dextran,平均分子量4 000),孵育培养3 h。收集底室培养液,用DF-540 型荧光分光光度计(激发波长 495 nm,发射波长 520 nm)测定荧光强度,计算FITC-dextran含量。
造模前所有实验大鼠禁食24 h,自由饮水。TNBS 溶解于体积分数为50%的乙醇溶液中,使TNBS 的终浓度为25 mg·mL-1。实验大鼠以乙醚轻度麻醉后,将大鼠置于倒悬位,用一直径为2 mm、长约12 cm的橡胶输液管,将其表面涂以石蜡油润滑后,缓慢插入距大鼠肛门约8 cm处的结肠腔内,用无菌注射器将100 mg·kg-1 TNBS-乙醇溶液注入结肠腔内,为防止药液流出肛门,将实验大鼠保持头朝下倒垂姿势约1 min后缓慢拔出橡胶输液管。根据疾病活动指数(disease activity index,DAI)判断模型是否成功。 造模后大鼠体质量下降,大便松散,腹泻,并且出现大便隐血,即造模成功[7]。
根据大鼠体质量,采用系统随机化法随机分为5组,除正常对照组外其他4组按上述方法造模,造模后自由饮食饲养3 d,第3天根据DAI判断模型全部成功。4组造模大鼠按照 DAI 评分重新采用系统随机化法随机分成4组,每组8只。开始给药,各组处理如下:GABA 大剂量(200 mg·kg-1)、中剂量(100 mg·kg-1)、小剂量(50 mg·kg-1) 组分别灌胃给予 40,20,10 mg·mL-1的 GABA 0.5 mL·(100 g)-1。各组给药每天1次,持续11 d。实验期间,大鼠自由饮食、饮水,进行DAI评分观察。第14天,处死动物。所有大鼠进行结肠组织大体形态评分、结肠炎症组织病理学观察等指标测定。其中正常对照组、模型对照组、GABA大剂量(200 mg·kg-1)行组织蛋白含量检测。
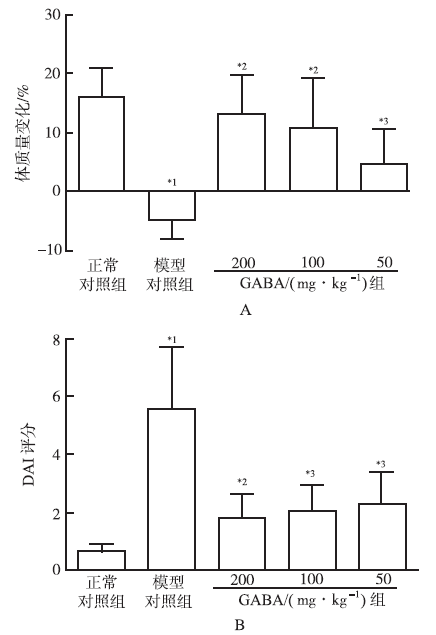
1.8.1 DAI评分 评分实验过程中每天观察大鼠体质量变化和大便性状,并且每天观察或用粪便隐血试纸检测大便带血情况,按文献方法行DAI 评分[8]。
1.8.2 大鼠结肠黏膜渗透性检测 按Lange法使用伊文思蓝(Evan’blue,EB)检测结肠通透性[9]。大鼠麻醉,剖腹,剪断盲肠末端,温PBS由肛门开始冲洗整段结肠,结扎剪断的盲肠末端以及直肠与降结肠交汇处以形成闭合袢,并注入1.5% EB 0.5 mL,关腹腔。2 h后处死大鼠,取出结肠并剪开,乙酰半胱氨酸冲洗3次,滤纸吸干后称质量,然后加入甲酰胺2 mL,50 ℃水浴箱中提取48 h,660 nm下测定吸光度。
1.8.3 结肠组织大体形态评分 两个盲态实验设计的独立观察者对结肠组织进行大体形态评分。解剖结肠,测量结肠长度和质量计算结肠单位长度质量。肛门至盲肠段结肠沿肠系膜纵轴剪开,20 ℃的0.9%氯化钠溶液冲洗干净,进行大体形态评分。参照文献[10]:0=无损伤;1=轻度充血、水肿,无糜烂或溃疡;2=中度充血、水肿,糜烂或浅溃疡;3=重度充血、水肿,黏膜表面有坏死及溃疡形成,溃疡直径<1 cm;4=重度充血、水肿,坏死及溃疡形成,溃疡直径>1 cm。
1.8.4 大鼠结肠炎症组织病理学观察 大鼠处死,取距离肛门8 cm处结肠,4%多聚甲醛固定,常规脱水,石蜡包埋,切片。进行苏木精-伊红(HE)染色和阿利新蓝(AB-PAS)染色。100倍光学显微镜下观察病理变化。
1.8.5 结肠组织蛋白含量检测 取上述另一份结肠组织加入5倍量RIPA裂解液,匀浆。或者Caco-2细胞加入RIPA裂解液,超声破碎细胞。低温高速离心[4 ℃,12 000 r·min-1 (
采用SPSS13.0版统计软件,实验结果数据采用均数±标准差(
通过建立Caco-2细胞单层体外黏膜屏障模型,观察GABA对体外黏膜屏障完整性的影响。结果可见,LPS刺激后,单层细胞模型TER显著降低(
实验期间,模型对照组于第3天死亡大鼠2只,第5天死亡大鼠1只,其余4组未出现大鼠死亡情况。给药期间,正常对照组大鼠毛发光泽、饮食饮水正常,体质量逐渐增加,活动敏捷,未出现稀便情况,大鼠肛周洁净;模型对照组大鼠自造模后第2天出现饮食下降,第4天出现血便,实验期间大鼠稀便,体质量降低,出现懒动,精神萎靡等症状。GABA给药组造模后初期出现腹泻、体质量下降,饮食减少现象,但程度较轻,且大鼠精神、食欲随给药时间延长逐渐好转,体质量逐步增加,腹泻在给药1周后逐渐消失。结果见
正常对照组大鼠的结肠均匀细长,颜色呈嫩粉色且色泽均一。TNBS造模形成的实验性结肠炎大鼠结肠段不同程度充血,肠壁增厚,伴有溃疡出现,且形成巨结肠,黏膜表面坏死,病变处黏膜呈黑褐色,其结肠重量和组织大体形态损伤评分显著高于正常对照组(
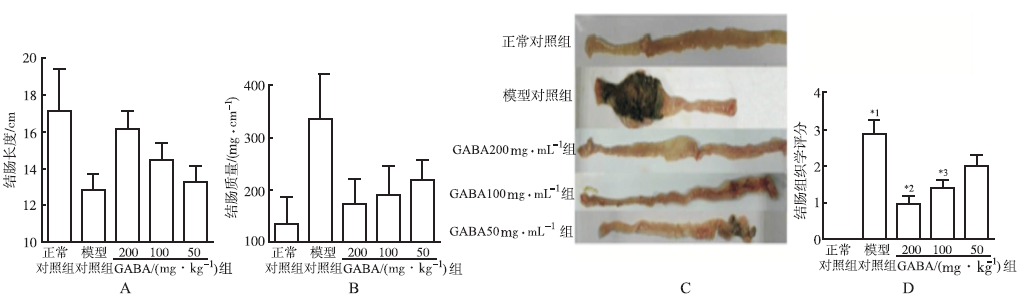
图3
5组大鼠结肠长度(A)、质量(B)、形态(C)及组织学评分(D)比较(
Fig.3
Comparison of colon length(A),weight(B),appearance(C) and histologic scores(D) among five groups of rats(
大鼠结肠病理学观察可见,正常对照组大鼠结肠黏膜上皮完整连续,结构清晰,排列紧密有规则,未见炎症细胞浸润,无糜烂及溃疡形成。模型对照组大鼠结肠腺体结构破坏异常,黏膜、黏膜下层出现中性粒细胞、淋巴细胞等大量炎症细胞浸润,黏膜下层结构紊乱、水肿,结肠组织病理学评分显著高于正常对照组(
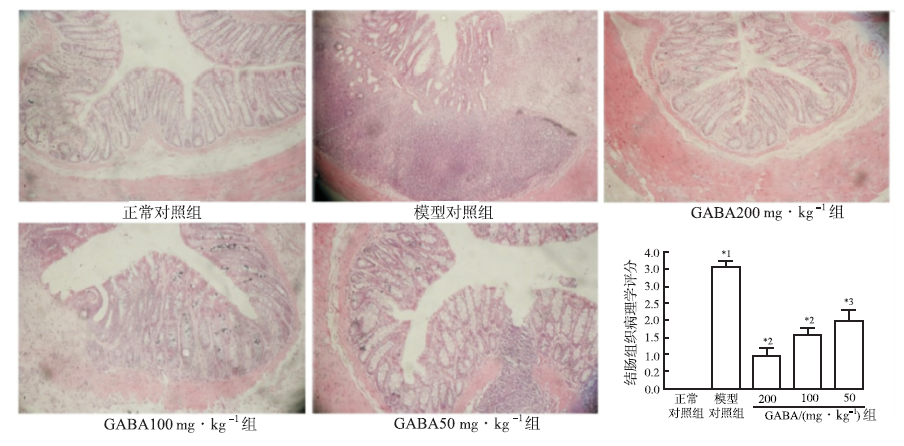
图4
5组大鼠结肠组织病理学切片及组织损伤评分的比较(×100,
Fig.4
Comparison of histopathological image and tissue injury scores among five groups of rats(×100,
大鼠结肠AB-PAS染色结果见
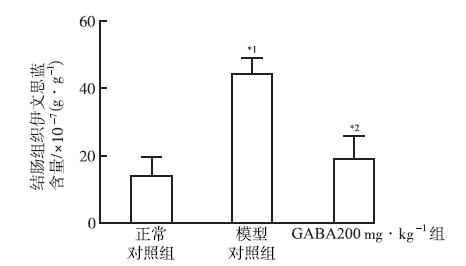
为观察GABA对于实验性结肠炎引起的肠黏膜渗透性的影响,进行大鼠伊文思蓝肠黏膜渗透性实验。实验结果见
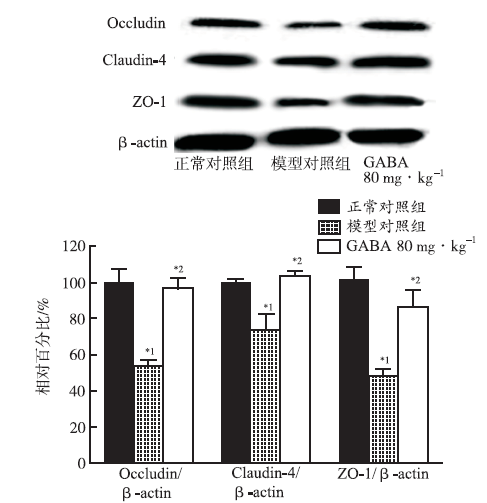
通过WB法观察实验性结肠炎各组大鼠肠黏膜屏障连接蛋白表达情况。结果见
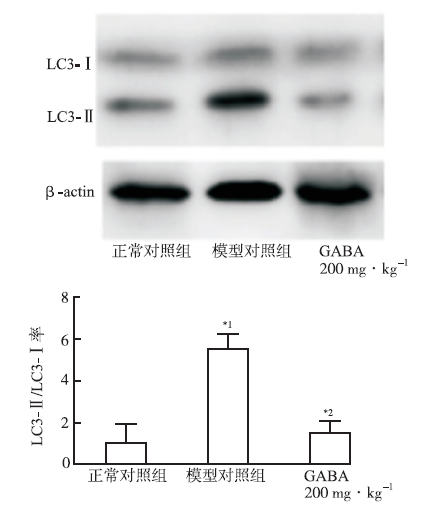
为观察GABA对于LPS刺激下Caco-2自噬的影响,免疫印迹法测定LPS刺激下Caco-2细胞中LC3蛋白表达情况,LC3蛋白表达情况以LC3Ⅱ与LC3Ⅰ的比值表示。实验结果见
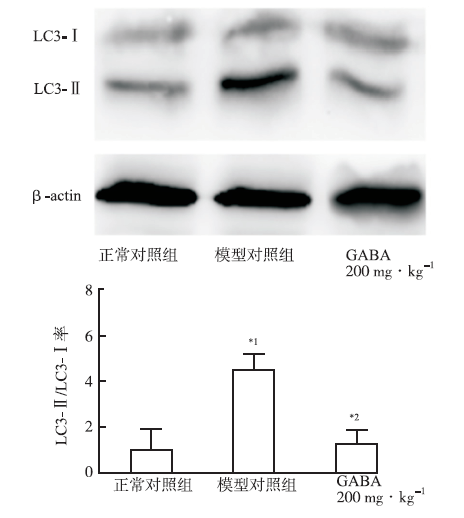
为观察GABA对于TNBS-乙醇溶液诱导的实验性结肠炎结肠组织自噬的影响,免疫印迹法测定TNBS-乙醇溶液诱导的实验性结肠炎结肠组织中LC3蛋白表达情况,LC3蛋白表达情况以LC3Ⅱ与LC3Ⅰ的比值表示。实验结果见
肠黏膜屏障功能异常是IBD发病的分子基础,IBD发病时肠黏膜屏障功能异常,肠腔内抗原物质向肠黏膜固有层移位。而抗原引起的肠道促炎因子的释放,又会进一步损伤肠道上皮细胞,破坏肠黏膜屏障[11,12]。肠黏膜通透性增高可能是IBD 的原发因素。因此,增加肠黏膜屏障可能为防治IBD提供新的治疗手段。
GABA药物治疗已经被用于焦虑、戒酒、癫痫,以及诱导镇静、麻醉。GABA能信号系统不仅在中枢系统发挥着重要的作用,在外周系统中也起重要的调控作用[13]。其在脾脏、胃、肝脏、肺以及血液单核细胞中都有功能性表达[14]。在免疫系统中,GABA能系统可以调控炎症反应。GABA受体已被证实在免疫细胞上存在,可降低外周巨噬细胞炎症因子的产生[15]。笔者尚未见国内有GABA与炎症性肠病的相关报道。而国外已有研究报道,GABA能用于炎症性肠病的防治[16]。但是GABA是否能保护黏膜屏障,及其作用机制均需进一步研究。TNBS-乙醇溶液诱导的大鼠结肠炎组织学改变的许多特点与人类IBD相似。GABA能够改善大鼠体质量变化、结肠指数、DAI评分、肉眼组织学损伤评分等。这些指标能较好反映结肠炎症状和组织学宏观改变的特点和程度[17]。
Caco-2单层模型为公认的肠黏膜屏障体外模型[18]。使用结肠炎的重要诱导因子LPS诱导体外黏膜屏障损伤。GABA能够改善LPS刺激引起的细胞跨膜电阻降低、大分子物质的渗透性增加。为探讨GABA对于实验性结肠炎引起的肠黏膜的影响,进行实验结肠炎大鼠伊文思蓝肠黏膜渗透性实验。证明GABA能够显著改善TNBS-乙醇溶液引起的肠黏膜渗透性改变。
紧密连接蛋白被认为是维持肠黏膜屏障结构完整性的重要组成部分,并在肠黏膜屏障功能的维持中起到决定性作用。构成肠上皮细胞间的紧密连接蛋白主要有Occludin、Claudin、ZO-1等。GABA能够增加紧密连接蛋白Occludin,Claudin-4和ZO-1的表达,通过调节紧密连接蛋白的表达与装配维持肠黏膜屏障功能。
组织细胞通过自噬作用来降解细胞内的受损细胞器、蛋白质和核酸等内容物,并重新利用氨基酸、核糖等代谢物,从而维持细胞稳态。但过度的自噬能够诱导细胞发生程序性死亡[19]。在TNBS-乙醇溶液诱导的实验性结肠炎动物模型,肠道组织出现过度自噬,表明TNBS-乙醇溶液诱导的实验性结肠炎结肠组织自噬显著增强,LC3Ⅱ与LC3Ⅰ的比值是正常对照组的5.4倍。而在LPS刺激的人上皮细胞Caco-2中,LC3Ⅱ与LC3Ⅰ的比值是正常对照组的5.5倍。由此可见,肠黏膜在强烈应激反应过程中出现过度自噬,导致Ⅱ型程序性细胞死亡。GABA能够显著抑制这种过度自噬。GABA对于肠黏膜屏障的保护作用可能与其抑制过度自噬有关。
由此可见,GABA能够抑制过度自噬,有效增强肠道黏膜屏障功能,对实验性结肠炎具有治疗作用。
The authors have declared that no competing interests exist.
| [1] |
Inflammatory bowel diseases(IBD)are a group of chronic inflammatory disorders most commonly affecting young adults.Currently available therapies can result in induction and maintenance of remission,but are not curative and have sometimes important side effects.Advances in basic research in IBD have provided new therapeutic opportunities to target the inflammatory process involved.Gene and cell therapy approaches are suitable to prevent inflammation in the gastrointestinal tract and show therefore potential in the treatment of IBD.In this review,we present the current progress in the field of both gene and cell therapy and future prospects in the context of IBD.Regarding gene therapy,we focus on viral vectors and their applications in preclinical models.The focus for cell therapy is on regulatory T lymphocytes and mesenchymal stromal cells,their potential for the treatment of IBD and the progress made in both preclinical models and clinical trials.
[本文引用:1]
|
| [2] |
Abstract The intestinal epithelium is a single-cell layer that constitutes the largest and most important barrier against the external environment. It acts as a selectively permeable barrier, permitting the absorption of nutrients, electrolytes, and water while maintaining an effective defense against intraluminal toxins, antigens, and enteric flora. The epithelium maintains its selective barrier function through the formation of complex protein-protein networks that mechanically link adjacent cells and seal the intercellular space. The protein networks connecting epithelial cells form 3 adhesive complexes: desmosomes, adherens junctions, and tight junctions. These complexes consist of transmembrane proteins that interact extracellularly with adjacent cells and intracellularly with adaptor proteins that link to the cytoskeleton. Over the past decade, there has been increasing recognition of an association between disrupted intestinal barrier function and the development of autoimmune and inflammatory diseases. In this review we summarize the evolving understanding of the molecular composition and regulation of intestinal barrier function. We discuss the interactions between innate and adaptive immunity and intestinal epithelial barrier function, as well as the effect of exogenous factors on intestinal barrier function. Finally, we summarize clinical and experimental evidence demonstrating intestinal epithelial barrier dysfunction as a major factor contributing to the predisposition to inflammatory diseases, including food allergy, inflammatory bowel diseases, and celiac disease.
[本文引用:1]
|
| [3] |
|
| [4] |
Abstract The current paradigm of inflammatory bowel diseases (IBD), both Crohn's disease (CD) and ulcerative colitis (UC), involves the interaction between environmental factors in the intestinal lumen and inappropriate host immune responses in genetically predisposed individuals. The intestinal mucosal barrier has evolved to maintain a delicate balance between absorbing essential nutrients while preventing the entry and responding to harmful contents. In IBD, disruptions of essential elements of the intestinal barrier lead to permeability defects. These barrier defects exacerbate the underlying immune system, subsequently resulting in tissue damage. The epithelial phenotype in active IBD is very similar in CD and UC. It is characterized by increased secretion of chloride and water, leading to diarrhea, increased permeability via both the transcellular and paracellular routes, and increased apoptosis of epithelial cells. The main cytokine that seems to drive these changes is tumor necrosis factor alpha in CD, whereas interleukin (IL)-13 may be more important in UC. Therapeutic restoration of the mucosal barrier would provide protection and prevent antigenic overload due to intestinal eakiness. Here we give an overview of the key players of the intestinal mucosal barrier and review the current literature from studies in humans and human systems on mechanisms underlying mucosal barrier dysfunction in IBD. (Inflamm Bowel Dis 2011;)
[本文引用:1]
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
DOI:10.1002/path.2749
URL
[本文引用:1]
|
| [10] |
|
| [11] |
Abstract Epithelial and endothelial tight junctions act as a rate-limiting barrier between an organism and its environment. Continuing studies have highlighted the regulation of the tight junction barrier by cytokines. Elucidation of this interplay is vital for both the understanding of physiological tight junction regulation and the etiology of pathological conditions. This review will focus on recent advances in our understanding of the molecular mechanisms of tight junctions modulation by cytokines.
[本文引用:1]
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
Although an extensive body of literature confirmed -aminobutyric acid (GABA) as mediator within the enteric nervous system (ENS) controlling gastrointestinal (GI) function, the true significance of GABAergic signalling in the gut is still a matter of debate. GABAergic cells in the bowel include neuronal and endocrine-like cells, suggesting GABA as modulator of both motor and secretory GI activity. GABA effects in the GI tract depend on the activation of ionotropic GABAA and GABAC receptors and metabotropic GABAB receptors, resulting in a potential noteworthy regulation of both the excitatory and inhibitory signalling in the ENS. However, the preservation of GABAergic signalling in the gut could not be limited to the maintenance of physiologic intestinal activity. Indeed, a series of interesting studies have suggested a potential key role of GABA in the promising field of neuroimmune interaction, being involved in the modulation of immune cell activity associated with different systemic and enteric inflammatory conditions. Given the urgency of novel therapeutic strategies against chronic immunity-related pathologies, i.e. multiple sclerosis and Inflammatory Bowel Disease, an in-depth comprehension of the enteric GABAergic system in health and disease could provide the basis for new clinical application of nerve-driven immunity. Hence, in the attempt to drive novel researches addressing both the physiological and pathological importance of the GABAergic signalling in the gut, we summarized current evidence on GABA and GABA receptor function in the different parts of the GI tract, with particular focus on the potential involvement in the modulation of GI motility and inflammation.
[本文引用:1]
|
| [17] |
DOI:10.1002/path.2749
URL
[本文引用:1]
|
| [18] |
|
| [19] |
哺乳动物雷帕霉素靶蛋白( mTOR)是一种保守的蛋白激酶。当真核细胞缺乏营养时,可以通过抑制mTOR来诱导自噬。作为细胞生长的重要调节因素,当营养条件、生长环境和应激状况发生变化时,mTOR在协调细胞生长与自噬的平衡过程中发挥关键作用,是调节细胞自噬的一个关键因素,但是其潜在的机制尚不十分清楚。mTOR活性主要受PI3K/Akt和LKB1/AMPK信号通路支配,并且通过调节自噬相关基因来调控自噬。在神经变性疾病的不同发病阶段,mTOR活性的调节至关重要。本文综述了mTOR调控自噬的相关机制及其对帕金森氏病、阿尔茨海默病和亨廷顿病的重要影响。
[本文引用:1]
|


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}