1.Department of Respiratory Medicine, Lihuili Hospital, Ningbo Medical Center, Ningbo 315000, China
2.State Key Laboratory for Diagnosis and Treatment of Infectious Disease, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, China
The spread of multidrug-resistant or pandrug-resistant gram-negative bacteria. Because of the slow development of new antibiotics, polymyxins are increasingly used as a last option for such infections.Therefore, this paper reviews the latest progress in the the pharmacological properties, pharmacokinetics/ pharmacodynamics, toxicity and clinical application of polymyxins to provide references the challenges for its optimal use.
目前针对PMB的药动学研究并不多。第一项针对PMB的PK研究发现其分布容积和半衰期分别为47.2 L和13.6 h [14]。在不同肾功能水平的患者中,PMB的清除率个体差异较小。值得注意的是,PMB由于本身就具有抗菌活性,无需转化,因此它能够更快地达到血药浓度高峰,并且PK的个体差异相较CMS小很多,即使是在肾功能差异很大的患者中[15]。这就意味着完善PMB的PK数据能够帮助临床优化给药方案,使初始剂量的选择更简单且更易预测,避免亚血药浓度治疗。
表2
根据不同肾功能水平达到2 mg·L-1稳态血药浓度所需的每日CMS和PMB剂量
Tab.2
The daily doses of CMS and PMB to achieve steady state plasma concentration of 2 mg·L-1 based on different creatinine clearance
内生肌酐清除率/ (mL·min-1)
CMS/ (mg·d-1)
PMB/ (mg·kg-1·d-1)
0~<10
316~352
2.5~3.0
10~<20
388
2.5~3.0
20~<50
424~532
2.5~3.0
50~<80
592~720
2.5~3.0
≥80
720~872
2.5~3.0
表2
根据不同肾功能水平达到2 mg·L-1稳态血药浓度所需的每日CMS和PMB剂量
Tab.2
The daily doses of CMS and PMB to achieve steady state plasma concentration of 2 mg·L-1 based on different creatinine clearance
2 临床应用现状
2.1 临床缺乏高质量研究结果,疗效不确定
多粘菌素的临床研究大部分局限于回顾性研究和小型的前瞻性研究,关于多粘菌素联合方案的价值一直存在着争议。联合治疗的主要原因是体外实验数据显示该方案能获得潜在的协同作用并阻止异质性耐药菌株的产生。QURESHI等[25]发现最初分离出的多粘菌素敏感鲍曼不动杆菌在接受CMS单一治疗后都出现了耐药株。而后面PAUL等[26]进行的一项随机对照研究发现CMS单药和联合治疗的临床失败率差异无统计学意义[156/198,79% vs 152/208,73%;RR 0.93,95%CI(0.83-1.03)]。可能需要依据感染的部位、严重程度、病原菌及患者的基础情况等进行综合的考量。
Infectious Diseases Society of America.The 10×'20 initiative: pursuing a global commitment to develop 10 new antibacterial drugs by 2020[J].Clin Infect Dis,2010,50(8):1081-1083.
The time has come for a global commitment to develop new antibacterial drugs. Current data document the impending disaster due to the confluence of decreasing investment in antibacterial drug research and development concomitant with the documented rapid increase in the level of resistance to currently licensed drugs. Despite the good faith efforts of many individuals, professional societies, and governmental agencies, the looming crisis has only worsened over the past decade.
FALAGAS ME,KASIAKOU SK.Colistin: The revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections[J].Clin Infect Dis,2005,40(9):1333-1341.
The emergence of multidrug-resistant gram-negative bacteria and the lack of new antibiotics to combat them have led to the revival of polymyxins, an old class of cationic, cyclic polypeptide antibiotics. Polymyxin B and polymyxin E (colistin) are the 2 polymyxins used in clinical practice. Most of the reintroduction of polymyxins during the last few years is related to colistin. The polymyxins are active against selected gram-negative bacteria, including Acinetobacter species, Pseudomonas aeruginosa, Klebsiella species, and Enterobacter species. These drugs have been used extensively worldwide for decades for local use. However, parenteral use of these drugs was abandoned approximately 20 years ago in most countries, except for treatment of patients with cystic fibrosis, because of reports of common and serious nephrotoxicity and neurotoxicity. Recent studies of patients who received intravenous polymyxins for the treatment of serious P. aeruginosa and Acinetobacter baumannii infections of various types, including pneumonia, bacteremia, and urinary tract infections, have led to the conclusion that these antibiotics have acceptable effectiveness and considerably less toxicity than was reported in old studies.
PETERSON AA,HANCOCKR E W,MCGROARTYE J.Binding of polycationic antibiotics and polyamines to lipopolysaccharides of pseudomonas-aeruginosa[J].J Bacteriol,1985,164(3):1256-1261.
Polycations, such as aminoglycoside and peptide antibiotics, and naturally occurring polyamines were found to bind to the lipopolysaccharide of Pseudomonas aeruginosa and alter its packing arrangement. Binding of cations was measured by the displacement of a cationic spin probe from lipopolysaccharide into the aqueous environment upon addition of competitive cations. The level of probe displacement was dependent on the concentration and charge of the competing cation, with the more highly charged cations being more effective at displacing probe. The relative affinity of several antibiotics for lipopolysaccharide correlated with their ability to increase outer membrane permeability, while the relative affinity of several polyamines correlated with their ability to stabilize the outer membrane. Probe mobility within the lipopolysaccharide head group was shown to be decreased by cationic antibiotics and unaltered or increased by polyamines. We propose that antibiotic permeability and disruption of outer membrane integrity by polycationic antibiotics results from binding of the antibiotic to anionic groups on lipopolysaccharide with a consequent change in the conformation of lipopolysaccharide aggregate structure.
ZHANGL,DHILLONP,YANH,et al.Interactions of bacterial cationic peptide antibiotics with outer and cytoplasmic membranes of pseudomonas aeruginosa[J].Antimicrob Agents Chemother,2000,44(12):3317-3321.
Polymyxins B and E1 and gramicidin S are bacterium-derived cationic antimicrobial peptides. The polymyxins were more potent than gramicidin S against Pseudomonas aeruginosa, with MICs of 0.125 to 0. 25 and 8 microg/ml, respectively. These peptides differed in their affinities for binding to lipopolysaccharide, but all were able to permeabilize the outer membrane of wild-type P. aeruginosa PAO1 strain H103, suggesting differences in their mechanisms of self-promoted uptake. Gramicidin S caused rapid depolarization of the bacterial cytoplasmic membrane at concentrations at which no killing was observed within 30 min, whereas, conversely, the concentrations of the polymyxins that resulted in rapid killing resulted in minimal depolarization. These data indicate that the depolarization of the cytoplasmic membrane by these peptides did not correlate with bacterial cell lethality.
ZHANGY,WANGQ,YINY,et al.Epidemiology of carba-penem-resistant enterobacteriaceae infections: Report from the china cre network[J].Antimicrob Agents Chemother,2018,62(2).doi:10.1128/AAC.01882-17.
Saprochaete capitata, formerly known as Geotrichum capitatum, is an emerging fungal pathogen with low susceptibility to echinocandins. Here, we report the nucleotide sequence of the S. capitata hot spot 1 region of the FKS gene (FKS HS1), which codifies for the catalytic subunit of β-1,3-d-glucan synthase, the target of echinocandins. For that purpose, we first designed degenerated oligonucleotide primers derived from conserved flanking regions of the FKS1 HS1 segment of 12 different fungal species. Interestingly, analysis of the translated FKS HS1 sequences of 12 isolates of S. capitata revealed that all of them exhibited the same F-to-L substitution in a position that is highly related to reduced echinocandin susceptibility.
LIU YY,WANGY,WALSH TR,et al.Emergence of plasmid-mediated colistin resistance mechanism mcr-1 in animals and human beings in china: A microbiological and molecular biological study[J].Lancet Infect Dis,2016,16(2):161-168.
Until now, polymyxin resistance has involved chromosomal mutations but has never been reported via horizontal gene transfer. During a routine surveillance project on antimicrobial resistance in commensal Escherichia coli from food animals in China, a major increase of colistin resistance was observed. When an E coli strain, SHP45, possessing colistin resistance that could be transferred to another strain, was isolated from a pig, we conducted further analysis of possible plasmid-mediated polymyxin resistance. Herein, we report the emergence of the first plasmid-mediated polymyxin resistance mechanism, MCR-1, in Enterobacteriaceae.
WANGY,TIAN GB,ZHANGR,et al.Prevalence, risk factors,outcomes,and molecular epidemiology of mcr-1-positive enterobacteriaceae in patients and healthy adults from china: An epidemiological and clinical study[J].Lancet Infect Dis,2017,17(4):390-399.
The mcr-1 gene confers transferable colistin resistance. mcr-1-positive Enterobacteriaceae (MCRPE) have attracted substantial medical, media, and political attention; however, so far studies have not addressed their clinical impact. Herein, we report the prevalence of MCRPE in human infections and carriage, clinical associations of mcr-1-positive Escherichia coli (MCRPEC) infection, and risk factors for MCRPEC carriage.
XUA,ZHENGB,XU YC,et al.National epidemiology of carbapenem-resistant and extensively drug-resistant gram-negative bacteria isolated from blood samples in china in 2013[J].Clin Microbiol Infect,2016,22:S1-S8.
Although antimicrobial resistance poses a great challenge to clinicians in China, there are limited antimicrobial resistance data on Gram-negative bacteria nationwide. We investigated the phenotypic characteristics of carbapenem-resistant Escherichia coli (CREC) and Klebsiella pneumoniae (CRKP) as well as extensively drug-resistant strains of Pseudomonas aeruginosa (XDRPA) and Acinetobacter baumannii (XDRAB) isolated from blood cultures in China. Data were collected on 24113 isolates from the China surveillance of antimicrobial resistance program in 2013, which comprised 208 hospitals located in all seven administrative regions of China. Minimum inhibitory concentrations (MICs) for common antimicrobials were determined by commercial automated systems available at local hospitals, and associations with geographic and clinical distributions was further studied. The overall prevalence of CREC, CRKP, XDRAB and XDRPA strains was 1.0, 5.5, 13.7 and 4.2%, respectively. Except for CREC, which did not differ greatly by region, the prevalence of the remaining three strains varied significantly across regions. The highest prevalence of CRKP (10.6%) and XDRAB (13.1%) were found in the pediatric group, and higher prevalence of all four target strains was found in the intensive care unit. For imipenem, 55.8% of CREC and 22.9% of CRKP strains had MICs of ≤4 μg/mL, while 97.4% XDRAB and 84% XDRPA isolates had MICs of ≥16 μg/mL. All CREC, CRKP and 81.2% of XDRAB strains were susceptible to tigecycline, with MIC90 values of 0.5, 2 and 4 μg/mL, respectively. In conclusion, a high prevalence of CRKP and XDRAB has emerged in China, especially in children and in the intensive care unit.
HINDLER JA,HUMPHRIES RM.Colistin mic variability by method for contemporary clinical isolates of multidrug-resistant gram-negative bacilli[J].J Clin Microbiol,2013,51(6):1678-1684.
In vitro evaluation of colistin susceptibility is fraught with complications, due in part to the inherent cationic properties of colistin. In addition, no reference method has been defined against which to compare the results of colistin susceptibility testing. This study systematically evaluated the available methods for colistin MIC testing in two phases. In phase I, colistin MICs were determined in 107 fresh clinical isolates of multidrug-resistant (MDR) Gram-negative bacilli (GNB) by broth microdilution with polysorbate 80 (BMD-T), broth macrodilution (TDS), and the Etest. In phase II, 50 of these isolates, 10 of which were colistin resistant, were tested in parallel using BMD-T, TDS, agar dilution, broth microdilution without polysorbate 80 (BMD), and the TREK Gram-negative extra MIC format (GNXF) Sensititre. The Etest was also performed on these 50 isolates using Mueller-Hinton agar (MHA) from three different manufacturers. Colistin MIC results obtained from the five methods were compared to the MIC results obtained using BMD-T, the method that enables the highest nominal concentration of colistin in the test medium. Essential agreement ranged from 34% (BMD) to 83% (TDS), whereas categorical agreement was >90% for all methods except for BMD, which was 88%. Very major errors (VMEs) (i.e., false susceptibility) for the Etest were found in 47 to 53% of the resistant isolates, depending on the manufacturer of the MHA that was used. In contrast, VMEs were found for 10% (n = 1) of the resistant isolates by BMD and 0% of the isolates by the TDS, agar dilution, and Sensititre methods. Based on these data, we urge clinical laboratories to be aware of the variable results that can occur when using different methods for colistin MIC testing and, in particular, to use caution with the Etest.
LIJ,NATION RL,TURNIDGE JD,et al.Colistin: The reemerging antibiotic for multidrug-resistant gram-negative bacterial infections[J].Lancet Infect Dis,2006,6(9):589-601.
Increasing multidrug resistance in Gram-negative bacteria, in particular Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae, presents a critical problem. Limited therapeutic options have forced infectious disease clinicians and microbiologists to reappraise the clinical application of colistin, a polymyxin antibiotic discovered more than 50 years ago. We summarise recent progress in understanding the complex chemistry, pharmacokinetics, and pharmacodynamics of colistin, the interplay between these three aspects, and their effect on the clinical use of this important antibiotic. Recent clinical findings are reviewed, focusing on evaluation of efficacy, emerging resistance, potential toxicities, and combination therapy. In the battle against rapidly emerging bacterial resistance we can no longer rely entirely on the discovery of new antibiotics; we must also pursue rational approaches to the use of older antibiotics such as colistin.
PLACHOURASD,KARVANENM,FRIBERG LE,et al.Population pharmacokinetic analysis of colistin methanesulfonate and colistin after intravenous administration in critically ill patients with infections caused by gram-negative bacteria[J].Antimicro Agents Chemother,2009,53(8):3430-3436.
Colistin is used to treat infections caused by multidrug-resistant gram-negative bacteria (MDR-GNB). It is administered intravenously in the form of colistin methanesulfonate (CMS), which is hydrolyzed in vivo to the active drug. However, pharmacokinetic data are limited. The aim of the present study was to characterize the pharmacokinetics of CMS and colistin in a population of critically ill patients. Patients receiving colistin for the treatment of infections caused by MDR-GNB were enrolled in the study; however, patients receiving a renal replacement therapy were excluded. CMS was administered at a dose of 3 million units (240 mg) every 8 h. Venous blood was collected immediately before and at multiple occasions after the first and the fourth infusions. Plasma CMS and colistin concentrations were determined by a novel liquid chromatography-tandem mass spectrometry method after a rapid precipitation step that avoids the significant degradation of CMS and colistin. Population pharmacokinetic analysis was performed with the NONMEM program. Eighteen patients (6 females; mean age, 63.6 years; mean creatinine clearance, 82.3 ml/min) were included in the study. For CMS, a two-compartment model best described the pharmacokinetics, and the half-lives of the two phases were estimated to be 0.046 h and 2.3 h, respectively. The clearance of CMS was 13.7 liters/h. For colistin, a one-compartment model was sufficient to describe the data, and the estimated half-life was 14.4 h. The predicted maximum concentrations of drug in plasma were 0.60 mg/liter and 2.3 mg/liter for the first dose and at steady state, respectively. Colistin displayed a half-life that was significantly long in relation to the dosing interval. The implications of these findings are that the plasma colistin concentrations are insufficient before steady state and raise the question of whether the administration of a loading dose would benefit critically ill patients.
GARONZIK SM,LIJ,THAMLIKITKULV,et al.Popula-tion pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients[J].Antimicro Agents Chemother,2011,55(7):3284-3294.
With increasing clinical emergence of multidrug-resistant Gram-negative pathogens and the paucity of new agents to combat these infections, colistin (administered as its inactive prodrug colistin methanesulfonate [CMS]) has reemerged as a treatment option, especially for critically ill patients. There has been a dearth of pharmacokinetic (PK) data available to guide dosing in critically ill patients, including those on renal replacement therapy. In an ongoing study to develop a population PK model for CMS and colistin, 105 patients have been studied to date; these included 12 patients on hemodialysis and 4 on continuous renal replacement therapy. For patients not on renal replacement, there was a wide variance in creatinine clearance, ranging from 3 to 169 ml/min/1.73 m(2). Each patient was treated with a physician-selected CMS dosage regimen, and 8 blood samples for PK analysis were collected across a dosage interval on day 3 or 4 of therapy. A linear PK model with two compartments for CMS and one compartment for formed colistin best described the data. Covariates included creatinine clearance on the total clearance of CMS and colistin, as well as body weight on the central volume of CMS. Model-fitted parameter estimates were used to derive suggested loading and maintenance dosing regimens for various categories of patients, including those on hemodialysis and continuous renal replacement. Based on our current understanding of colistin PK and pharmacodynamic relationships, colistin may best be used as part of a highly active combination, especially for patients with moderate to good renal function and/or for organisms with MICs of ≥ 1.0 mg/liter.
KWA AL,LIM TP,LOW JG,et al.Pharmacokinetics of polymyxin b1 in patients with multidrug-resistant gram-negative bacterial infections[J].Diagn Microbiol Infect Dis,2008,60(2):163-167.
Polymyxin B is increasingly used clinically for the treatment of multidrug-resistant Gram-negative infections, despite very limited understanding of its disposition in humans. The disposition of intravenous polymyxin B1 in 9 adult patients was characterized. Random blood samples (specifically timed in relation to the dose administered) were obtained, and the serum concentrations of polymyxin B1 were assayed using a validated methodology by liquid chromatography mass spectroscopy. The serum concentration profiles of all the patients were analyzed by a population pharmacokinetic analysis using the nonparametric adaptive grid program. The mean volume of distribution and elimination half-life were found to be 47.2 L and 13.6 h, respectively. This is the 1st case series to date in which the pharmacokinetics of polymyxin B1 after intravenous administration are described. The results of the series in conjunction with pharmacodynamic and susceptibility surveillance studies could facilitate an approach to the design of optimal dosing regimens.
SANDRI AM,LANDERSDORFER CB,JACOBJ, et al.Population pharmacokinetics of intravenous polymyxin b in critically ill patients: implications for selection of dosage regimens[J].Clin Infect Dis,2013,57(4):524-531.
Background. Polymyxin B is a last-line therapy for multidrug-resistant gram-negative bacteria. There is a dearth of pharmacokinetic data to guide dosing in critically ill patients. Methods. Twenty-four critically ill patients were enrolled and blood/urine samples were collected over a dosing interval at steady state. Polymyxin B concentrations were measured by liquid chromatography-tandem mass spectrometry. Population pharmacokinetic analysis and Monte Carlo simulations were conducted. Results. Twenty-four patients aged 21-87 years received intravenous polymyxin B (0.45-3.38 mg/kg/day). Two patients were on continuous hemodialysis, and creatinine clearance in the other patients was 10-143 mL/min. Even with very diverse demographics, the total body clearance of polymyxin B when scaled by total body weight (population mean, 0.0276 L/hour/kg) showed remarkably low interindividual variability (32.4% coefficient of variation). Polymyxin B was predominantly nonrenally cleared with median urinary recovery of 4.04%. Polymyxin B total body clearance did not show any relationship with creatinine clearance (r(2) = 0.008), APACHE II score, or age. Median unbound fraction in plasma was 0.42. Monte Carlo simulations revealed the importance of initiating therapeutic regimens with a loading dose. Conclusions. Our study showed that doses of intravenous polymyxin B are best scaled by total body weight. Importantly, dosage selection of this drug should not be based on renal function.
OWEN RJ,LIJ,NATION RL,et al.In vitro pharmacody-namics of colistin against acinetobacter baumannii clinical isolates[J].J Antimicrob Chemother,2007,59(3):473-477.
Colistin is being increasingly used for treatment of infections caused by multidrug-resistant Gram-negative bacteria, including Acinetobacter baumannii.
BERGEN PJ,BULITTA JB,FORRESTA,et al.Pharma-cokinetic/pharmacodynamic investigation of colistin against pseudomonas aeruginosa using an in vitro model[J].Antimicro Agents Chemother,2010,54(9):3783-3789.
Colistin plays a key role in treatment of serious infections by Pseudomonas aeruginosa. The aims of this study were to (i) identify the pharmacokinetic/pharmacodynamic (PK/PD) index (i.e., the area under the unbound concentration-time curve to MIC ratio [fAUC/MIC], the unbound maximal concentration to MIC ratio [fC(max)/MIC], or the cumulative percentage of a 24-h period that unbound concentrations exceed the MIC [fT(&gt;MIC)]) that best predicts colistin efficacy and (ii) determine the values for the predictive PK/PD index required to achieve various magnitudes of killing effect. Studies were conducted in a one-compartment in vitro PK/PD model for 24 h using P. aeruginosa ATCC 27853, PAO1, and the multidrug-resistant mucoid clinical isolate 19056 muc. Six intermittent dosing intervals, with a range of fC(max) colistin concentrations, and two continuous infusion regimens were examined. PK/PD indices varied from 0.06 to 18 for targeted fC(max)/MIC, 0.36 to 312 for fAUC/MIC, and 0 to 100% for fT(&gt;MIC). A Hill-type model was fit to killing effect data, which were expressed as the log(10) ratio of the area under the CFU/ml curve for treated regimens versus control. With fC(max) values equal to or above the MIC, rapid killing was observed following the first dose; substantial regrowth occurred by 24 h with most regimens. The overall killing effect was best correlated with fAUC/MIC (R(2) = 0.931) compared to fC(max)/MIC (R(2) = 0.868) and fT(&gt;MIC) (R(2) = 0.785). The magnitudes of fAUC/MIC required for 1- and 2-log(10) reductions in the area under the CFU/ml curve relative to growth control were 22.6 and 30.4, 27.1 and 35.7, and 5.04 and 6.81 for ATCC 27853, PAO1, and 19056 muc, respectively. The PK/PD targets identified will assist in designing optimal dosing strategies for colistin.
MARKOUN,MARKANTONIS SL,DIMITRAKISE, et al.Colistin serum concentrations after intravenous administration in critically ill patients with serious multidrug-resistant,gram-negative bacilli infections: A prospective,open-label,uncontrolled study[J].Clin Ther,2008,30(1):143-151.
The emergence of multidrug-resistant nosocomial pathogens, such as Pseudomonas aeruginosa and Acinetobacter baumannii, has led to the revival of the systemic use of antimicrobial agent colistin in critically ill patients, but only limited data are available to define its pharmacokinetic profile in these patients.
DUDHANI RV,TURNIDGE JD,COULTHARDK, et al.Elucidation of the pharmacokinetic/pharmacodynamic determinant of colistin activity against pseudomonas aeruginosa in murine thigh and lung infection models[J].Antimicro Agents Chemother,2010,54(3):1117-1124.
Colistin is increasingly used as last-line therapy against Gram-negative pathogens. The pharmacokinetic (PK)/pharmacodynamic (PD) index that best correlates with the efficacy of colistin remains undefined. The activity of colistin against three strains of Pseudomonas aeruginosa was studied in neutropenic mouse thigh and lung infection models. The PKs of unbound colistin were determined from single-dose PK studies together with extensive plasma protein binding analyses. Dose-fractionation studies were conducted over 24 h with a dose range of 5 to 160 mg/kg of body weight/day. The bacterial burden in the thigh or lung was measured at 24 h after the initiation of treatment. Relationships between antibacterial effect and measures of exposure to unbound (f) colistin (area under the concentration-time curve [fAUC/MIC], maximum concentration of drug in plasma [fC(max)]/MIC, and the time that the concentration in plasma is greater than the MIC [fT &gt; MIC]) were examined by using an inhibitory sigmoid maximum-effect model. Nonlinearity in the PKs of colistin, including its plasma protein binding, was observed. The PK/PD index that correlated best with its efficacy was fAUC/MIC in both the thigh infection model (R(2) = 87%) and the lung infection model (R(2) = 89%). The fAUC/MIC targets required to achieve 1-log and 2-log kill against the three strains were 15.6 to 22.8 and 27.6 to 36.1, respectively, in the thigh infection model, while the corresponding values were 12.2 to 16.7 and 36.9 to 45.9 in the lung infection model. The findings of this in vivo study indicate the importance of achieving adequate time-averaged exposure to colistin. The results will facilitate efforts to define the more rational design of dosage regimens for humans.
LIM LM,LYN,ANDERSOND,et al.Resurgence of colistin: a review of resistance,toxicity,pharmaco-dynamics,and dosing[J].Pharmacotherapy,2010,30(12):1279-1291.
Colistin is a polymyxin antibiotic that was discovered in the late 1940s for the treatment of gram-negative infections. After several years of clinical use, its popularity diminished because of reports of significant nephrotoxicity and neurotoxicity. Recently, the antibiotic has resurfaced as a last-line treatment option for multidrug-resistant organisms such as Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae. The need for antibiotics with coverage of these gram-negative pathogens is critical because of their high morbidity and mortality, making colistin a very important treatment option. Unfortunately, however, resistance to colistin has been documented among all three of these organisms in case reports. Although the exact mechanism causing colistin resistance has not been defined, it is hypothesized that the PmrA-PmrB and PhoP-PhoQ genetic regulatory systems may play a role. Colistin dosages must be optimized, as colistin is a last-line treatment option; in addition, suboptimal doses have been linked to the development of resistance. The lack of pharmacokinetic and pharmacodynamic studies and no universal harmonization of dose units, however, have made it difficult to derive optimal dosing regimens and specific dosing guidelines for colistin. In critically ill patients who may have multiorgan failure, renal insufficiency may alter colistin pharmacokinetics. Therefore, dosage alterations in this patient population are imperative to achieve maximal efficacy and minimal toxicity. With regard to colistin toxicity, most studies show that nephrotoxicity is reversible and less frequent than once thought, and neurotoxicity is rare. Further research is needed to fully understand the impact that the two regulatory systems have on resistance, as well as the dosages of colistin needed to inhibit and overcome these developing patterns.
LEE HJ,BERGEN PJ,BULITTA JB,et al.Synergistic activity of colistin and rifampin combination against multidrug-resistant acinetobacter baumannii in an in vitro pharmacokinetic/pharmacodynamic model[J].Antimicrob Agents Chemother,2013,57(8):3738-3745.
Combination therapy may be required for multidrug-resistant (MDR) Acinetobacter baumannii. This study systematically investigated bacterial killing and emergence of colistin resistance with colistin and rifampin combinations against MDR A. baumannii. Studies were conducted over 72 h in an in vitro pharmacokinetic (PK)/pharmacodynamic (PD) model at inocula of ~10(6) and ~10(8) CFU/ml using two MDR clinical isolates of A. baumannii, FADDI-AB030 (colistin susceptible) and FADDI-AB156 (colistin resistant). Three combination regimens achieving clinically relevant concentrations (constant colistin concentration of 0.5, 2, or 5 mg/liter and a rifampin maximum concentration [C(max)] of 5 mg/liter every 24 hours; half-life, 3 h) were investigated. Microbiological response was measured by serial bacterial counts. Population analysis profiles assessed emergence of colistin resistance. Against both isolates, combinations resulted in substantially greater killing at the low inoculum; combinations containing 2 and 5 mg/liter colistin increased killing at the high inoculum. Combinations were additive or synergistic at 6, 24, 48, and 72 h with all colistin concentrations against FADDI-AB030 and FADDI-AB156 in, respectively, 8 and 11 of 12 cases (i.e., all 3 combinations) at the 10(6)-CFU/ml inoculum and 8 and 7 of 8 cases with the 2- and 5-mg/liter colistin regimens at the 10(8)-CFU/ml inoculum. For FADDI-AB156, killing by the combination was ~2.5 to 7.5 and ~2.5 to 5 log(10) CFU/ml greater at the low inoculum (all colistin concentrations) and high inoculum (2 and 5 mg/liter colistin), respectively. Emergence of colistin-resistant subpopulations was completely suppressed in the colistin-susceptible isolate with all combinations at both inocula. Our study provides important information for optimizing colistin-rifampin combinations against colistin-susceptible and -resistant MDR A. baumannii.
BERGEN PJ,TSUJI BT,BULITTA JB,et al.Synergistic killing of multidrug-resistant pseudomonas aeruginosa at multiple inocula by colistin combined with doripenem in an in vitro pharmacokinetic/pharmacodynamic model[J].Antimicrob Agents Chemother,2011,55(12):5685-5695.
Combination therapy may be required for multidrug-resistant (MDR) Pseudomonas aeruginosa. The aim of this study was to systematically investigate bacterial killing and emergence of colistin resistance with colistin and doripenem combinations against MDR P. aeruginosa. Studies were conducted in a one-compartment in vitro pharmacokinetic/pharmacodynamic model for 96 h at two inocula (~10(6) and ~10(8) CFU/ml) against a colistin-heteroresistant reference strain (ATCC 27853) and a colistin-resistant MDR clinical isolate (19147 n/m). Four combinations utilizing clinically achievable concentrations were investigated. Microbiological response was examined by log changes and population analysis profiles. Colistin (constant concentrations of 0.5 or 2 mg/liter) plus doripenem (peaks of 2.5 or 25 mg/liter every 8 h; half-life, 1.5 h) substantially increased bacterial killing against both strains at the low inoculum, while combinations containing colistin at 2 mg/liter increased activity against ATCC 27853 at the high inoculum; only colistin at 0.5 mg/liter plus doripenem at 2.5 mg/liter failed to improve activity against 19147 n/m at the high inoculum. Combinations were additive or synergistic against ATCC 27853 in 16 and 11 of 20 cases (4 combinations across 5 sample points) at the 10(6)- and 10(8)-CFU/ml inocula, respectively; the corresponding values for 19147 n/m were 16 and 9. Combinations containing doripenem at 25 mg/liter resulted in eradication of 19147 n/m at the low inoculum and substantial reductions in regrowth (including to below the limit of detection at ∼50 h) at the high inoculum. Emergence of colistin-resistant subpopulations of ATCC 27853 was substantially reduced and delayed with combination therapy. This investigation provides important information for optimization of colistin-doripenem combinations.
DERIS ZZ,YU HH,DAVISK,et al.The combination of colistin and doripenem is synergistic against klebsiella pneumoniae at multiple inocula and suppresses colistin resistance in an in vitro pharmacokinetic/pharmacodynamic model[J].Antimicrob Agents Chemother,2012,56(10):5103-5112.
Multidrug-resistant (MDR) Klebsiella pneumoniae may require combination therapy. We systematically investigated bacterial killing with colistin and doripenem mono- and combination therapy against MDR K. pneumoniae and emergence of colistin resistance. A one-compartment in vitro pharmacokinetic/pharmacodynamic model was employed over a 72-h period with two inocula (∼10(6) and ∼10(8) CFU/ml); a colistin-heteroresistant reference strain (ATCC 13883) and three clinical isolates (colistin-susceptible FADDI-KP032 [doripenem resistant], colistin-heteroresistant FADDI-KP033, and colistin-resistant FADDI-KP035) were included. Four combinations utilizing clinically achievable concentrations were investigated. Microbiological responses were examined by determining log changes and population analysis profiles (for emergence of colistin resistance) over 72 h. Against colistin-susceptible and -heteroresistant isolates, combinations of colistin (constant concentration regimens of 0.5 or 2 mg/liter) plus doripenem (steady-state peak concentration [C(max)] of 2.5 or 25 mg/liter over 8 h; half-life, 1.5 h) generally resulted in substantial improvements in bacterial killing at both inocula. Combinations were additive or synergistic against ATCC 13883, FADDI-KP032, and FADDI-KP033 in 9, 9, and 14 of 16 cases (4 combinations at 6, 24, 48, and 72 h) at the 10(6)-CFU/ml inoculum and 14, 11, and 12 of 16 cases at the 10(8)-CFU/ml inoculum, respectively. Combinations at the highest dosage regimens resulted in undetectable bacterial counts at 72 h in 5 of 8 cases (4 isolates at 2 inocula). Emergence of colistin-resistant subpopulations in colistin-susceptible and -heteroresistant isolates was virtually eliminated with combination therapy. Against the colistin-resistant isolate, colistin at 2 mg/liter plus doripenem (C(max), 25 mg/liter) at the low inoculum improved bacterial killing. This investigation provides important information for optimization of colistin-doripenem combinations.
TSUJI BT,POGUE JM,ZAVASCKI AP,et al.Interna-tional consensus guidelines for the optimal use of the polymyxins endorsed by the american college of clinical pharmacy(accp),european society of clinical microbiology and infectious diseases(escmid),infectious diseases society of america(idsa),international society for anti-infective pharmacology(isap),society of critical care medicine(sccm),and society of infectious diseases pharmacists(sidp)[J].Pharmacotherapy,2019,39(1):10-39.
The polymyxin antibiotics colistin (polymyxin E) and polymyxin B became available in the 1950s and thus did not undergo contemporary drug development procedures. Their clinical use has recently resurged, assuming an important role as salvage therapy for otherwise untreatable gram-negative infections. Since their reintroduction into the clinic, significant confusion remains due to the existence of several different conventions used to describe doses of the polymyxins, differences in their formulations, outdated product information, and uncertainties about susceptibility testing that has led to lack of clarity on how to optimally utilize and dose colistin and polymyxin B. We report consensus therapeutic guidelines for agent selection and dosing of the polymyxin antibiotics for optimal use in adult patients, as endorsed by the American College of Clinical Pharmacy (ACCP), Infectious Diseases Society of America (IDSA), International Society of Anti-Infective Pharmacology (ISAP), Society for Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). The European Society for Clinical Microbiology and Infectious Diseases (ESCMID) endorses this document as a consensus statement. The overall conclusions in the document are endorsed by the European Committee on Antimicrobial Susceptibility Testing (EUCAST). We established a diverse international expert panel to make therapeutic recommendations regarding the pharmacokinetic and pharmacodynamic properties of the drugs and pharmacokinetic targets, polymyxin agent selection, dosing, dosage adjustment and monitoring of colistin and polymyxin B, use of polymyxin-based combination therapy, intrathecal therapy, inhalation therapy, toxicity, and prevention of renal failure. The treatment guidelines provide the first ever consensus recommendations for colistin and polymyxin B therapy that are intended to guide optimal clinical use.
With an increase in the use of colistin methansulfonate (CMS) to treat carbapenem-resistant Acinetobacter baumannii infections, colistin resistance is emerging.
PAULM,DAIKOS GL,DURANTE-MANGONIE,et al.Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant gram-negative bacteria: an open-label,randomised controlled trial[J].Lancet Infect Dis,2018,18(4):391-400.
Colistin-carbapenem combinations are synergistic in vitro against carbapenem-resistant Gram-negative bacteria. We aimed to test whether combination therapy improves clinical outcomes for adults with infections caused by carbapenem-resistant or carbapenemase-producing Gram-negative bacteria.
GHANNAM DE,RODRIGUEZ GH,RAAD II,et al.Inhaled aminoglycosides in cancer patients with ventilator-associated gram-negative bacterial pneumonia: safety and feasibility in the era of escalating drug resistance[J].Eur J Clin Microbiol,2009,28(3):253-259.
We sought to evaluate the safety and feasibility of inhaled aminoglycosides or colistin in cancer patients with ventilator-associated pneumonia (VAP) due to Gram-negative bacteria (GNB). A retrospective case-matched study was obtained after obtaining IRB approval in patients at the intensive care unit at our NCI-designated comprehensive cancer center between 1999 and 2005. Sixteen patients with GNB-VAP who received inhaled aminoglycosides or colistin were compared with 16 patients who had received these antibiotics intravenously alone. Eligible patients were required to have received at least six doses of inhaled therapy, or 3 or more days of intravenous therapy. Clinical Pulmonary Infection Scores were used to assess pneumonia severity. Standard ATS criteria were used to define VAP. Patients treated with inhaled antibiotics were less likely to have received corticosteroids (13% vs 50%; P < 0.02) and had a higher median baseline creatinine level (0.85 vs 0.6 mg/dL; P < 0.02) than patients treated intravenously. Pseudomonas aeruginosa (69%) was the most common cause of VAP. There were no serious adverse events associated with inhaled antibiotics. Patients who received these antibiotics intravenously developed renal dysfunction (31%); none of the patients treated with inhaled antibiotics developed nephrotoxicity (P ≤ 0.04). Patients treated with inhaled antibiotics were more likely to have complete resolution of clinical (81% vs 31% in the intravenous antibiotic group; P < 0.01) and microbiologic infection (77% vs 8% in the intravenous antibiotic group: P < 0.0006). In a multivariate analysis adjusted for corticosteroid use, inhaled antibiotic therapy was predictive of complete clinical resolution (odds ratio [OR], 6.3; 95% confidence interval [CI], 1.1, 37.6; P < 0.04) and eradication of causative organisms (OR 36.7; 95% CI, 3.3, 412.2; P < 0.003). In critically ill cancer patients with Gram-negative VAP, inhaled aminoglycosides were tolerated without serious toxicity and may lead to improved outcome.
FALAGAS ME,SIEMPOS II,RAFAILIDIS PI, et al.Inhaled colistin as monotherapy for multidrug-resistant gram(-) nosocomial pneumonia:a case series[J].Resp Med,2009,103(5):707-713.
Reports of patients with polymyxin-only susceptible gram-negative nosocomial pneumonia treated with inhaled, but without concurrent intravenous, colistin are rare.
MICHALOPOULOSA,FOTAKISD,VIRTZILIS, et al.Aerosolized colistin as adjunctive treatment of ventilator-associated pneumonia due to multidrug-resistant gram-negative bacteria: a prospective study[J].Resp Med,2008,102(3):407-412.
A new genus and species of platyrrhine primate, Nuciruptor rubricae, are added to the increasingly diverse primate fauna from the middle Miocene of La Venta, Columbia. This species displays a number of dental and gnathic features indicating that it is related to living and extinct Pitheciinae (extant Callicebus, Pithecia, Chiropotes, Cacajao, and the Colombian middle Miocene Cebupithecia sarmientoi). Nuciruptor is markedly more derived than Callicebus but possesses a less derived mandibular form and incisor-canine complex than extant and extinct pitheciins (Cebupithecia, Pithecia, Chiropotes, and Cacajao), suggesting that it is a primitive member of the tribe Pitheciini within the larger monophyletic Pitheciinae. Nuciruptor has procumbent and moderately elongate lower incisors and low-crowned molars, suggesting that is was a seed predator, as are living pitheciins. Its estimated body size of approximately 2.0 kg places it within the size range of extant pitheciines. The dental and gnathic morphology of Nuciruptor clarifies several aspects of dental character evolution in Pitheciinae and makes it less likely that the enigmatic Mohanamico hershkovitzi (m. Miocene, Columbia) is a pitheciin.
VALACHISA,SAMONISG,KOFTERIDI DR.The role of aerosolized colistin in the treatment of ventilator-associated pneumonia: A systematic review and metaanalysis[J].Critical Care Med,2015,43(3):527-533.
The present meta-analysis and systematic review evaluated the efficacy and safety of aerosolized colistin as adjunctive therapy to i.v. antimicrobials or as monotherapy in the treatment of ventilator-associated pneumonia.
QURESHI ZA,PATERSON DL,POTOSKI BA, et al.Treatment outcome of bacteremia due to kpc-producing klebsiella pneumoniae: Superiority of combination antimicrobial regimens[J].Antimicrob Agents Chemother,2012,56(4):2108-2113.
Klebsiella pneumoniae producing Klebsiella pneumoniae carbapenemase (KPC) has been associated with serious infections and high mortality. The optimal antimicrobial therapy for infection due to KPC-producing K. pneumoniae is not well established. We conducted a retrospective cohort study to evaluate the clinical outcome of patients with bacteremia caused by KPC-producing K. pneumoniae. A total of 41 unique patients with blood cultures growing KPC-producing K. pneumoniae were identified at two medical centers in the United States. Most of the infections were hospital acquired (32; 78%), while the rest of the cases were health care associated (9; 22%). The overall 28-day crude mortality rate was 39.0% (16/41). In the multivariate analysis, definitive therapy with a combination regimen was independently associated with survival (odds ratio, 0.07 [95% confidence interval, 0.009 to 0.71], P = 0.02). The 28-day mortality was 13.3% in the combination therapy group compared with 57.8% in the monotherapy group (P = 0.01). The most commonly used combinations were colistin-polymyxin B or tigecycline combined with a carbapenem. The mortality in this group was 12.5% (1/8). Despite in vitro susceptibility, patients who received monotherapy with colistin-polymyxin B or tigecycline had a higher mortality of 66.7% (8/12). The use of combination therapy for definitive therapy appears to be associated with improved survival in bacteremia due to KPC-producing K. pneumoniae.
TUMBARELLOM,VIALEP,VISCOLIC,et al.Predictors of mortality in bloodstream infections caused by klebsiella pneumoniae carbapenemase-producing k.Pneumoniae: Importance of combination therapy[J].Clin Infect Dis,2012,55(7):943-950.
Background. The spread of Klebsiella pneumoniae (Kp) strains that produce K. pneumoniae carbapenemases (KPCs) has become a significant problem, and treatment of infections caused by these pathogens is a major challenge for clinicians. Methods. In this multicenter retrospective cohort study, conducted in 3 large Italian teaching hospitals, we examined 125 patients with bloodstream infections (BSIs) caused by KPC-producing Kp isolates (KPC-Kp) diagnosed between 1 January 2010 and 30 June 2011. The outcome measured was death within 30 days of the first positive blood culture. Survivor and nonsurvivor subgroups were compared to identify predictors of mortality. Results. The overall 30-day mortality rate was 41.6%. A significantly higher rate was observed among patients treated with monotherapy (54.3% vs 34.1% in those who received combined drug therapy; P = .02). In logistic regression analysis, 30-day mortality was independently associated with septic shock at BSI onset (odds ratio [OR]: 7.17; 95% confidence interval [CI]: 1.65-31.03; P = .008); inadequate initial antimicrobial therapy (OR: 4.17; 95% CI: 1.61-10.76; P = .003); and high APACHE III scores (OR: 1.04; 95% CI: 1.02-1.07; P < .001). Postantibiogram therapy with a combination of tigecycline, colistin, and meropenem was associated with lower mortality (OR: 0.11; 95% CI:.02-. 69; P = .01). Conclusions. KPC-Kp BSIs are associated with high mortality. To improve survival, combined treatment with 2 or more drugs with in vitro activity against the isolate, especially those also including a carbapenem, may be more effective than active monotherapy.
FALAGASME,RAFAILIDISPI,IOANNIDOUE, et al.Colistin therapy for microbiologically documented multidrug-resistant gram-negative bacterial infections: A retrospective cohort study of 258 patients[J].Int J Antimicrob Agents,2010,35(2):194-199.
It is unclear whether the effectiveness of polymyxins depends on the site of infection, the responsible pathogen, dosage, and monotherapy vs. combination therapy. We investigated colistin therapy in a large, retrospective, single-centre, cohort study. Primary analysis outcomes were infection outcome, survival and nephrotoxicity. Over a 7-year period (October 2000 to October 2007), 258 patients received intravenous (i.v.) colistin for at least 72h for microbiologically documented multidrug-resistant Gram-negative bacterial infections, comprising 170 (65.9%) Acinetobacter baumannii, 68 (26.4%) Pseudomonas aeruginosa, 18 (7.0%) Klebsiella pneumoniae, 1 (0.4%) Stenotrophomonas maltophilia and 1 (0.4%) Enterobacter cloacae. Cure of infection occurred in 79.1% of patients, nephrotoxicity in 10% and hospital survival in 65.1%. In the multivariate analysis, independent predictors of survival were colistin average daily dose [adjusted odds ratio (aOR)=1.22, 95% confidence interval (CI) 1.05-1.42] and cure of infection (aOR=9, 95% CI 3.6-23.1), whilst the proportion of creatinine change (aOR=0.21, 95% CI 0.1-0.45), Acute Physiology and Chronic Health Evaluation (APACHE) II score (aOR=0.89, 95% CI 0.84-0.95) and haematological disease (aOR=0.23, 95% CI 0.08-0.66) were associated with mortality. Effectiveness of colistin was not dependent on the type of pathogen. No independent predictors for nephrotoxicity were observed. The findings of the largest cohort study to date on i.v. colistin show that colistin is a valuable antibiotic with acceptable nephrotoxicity and considerable effectiveness that depends on the daily dosage and infection site.
AYDEMIRH,AKDUMAND,PISKINN,et al.Colistin vs.The combination of colistin and rifampicin for the treatment of carbapenem-resistant acinetobacter baumannii ventilator-associated pneumonia[J].Epidemiol Infect,2013,141(6):1214-1222.
The aim of this study was to compare the responses of colistin treatment alone vs. a combination of colistin and rifampicin in the treatment of ventilator-associated pneumonia (VAP) caused by a carbapenem-resistant A. baumannii strain. Forty-three patients were randomly assigned to one of two treatment groups. Although clinical (P=0.654), laboratory (P=0.645), radiological (P=0.290) and microbiological (P=0.597) response rates were better in the combination group, these differences were not significant. However, time to microbiological clearance (3.1+/-0.5 days, P=0.029) was significantly shorter in the combination group. The VAP-related mortality rates were 63.6% (14/22) and 38.1% (8/21) for the colistin and the combination groups (P=0.171), respectively. Our results suggest that the combination of colistin with rifampicin may improve clinical and microbiological outcomes of VAP patients infected with A. baumannii.
DURANTE-MANGONIE,SIGNORIELLOG, ANDINIR,et al.Colistin and rifampicin compared with colistin alone for the treatment of serious infections due to extensively drug-resistant acinetobacter baumannii: A multicenter,randomized clinical trial[J].Clin Infect Dis,2013,57(3):349-358.
Background. Extensively drug-resistant (XDR) Acinetobacter baumannii may cause serious infections in critically ill patients. Colistin often remains the only therapeutic option. Addition of rifampicin to colistin may be synergistic in vitro. In this study, we assessed whether the combination of colistin and rifampicin reduced the mortality of XDR A. baumannii infections compared to colistin alone. Methods. This multicenter, parallel, randomized, open-label clinical trial enrolled 210 patients with life-threatening infections due to XDR A. baumannii from intensive care units of 5 tertiary care hospitals. Patients were randomly allocated (1: 1) to either colistin alone, 2 MU every 8 hours intravenously, or colistin (as above), plus rifampicin 600 mg every 12 hours intravenously. The primary end point was overall 30-day mortality. Secondary end points were infection-related death, microbiologic eradication, and hospitalization length. Results. Death within 30 days from randomization occurred in 90 (43%) subjects, without difference between treatment arms (P = .95). This was confirmed by multivariable analysis (odds ratio, 0.88 [95% confidence interval,.46-1.69], P = .71). A significant increase of microbiologic eradication rate was observed in the colistin plus rifampicin arm (P = .034). No difference was observed for infection-related death and length of hospitalization. Conclusions. In serious XDR A. baumannii infections, 30-day mortality is not reduced by addition of rifampicin to colistin. These results indicate that, at present, rifampicin should not be routinely combined with colistin in clinical practice. The increased rate of A. baumannii eradication with combination treatment could still imply a clinical benefit.
MAKRISD,PETINAKIE,TSOLAKIV,et al.Colistin versus colistin combined with ampicillin-sulbactam for multiresistant acinetobacter baumannii ventilator-associated pneumonia treatment: An open-label prospective study[J].Indian J Crit Care M,2018,22(2):67-77.
Retrospective studies have reported good clinical success rates using colistin as monotherapy to treat Acinetobacter baumannii ventilator-associated pneumonia (VAP), comparable to that obtained with colistin combined with other antibiotics. However, inadequate penetration into the pulmonary parenchyma for colistin has been shown in animal models.
LINDEN PK,KUSNES,COLEYK,et al.Use of parenteral colistin for the treatment of serious infection due to antimicrobial-resistant pseudomonas aeruginosa[J].Clin Infect Dis,2003,37(11):E154-E160.
Serious infection due to strains of Pseudomonas aeruginosa that exhibit resistance to all common antipseudomonal antimicrobials increasingly is a serious problem. Colistin was used as salvage therapy for 23 critically ill patients with multidrug-resistant P. aeruginosa infection. Twenty-two patients who had septic shock (n=14) and/or renal failure (n=21) received mechanical ventilatory support at baseline. The most common types of infection were pneumonia (n=18) and intra-abdominal infection (n=5). Colistin was administered for a median of 17 days (range, 7-36 days). Seven patients died during therapy, at a median of 17 days (range, 4-26 days) after initiation of treatment. A favorable clinical response was observed in 14 patients (61%); only 3 patients experienced relapse. Bacteremia was the only significant factor associated with treatment failure (P=.02). One patient manifested diffuse weakness that resolved after temporary cessation of colistin therapy. Colistin provides an important salvage therapeutic option for patients with otherwise untreatable serious P. aeruginosa infection.
FURTADOGHC,D'AZEVEDOP A,SANTOSA F, et al.Intravenous polymyxin b for the treatment of nosocomial pneumonia caused by multidrug-resistant pseudomonas aeruginosa[J].Int J Antimicrob Ag,2007,30(4):315-319.
Nosocomial pneumonia caused by multidrug-resistant (MDR) Pseudomonas aeruginosa is becoming increasingly prevalent throughout the world. The use of polymyxins to treat these infections has greatly increased. We analysed 74 patients with nosocomial pneumonia caused by MDR P. aeruginosa who were treated with polymyxin B. A favourable outcome was observed in 35 patients (47.3%). A case-control study was performed to assess the variables associated with an unfavourable outcome. The presence of acute respiratory distress syndrome (odds ratio (OR)=11.29, 95% confidence interval (CI) 2.64-48.22; P=0.001) and septic shock (OR=4.81, 95% CI 1.42-16.25; P=0.01) were independently associated with an unfavourable outcome in patients with nosocomial pneumonia due to MDR P. aeruginosa. Our study demonstrated that polymyxin B is a reliable antimicrobial drug, but only as salvage therapy, for nosocomial pneumonia caused by MDR P. aeruginosa.
ZUSMANO,ALTUNINS,KOPPELF,et al.Polymyxin monotherapy or in combination against carbapenem-resistant bacteria: Systematic review and meta-analysis[J].J Antimicrob Chemother,2017,72(1):29-39.
The objective of this study was to summarize available data on polymyxin-based combination therapy or monotherapy for carbapenem-resistant Gram-negative bacteria.
KALIL AC,METERSKY ML,KLOMPASM,et al.Mana-gement of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the american thoracic society[J].Clin Infect Dis,2016,63(5):e61-e111.
It is important to realize that guidelines cannot always account for individual variation among patients. They are not intended to supplant physician judgment with respect to particular patients or special clinical situations. IDSA considers adherence to these guidelines to be voluntary, with the ultimate determination regarding their application to be made by the physician in the light of each patient's individual circumstances.These guidelines are intended for use by healthcare professionals who care for patients at risk for hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP), including specialists in infectious diseases, pulmonary diseases, critical care, and surgeons, anesthesiologists, hospitalists, and any clinicians and healthcare providers caring for hospitalized patients with nosocomial pneumonia. The panel's recommendations for the diagnosis and treatment of HAP and VAP are based upon evidence derived from topic-specific systematic literature reviews.
KOCH-WESERJ,SIDELVW,FEDERMANEB,et al.Adverse effects of sodium colistimethate.Manifestations and specific reaction rates during 317 courses of therapy[J].Ann Intern Med,1970,72(6):857-868.
DERYKECA,CRAWFORDAJ,UDDINN,et al.Colistin dosing and nephrotoxicity in a large community teaching hospital[J].Antimicrob Agents Chemother,2010,54(10):4503-4505.
Thirty adult patients who received intravenous colistin (5.1 ± 2.4 mg/kg/day) were reviewed to evaluate dosing with respect to nephrotoxicity, which occurred in 10 (33%) patients within the first 5 days of treatment. Excessive colistin dosing was frequent (47%), often (71%) resulted from the use of actual body weight in obese patients, and was associated with higher rates of nephrotoxicity (80% versus 30%, P = 0.019).
KALING,ALPE,COSKUNR,et al.Use of high-dose iv and aerosolized colistin for the treatment of multidrug-resistant acinetobacter baumannii ventilator-associated pneumonia: Do we really need this treatment?[J].J Infect Chemother,2012,18(6):872-877.
In this study we aimed to assess the safety and efficacy of high-dose IV colistin (COL) and aerosolized COL for the treatment of Acinetobacter baumannii ventilator-associated pneumonia (VAP). Critically ill adult patients who received IV COL for multidrug-resistant A. baumannii VAP were evaluated retrospectively. A total of 45 patients were evaluated [15 patients with high-dose COL (2.5 mg/kg every 6 h), 20 patients with normal dose (2.5 mg/kg every 12 h), and 10 patients with low dose, determined according to creatine clearance]. Aerosolized COL was used in 29 patients treated with parenteral COL and 16 patients received only parenteral COL. The clinical response rates on the fifth day were 50, 30, and 27 % with the normal, low, and high doses, respectively. However, the clinical response rates at the end of the therapy had declined to 30, 30, and 7 % with the normal, low, and high doses, respectively. The bacteriological clearance rates at the end of the therapy were 65, 75, and 64 %, with the normal, low, and high doses, respectively. With the aerosolized COL, the clinical response rates on the fifth day and at the end of the therapy were 35 and 14 %, whereas these rates were 44 and 38 % without the aerosolized COL. Bacteriological clearance rates with and without the aerosolized COL were 76 and 69 %, respectively. The nephrotoxicity rate was 40 % for the high-dose COL, whereas it was 35 % for the normal dose, and 20 % for the low-dose COL. In conclusion, higher doses of COL and aerosolized COL had no advantages over lower doses in alleviating multidrug-resistant A. baumannii VAP. Moreover, the higher doses and the aerosolized COL increased the nephrotoxicity risk and seemed not to be safe.
FALAGAS ME,FRAGOULIS KN,KASIAKOU SK, et al.Nephrotoxicity of intravenous colistin: a prospective evaluation[J].Int J Antimicrob Ag,2005,26(6):504-507.
Twenty-one patients who received intravenous colistimethate sodium (CMS) for at least 7 days for the treatment of multidrug-resistant Gram-negative bacterial infections were included in a prospective cohort study at 'Henry Dunant' Hospital in Athens, Greece. The mean (+/- standard deviation) and median daily doses, cumulative doses and duration of treatment of intravenous CMS were, respectively, 5.5 (+/- 1.9) and 6 million IU, 90.2 (+/- 52.0) and 72 million IU, and 17.7 (+/- 11.7) and 15 days (range 7-54 days). Three patients (14.3%) developed nephrotoxicity during treatment with CMS. The cumulative dose of administered CMS was statistically correlated with the difference in values of serum creatinine between the end and start of CMS treatment (r = 0.6, P = 0.004 by Spearman's test).
FALAGAS ME,KASIAKOU SK.Toxicity of polymyxins: a systematic review of the evidence from old and recent studies[J].Crit Care,2006,10(1):R27.
The increasing problem of multidrug-resistant gram-negative bacteria causing severe infections and the shortage of new antibiotics to combat them has led to the re-evaluation of polymyxins. These antibiotics were discovered from different species of Bacillus polymyxa in 1947; only two of them, polymyxin B and E (colistin), have been used in clinical practice. Their effectiveness in the treatment of infections due to susceptible gram-negative bacteria, including Pseudomonas aeruginosa and Acinetobacter baumannii, has not been generally questioned. However, their use was abandoned, except in patients with cystic fibrosis, because of concerns related to toxicity.
PHEK,LEEY,MCDANELD PM,et al.In vitro assess-ment and multicenter cohort study of comparative nephrotoxicity rates associated with colistimethate versus polymyxin b therapy[J].Antimicrob Agents Chemother,2014,58(5):2740-2746.
Despite concerns of nephrotoxicity, polymyxin antibiotics often remain the only susceptible agents for multidrug-resistant (MDR) Gram-negative bacteria. Colistin has been more commonly used clinically due to a perceived safety benefit. We compared the nephrotoxicity of colistin to polymyxin B. The in vitro cytotoxicity of colistin was compared to polymyxin B in two mammalian renal cell lines. To validate the clinical relevance of the findings, we evaluated adult patients with normal renal function who received a minimum of 72 h of polymyxin therapy in a multicenter study. The primary outcome was the prevalence of nephrotoxicity, as defined by the RIFLE (risk, injury, failure, loss, end-stage kidney disease) criteria. Colistin exhibited an in vitro cytotoxicity profile similar to polymyxin B. A total of 225 patients (121 receiving colistimethate, 104 receiving polymyxin B) were evaluated. Independent risk factors for colistimethate-associated nephrotoxicity included age (odds ratio [OR], 1.04; 95% confidence interval [CI], 1.00 to 1.07; P = 0.03), duration of therapy (OR 1.08; 95% CI, 1.02 to 1.15; P = 0.02), and daily dose by ideal body weight (OR 1.40; 95% CI, 1.05 to 1.88; P = 0.02). In contrast, cystic fibrosis was found to be a protective factor in patients who received colistimethate (OR, 0.03; 95% CI, 0.001 to 0.79; P = 0.04). In a matched analysis based on the risk factors identified (n = 76), the prevalence of nephrotoxicity was higher with colistimethate than with polymyxin B (55.3% versus 21.1%; P = 0.004). Polymyxin B was not found to be more nephrotoxic than colistin and may be the preferred polymyxin for MDR infections. A prospective study comparing the two polymyxins directly is warranted.
OLIVEIRA MS,PRADOG V B,COSTAS F,et al. Poly-myxin b and colistimethate are comparable as to efficacy and renal toxicity[J].Diagn Micr Infec Dis,2009,65(4):431-434.
We compared 41 patients who received colistimethate with 41 who received polymyxin B for the treatment of serious infections caused by carbapenem-resistant Acinetobacter spp. and found both polymyxins have similar efficacy and toxicity.
BOSSO JA,LIPTAK CA,SEILHEIMER DK,et al.Toxi-city of colistin in cystic-fibrosis patients[J].Dicp Ann Pharmac,1991,25(11):1168-1170.
Pulmonary exacerbations of cystic fibrosis associated with strains of Pseudomonas aeruginosa that are resistant to multiple antibiotics are becoming increasingly common. The search for treatment alternatives continues and may include the reexamination of older antibiotics. Colistin sulfate is a polypeptide antibiotic with good activity against P. aeruginosa. Although its use was largely discontinued in the early 1970s because of reports of frequent renal and neurologic toxicity, intravenous colistin is often prescribed at our institution for patients with P. aeruginosa resistant to multiple-drug therapy. We prospectively monitored 19 patients during 21 courses of colistin therapy to identify the character and incidence of this agent's toxicity. Only one case of renal toxicity occurred. Six cases of neurotoxicity occurred, which were characterized by perioral paresthesia, ataxia, or both. The rate of intolerable renal adverse effects secondary to colistin therapy was appreciably lower among these patients than that reported previously for other patients. It appears that intravenous colistin can be considered for cystic fibrosis patients with strains of P. aeruginosa that are resistant to more commonly used antibiotics.
FALAGAS ME,RIZOSM,BLIZIOTIS IA,et al.Toxicity after prolonged(more than four weeks) administration of intravenous colistin[J].BMC Infect Dis,2005,5:1.
Background
The intravenous use of polymyxins has been considered to be associated with considerable nephrotoxicity and neurotoxicity. For this reason, the systemic administration of polymyxins had been abandoned for about 20 years in most areas of the world. However, the problem of infections due to multidrug-resistant (MDR) Gram-negative bacteria such us Pseudomonas aeruginosa and Acinetobacter baumanniii has led to the re-use of polymyxins. Our objective was to study the toxicity of prolonged intravenous administration of colistin (polymyxin E).
DALFINOL,PUNTILLOF,MOSCAA,et al.High-dose,extended-interval colistin administration in critically ill patients: is this the right dosing strategy? A preliminary study[J].Clin Infect Dis,2012,54(12):1720-1726.
Background. Gram-negative bacteria susceptible only to colistin (COS) are emerging causes of severe nosocomial infections, reviving interest in the use of colistin. However, consensus on the most effective way to administer colistin has not yet been reached. Methods. All patients who had sepsis due to COS gram-negative bacteria or minimally susceptible gram-negative bacteria and received intravenous colistimethate sodium (CMS) were prospectively enrolled. The CMS dosing schedule was based on a loading dose of 9 MU and a 9-MU twice-daily fractioned maintenance dose, titrated on renal function. For each CMS course, clinical cure, bacteriological clearance, daily serum creatinine clearance, and estimated creatinine clearance were recorded. Results. Twenty-eight infectious episodes due to Acinetobacter baumannii (46.4%), Klebsiella pneumoniae (46.4%), and Pseudomonas aeruginosa (7.2%) were analyzed. The main types of infection were bloodstream infection (64.3%) and ventilator-associated pneumonia (35.7%). Clinical cure was observed in 23 cases (82.1%). Acute kidney injury developed during 5 treatment courses (17.8%), did not require renal replacement therapy, and subsided within 10 days from CMS discontinuation. No correlation was found between variation in serum creatinine level (from baseline to peak) and daily and cumulative doses of CMS, and between variation in serum creatinine level (from baseline to peak) and duration of CMS treatment. Conclusions. Our study shows that in severe infections due to COS gram-negative bacteria, the high-dose, extended-interval CMS regimen has a high efficacy, without significant renal toxicity.
HORCAJADA JP,SORLIL,LUQUES,et al.Validation of a colistin plasma concentration breakpoint as a predictor of nephrotoxicity in patients treated with colistin methanesulfonate[J].Int J Antimicrob Ag,2016,48(6):725-727.
Nephrotoxicity limits the effective use of colistin for the treatment of multidrug-resistant Gram-negative bacteria (MDR-GNB) infections. We previously defined a steady-state colistin plasma concentration (Css) of 2.42 mg/L that predicted nephrotoxicity at end of treatment (EOT). The objective of this study was to validate this breakpoint in a prospective cohort. This was a multicentre, prospective, observational study conducted at three hospitals with a cohort of patients treated for MDR-GNB infection with colistin methanesulfonate from September 2011 until January 2015. Nephrotoxicity was evaluated at Day 7 and at EOT using the RIFLE criteria. Css values were measured and analysed using HPLC. Taking the previously defined breakpoint for colistin concentration as a criterion, patients were divided into two groups (Css, ≤2.42 mg/L vs. >2.42 mg/L). Sixty-four patients were included. Seven patients (10.9%) had a Css > 2.42 mg/L and were compared with the remaining patients. Bivariate analysis showed that patients with a Css > 2.42 mg/L were older and had a significantly higher incidence of nephrotoxicity at Day 7 and EOT. Although not statistically significant, nephrotoxicity occurred earlier in these patients (6.2 days vs. 9.2 days in patients with lower Css; P = 0.091). Multivariate analysis of nephrotoxicity showed that Css > 2.42 mg/L was the only predictive factor. Nephrotoxicity was more frequent and occurred earlier in patients with colistin plasma concentrations higher than the previously defined breakpoint (2.42 mg/L). Colistin therapeutic drug monitoring should be routinely considered to avoid reaching this toxicity threshold and potential clinical consequences.
LANDERSDORFER CB,NATION RL.Colistin: how should it be dosed for the critically ill?[J].Semin Resp Crit Care,2015,36(1):126-135.
Intravenous colistimethate sodium (CMS) is used to treat infections with multiresistant Gram-negative bacteria. Optimal dosing in patients undergoing continuous renal replacement therapy (CRRT) is unclear. In a prospective study, we determined CMS and colistin pharmacokinetics in 10 critically ill patients requiring CRRT (8 underwent continuous venovenous hemodialysis [CVVHD]; median blood flow, 100 ml/min). Intensive sampling was performed on treatment days 1, 3, and 5 after an intravenous CMS loading dose of 9 million international units (MU) (6 MU if body weight was &lt;60 kg) with a consecutive 3-MU (respectively, 2 MU) maintenance dose at 8 h. CMS and colistin concentrations were determined by liquid chromatography with mass spectroscopy. A model-based population pharmacokinetic analysis incorporating CRRT settings was applied to the observations. Sequential model building indicated a monocompartmental distribution for both CMS and colistin, with interindividual variability in both volume and clearance. Hematocrit was shown to affect the efficacy of drug transfer across the filter. CRRT clearance accounted for, on average, 41% of total CMS and 28% of total colistin clearance, confirming enhanced elimination of colistin compared to normal renal function. Target colistin steady-state trough concentrations of at least 2.5 mg/liter were achieved in all patients receiving 3 MU at 8 h. In conclusion, a loading dose of 9 MU followed after 8 h by a maintenance dose of 3 MU every 8 h independent of body weight is expected to achieve therapeutic colistin concentrations in patients undergoing CVVHD using low blood flows. Colistin therapeutic drug monitoring might help to further ensure optimal dosing in individual patients. (This study has been registered at ClinicalTrials.gov under identifier NCT02081560.).
SORLIL,LUQUES,LIJ,et al.Colistin use in patients with chronic kidney disease: are we underdosing patients?[J].Molecules,2019,24(3).doi:10.3390/molecules24030530.
Simple and rapid detection of DNA single base mismatch or point mutation is of great significance for the diagnosis, treatment, and detection of single nucleotide polymorphism (SNP) in genetic diseases. Homogeneous mutation assays with fast hybridization kinetics and amplified discrimination signals facilitate the automatic detection. Herein we report a quick and cost-effective assay for SNP analysis with a fluorescent single-labeled DNA probe. This convenient strategy is based on the efficient quenching effect and the preferential binding of graphene oxide (GO) to ssDNA over dsDNA. Further, a cationic comb-type copolymer (CCC), poly(l-lysine)-graft-dextran (PLL-g-Dex), significantly accelerates DNA hybridization and strand-exchange reaction, amplifying the effective distinction of the kinetic barrier between a perfect matched DNA and a mismatched DNA. Moreover, in vitro experiments indicate that RAW 264.7 cells cultured on PLL-g-Dex exhibits excellent survival and proliferation ability, which makes this mismatch detection strategy highly sensitive and practical.
Emergence of plasmid-mediated colistin resistance mechanism mcr-1 in animals and human beings in china: A microbiological and molecular biological study
Prevalence, risk factors,outcomes,and molecular epidemiology of mcr-1-positive enterobacteriaceae in patients and healthy adults from china: An epidemiological and clinical study
Population pharmacokinetic analysis of colistin methanesulfonate and colistin after intravenous administration in critically ill patients with infections caused by gram-negative bacteria
Popula-tion pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients
Colistin serum concentrations after intravenous administration in critically ill patients with serious multidrug-resistant,gram-negative bacilli infections: A prospective,open-label,uncontrolled study
Elucidation of the pharmacokinetic/pharmacodynamic determinant of colistin activity against pseudomonas aeruginosa in murine thigh and lung infection models
Synergistic activity of colistin and rifampin combination against multidrug-resistant acinetobacter baumannii in an in vitro pharmacokinetic/pharmacodynamic model
Synergistic killing of multidrug-resistant pseudomonas aeruginosa at multiple inocula by colistin combined with doripenem in an in vitro pharmacokinetic/pharmacodynamic model
The combination of colistin and doripenem is synergistic against klebsiella pneumoniae at multiple inocula and suppresses colistin resistance in an in vitro pharmacokinetic/pharmacodynamic model
Interna-tional consensus guidelines for the optimal use of the polymyxins endorsed by the american college of clinical pharmacy(accp),european society of clinical microbiology and infectious diseases(escmid),infectious diseases society of america(idsa),international society for anti-infective pharmacology(isap),society of critical care medicine(sccm),and society of infectious diseases pharmacists(sidp)
... 多粘菌素的临床研究大部分局限于回顾性研究和小型的前瞻性研究,关于多粘菌素联合方案的价值一直存在着争议.联合治疗的主要原因是体外实验数据显示该方案能获得潜在的协同作用并阻止异质性耐药菌株的产生.QURESHI等[25]发现最初分离出的多粘菌素敏感鲍曼不动杆菌在接受CMS单一治疗后都出现了耐药株.而后面PAUL等[26]进行的一项随机对照研究发现CMS单药和联合治疗的临床失败率差异无统计学意义[156/198,79% vs 152/208,73%;RR 0.93,95%CI(0.83-1.03)].可能需要依据感染的部位、严重程度、病原菌及患者的基础情况等进行综合的考量. ...
Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant gram-negative bacteria: an open-label,randomised controlled trial
2
2018
... 多粘菌素的临床研究大部分局限于回顾性研究和小型的前瞻性研究,关于多粘菌素联合方案的价值一直存在着争议.联合治疗的主要原因是体外实验数据显示该方案能获得潜在的协同作用并阻止异质性耐药菌株的产生.QURESHI等[25]发现最初分离出的多粘菌素敏感鲍曼不动杆菌在接受CMS单一治疗后都出现了耐药株.而后面PAUL等[26]进行的一项随机对照研究发现CMS单药和联合治疗的临床失败率差异无统计学意义[156/198,79% vs 152/208,73%;RR 0.93,95%CI(0.83-1.03)].可能需要依据感染的部位、严重程度、病原菌及患者的基础情况等进行综合的考量. ...
Inhaled aminoglycosides in cancer patients with ventilator-associated gram-negative bacterial pneumonia: safety and feasibility in the era of escalating drug resistance
Predictors of mortality in bloodstream infections caused by klebsiella pneumoniae carbapenemase-producing k.Pneumoniae: Importance of combination therapy
Colistin vs.The combination of colistin and rifampicin for the treatment of carbapenem-resistant acinetobacter baumannii ventilator-associated pneumonia
Colistin and rifampicin compared with colistin alone for the treatment of serious infections due to extensively drug-resistant acinetobacter baumannii: A multicenter,randomized clinical trial
Colistin versus colistin combined with ampicillin-sulbactam for multiresistant acinetobacter baumannii ventilator-associated pneumonia treatment: An open-label prospective study
Mana-gement of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the american thoracic society
Use of high-dose iv and aerosolized colistin for the treatment of multidrug-resistant acinetobacter baumannii ventilator-associated pneumonia: Do we really need this treatment?

 , 肖永红
, 肖永红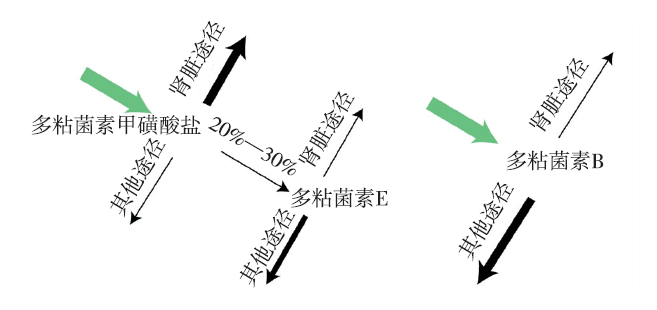

{kind=link}
{kind=link}