中国科技论文统计源期刊 中文核心期刊
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖
美国《化学文摘》《国际药学文摘》
《乌利希期刊指南》
WHO《西太平洋地区医学索引》来源期刊
日本科学技术振兴机构数据库(JST)
第七届湖北十大名刊提名奖

叶酸是一种水溶性维生素,为人体细胞生长和繁殖所必需,可用于治疗由叶酸缺乏引起的贫血,也是孕妇的营养素补充剂。超过50%的新生儿神经管缺陷(neural tube defects,NTDs)病例与妊娠初期叶酸不足有关,补充叶酸可显著降低NTDs的发生率。长期补充叶酸也有助于降低心脑血管疾病的发生风险。
目前,我国临床实践暴露了对叶酸的价值认识不足的问题。有关叶酸的研究很多,但研究质量和结果参差不齐,针对叶酸缺乏的筛查、预防及补充叶酸的适宜人群、时机、剂量、疗程等缺乏统一的标准和规范,给临床使用叶酸带来困扰。
为规范、合理补充叶酸,中国医药教育协会临床合理用药专业委员会、中国医疗保健国际交流促进会高血压分会、中国妇幼保健协会围产营养与代谢专业委员会、中国药理学会治疗药物监测研究专业委员会、中国医药教育协会神经内科专业委员会、中国营养保健食品协会精准营养专业委员会、中国药师协会居家药学服务药师分会、健康中国研究中心药品和健康产品专家委员会组织多学科专家编写了《中国临床合理补充叶酸多学科专家共识》(以下简称《共识》),以探究合理补充叶酸与相关疾病发生、发展的关系,为叶酸在临床中的合理应用提供循证依据和参考。
依据当前的临床研究结果,包括指南、共识、研究文献,结合专家意见形成《共识》意见条目;针对意见条目,依照患者-干预-比较-结局(patient,intervention,comparison,outcome,PICO)原则制订相应的检索策略,检索所有文献。
对所有的检索文献进行分析和质量评价,形成推荐意见。《共识》采用美国心脏协会的证据等级和推荐意见分类,具体见
表1 证据等级
表2 推荐意见分类
叶酸分子结构中有3个亚基:6-甲基蝶啶、4-氨基苯甲酸和谷氨酸[1],相对分子质量为441 000(
叶酸与多种药物存在相互作用,但发生机制各不相同,可发生于吸收、分布、代谢和排泄的各个环节。可以采取必要的措施,如增减剂量、避免联用、延长服药间隔时间等进行处理(
表3 叶酸与多种药物的相互作用及其处理措施
推荐意见:①血清叶酸和红细胞叶酸是评价临床叶酸缺乏/不足的特异性指标(Ⅰ类推荐,B级证据)。②血浆同型半胱氨酸(homocysteine,Hcy) 是评价叶酸功能性缺乏的非特异性指标(Ⅱa类推荐,C级证据)。
叶酸不足/缺乏一般要历经膳食叶酸摄入不足或需要量增加→血清叶酸水平下降→红细胞叶酸水平下降、血清Hcy水平升高→骨髓和其他快速增殖组织巨细胞改变→巨幼红细胞性贫血等多个阶段[20,21,22]。因此,膳食调查、实验室生化检测、体格检查、临床症状和体征等是综合评价个体叶酸状况的主要手段。一般可通过检测血清/血浆、红细胞和尿液中的叶酸水平来评价机体叶酸状况。
血清叶酸被认为是反映近期叶酸营养状况的指标,单独检测血清叶酸水平并不能区分一过性膳食叶酸摄入不足和慢性叶酸缺乏状态;而红细胞叶酸水平可反映慢性或长期(4个月内)叶酸营养状况,更适合于评价叶酸干预效果[23]。叶酸检测方法较多,其中最经典、最可靠的是微生物法[24],其分析性能受叶酸标准物质和所用微生物菌种的影响。其他的叶酸检测方法还包括经典的高效液相色谱法、免疫法、离子捕获法等,其中免疫化学发光法是当前较为便捷的检测方法之一,其可以同时测定血清叶酸和红细胞叶酸水平,检测值可溯源至美国国家标准与技术研究院(National Institute of Standards and Technology,NIST)国家标准品。叶酸缺乏会导致高同型半胱氨酸血症(hyper homocysteinemia,高Hcy血症),后者可作为评价叶酸缺乏的非特异性指标。需注意的是,血清Hcy水平升高受多因素影响(如代谢酶基因变异,维生素B2、维生素B6、维生素B12缺乏,肾功能不全等),如
由于叶酸缺乏可能带来不同的健康风险,据此提出针对不同健康结局目标的叶酸缺乏/不足判定依据[24-25,29-30],如
表4 叶酸缺乏/不足判定依据①
推荐意见:①平衡膳食是改善叶酸营养状况的首选措施(Ⅰ类推荐,B级证据)。②对于叶酸缺乏高危人群和特殊人群,可进一步采取叶酸补充或强化食物等措施改善叶酸营养状况(Ⅱa类推荐,B级证据)。
叶酸推荐摄入量(reco- mmended nutrient intake,RNI)为个体摄入叶酸的目标值,涵盖普通食物中的天然叶酸以及强化食物和营养素补充剂中的化学合成叶酸,二者在体内生物利用率不同,因此需统一转换为膳食叶酸当量(dietary folate equivalent,DFE)。不同生理状态人群的叶酸RNI不一致(附录1)。
附录1 膳食叶酸参考摄入量
对于叶酸缺乏/不足的个体,首先推荐通过平衡膳食改善叶酸营养状况。绿叶蔬菜、豆制品、动物肝脏、瘦肉、蛋类等是叶酸的良好食物来源。依据《预包装食品营养标签通则》(GB 28050-2011)规定,食品中叶酸DFE含量≥120 μg·(100 g)-1(固体)或≥60 μgDFE/100 mL(液体)即可称为“高或富含叶酸”食品,叶酸DFE含量≥60 μg·(100 g)-1(固体)或DFE≥30 μg·(100 mL)-1(液体) 即可称为“含有叶酸”或“叶酸来源”食品[34]。据此标准,富含叶酸的食物包括藜麦、干大豆或杂豆、腐竹、菠菜、茴香、苋菜、动物肝脏、瘦肉、鸭蛋等(附录2)。
附录2 常见食物中叶酸DFE含量[193] μg·(100 g)-1
虽然天然食物中的叶酸相对安全,但由于其结构不稳定(食物加工过程中容易被破坏)、生物利用率较低,且其在体内的吸收利用受药物、乙醇、其他营养素缺乏等因素影响,即使对于一般人群,叶酸摄入量也较难满足RNI;尤其对于叶酸缺乏高危人群,如中国北方地区、贫困农村、冬/春季、孕妇/乳母、长期服用拮抗叶酸代谢药物、大量饮酒、某些疾病、叶酸代谢基因变异等特征人群,应进一步采用叶酸补充或强化食物等措施,以改善叶酸缺乏/不足状况[20,27,35-52]。
叶酸参与氨基酸和核酸的代谢,对细胞增殖、组织分化和机体生长发育均具有重要作用。叶酸在人体内不能合成,仅能从食物中摄取,孕期母体生理性变化和胎儿生长发育等导致对叶酸的需要量增加。
5.1.1 一般人群 推荐意见:(1)无高危因素的妇女,建议从可能妊娠或孕前至少3个月开始,增补叶酸0.4或0.8 mg·d-1,直至妊娠满3个月(Ⅰ类推荐,A级证据)。(2)个性化增补:存在以下情况的妇女,可酌情增加补充剂量或延长孕前增补时间,①居住在北方地区,尤其北方农村地区;②新鲜蔬菜和水果食用量小;③血液叶酸水平低;④备孕时间短(Ⅰ类推荐,B级证据)。(3)建议备孕和孕早期妇女多食用富含叶酸的食物如绿叶蔬菜和新鲜水果,养成健康的生活方式,保持合理体质量,从而降低胎儿发生NTDs的风险(Ⅰ类推荐,B级证据)。
围受孕期叶酸缺乏显著增加NTDs的发生风险[55]。NTDs是指胚胎发育过程中因神经管闭合失败而导致的中枢神经系统出生缺陷,胎儿发病率为1‰~1%,其形成机制非常复杂,是遗传因素和环境因素共同作用的结果。母体叶酸水平不足可能引起胎儿神经管闭合障碍,导致NTDs。多项随机对照试验和系统综述结果表明:孕前和孕期补充叶酸可显著降低NTDs发生风险[56,57,58,59]。一项在德国育龄女性中开展的随机对照试验发现,每日服用叶酸0.8 mg,在4~8周内可达到预防NTDs水平,而每日服用0.4 mg则无法在同样时间内达到该水平[60]。我国北方农村地区妇女血液叶酸水平较低[61,62],一项随机对照试验结果显示,我国北方农村地区育龄妇女服用叶酸0.4 mg·d-1,至少需要3个月,红细胞叶酸水平才能达到预防NTDs的水平[63]。此外,多项病例对照研究结果提示:提高膳食叶酸摄入量,也可使胎儿NTDs发生风险降低30%~60%[64,65]。
孕期叶酸缺乏还增加流产、早产、死胎、巨幼细胞贫血、子··前期等疾病发生风险[66,67],而补充叶酸可降低流产等风险[68]。叶酸是细胞DNA合成过程中的重要辅酶,叶酸缺乏会影响幼红细胞核DNA 的合成,使细胞核的成熟和分裂延缓、停滞,同时因红细胞核浆发育失衡,胞体变大而导致巨幼细胞贫血[66]。叶酸还是蛋氨酸脱甲基形成半胱氨酸时的重要辅酶,其含量与Hcy水平呈负相关。Hcy可通过胎盘影响胎儿的生长发育,诱导胎盘内皮细胞损伤,甚至诱发子··前期[67]。另一方面,叶酸使用过量存在增加妊娠期高血压的潜在风险。有队列研究显示,孕早期至孕中期大剂量(≥0.8 mg·d-1)补充叶酸会增加罹患妊娠期高血压和妊娠期糖尿病的风险[69,70]。
母体叶酸水平还可能与子代孤独症谱系障碍(autism spectrum disorder,ASD)的发生风险相关。观察性研究表明,孕前4周至妊娠8周内补充叶酸可降低子代ASD发生风险[71,72,73]。也有研究认为母体高血叶酸水平和叶酸不足均可能增加ASD风险[74]。此外,有研究显示母体叶酸水平与产后抑郁相关,但目前结论并不一致。
5.1.2 特殊人群 推荐意见:①NTDs生育史妇女建议从可能妊娠或孕前至少1个月开始,增补叶酸4 mg·d-1,直至妊娠满3个月;因国内剂型原因,可增补叶酸5 mg·d-1(Ⅰ类推荐,A级证据)。②夫妻一方患NTDs,或男方既往有NTDs生育史,建议备孕妇女从可能妊娠或孕前至少1个月开始,增补叶酸4 mg·d-1,直至妊娠满3个月;因国内剂型原因,可增补叶酸5 mg·d-1(Ⅰ类推荐,B级证据)。③患先天性脑积水、先天性心脏病、唇腭裂、肢体缺陷、泌尿系统缺陷,或有上述缺陷家族史,或一、二级直系亲属中有NTDs生育史的妇女,建议从可能妊娠或孕前至少3个月开始,增补叶酸0.8~1.0 mg·d-1,直至妊娠满3个月(Ⅰ类推荐,B级证据)。④患糖尿病、肥胖、癫··、胃肠道吸收不良性疾病,或正在服用增加胎儿NTDs发生风险药物(如卡马西平、丙戊酸、苯妥英钠、扑米酮、苯巴比妥、二甲双胍、甲氨蝶呤、柳氮磺吡啶、甲氧苄啶、氨苯蝶啶、考来烯胺等)的妇女,建议从可能妊娠或孕前至少3个月开始,增补叶酸0.8~1.0 mg·d-1,直至妊娠满3个月(Ⅰ类推荐,B级证据)。⑤高Hcy血症妇女,建议增补叶酸至少5 mg·d-1,且在血清Hcy水平降至正常后再受孕,并持续增补叶酸5 mg·d-1,直至妊娠满3个月(Ⅰ类推荐,B级证据)。⑥MTHFR 677位点TT基因型妇女,可根据个体情况酌情增加补充剂量或延长孕前增补时间(Ⅰ类推荐,B级证据)。
特殊人群在备孕和孕早期对叶酸的需求量不同于一般孕妇。存在NTDs生育史、夫妻一方为NTDs,或存在其他NTDs一级、二级亲属者,其胎儿发生NTDs的风险显著升高[80]。英国一项多中心随机对照试验结果显示,对于前次妊娠为NTDs 的妇女,孕前至孕12周增补大剂量叶酸(4 mg·d-1) 可降低72%的NTDs再发风险,同时未发现不良反应[81]。另外一项英国预防NTDs再发的随机对照试验显示,研究组妇女从孕前开始增补叶酸5 mg·d-1,直至妊娠满3个月,也未发现不良反应[82]。
叶酸代谢通路关键酶,如亚甲基四氢叶酸还原酶(methylenetetra hydrofolate reductase,MTHFR) 的基因突变影响叶酸的吸收和代谢[83]。MTHFR 677 位点TT纯合突变与高Hcy血症有关[84],增加NTDs 及其他不良妊娠结局的发生风险[85]。针对多项临床试验的荟萃分析结果显示,每日增补0.5~5.0 mg 叶酸可使血Hcy水平降低约25%[86]。
研究表明,孕早期服用某些抗惊厥药、降糖药、抗菌药、利尿药、调血脂药等均能增加胎儿NTDs 的发生风险[87,88,89,90]。抗癫··药如苯妥英钠、卡马西平、丙戊酸钠等均可降低血清叶酸水平。观察性研究表明,癫··妇女孕前补充叶酸可降低其后代发生孤独症的风险[91],但能否提高子代智商结论并不一致[92,93]。孕前肥胖和孕前糖尿病也增加胎儿NTDs 及其他先天缺陷的发生风险[94,95,96,97],而增补叶酸可降低胎儿NTDs的发生风险[95,97]。
孕前和孕期的药物和毒物暴露也增加子代罹患ASD的风险,而补充叶酸可降低相关风险。孕期每日摄入0.8 mg叶酸且同时有室内农药暴露史的孕妇,其子代出生后患ASD的风险是无农药暴露史孕妇的1.7倍,而叶酸摄入量不足0.8 mg·d-1的孕妇,其子代患ASD的风险增加了2.5倍[98]。
综上,特殊人群的备孕和孕早期需根据具体情况进行个性化叶酸补充。
推荐意见:推荐孕中、晚期妇女除经常摄入富含叶酸的食物外,继续增补叶酸(Ⅰ类推荐,B级证据)。
孕中、晚期叶酸增补剂量建议为0.4 mg·d-1(Ⅱa类推荐,C级证据)。
推荐意见:推荐哺乳期妇女除经常摄入富含叶酸的食物外,继续增补叶酸(Ⅰ类推荐,C级证据)。
哺乳期叶酸增补剂量建议为0.4 mg·d-1(Ⅱa类推荐,C级证据)。
由于泌乳需要,哺乳期妇女对营养素的需求普遍增加,因此,相较于正常成人,乳母更易缺乏叶酸。研究显示,哺乳期妇女血液叶酸水平低于未哺乳妇女[101]。横断面研究结果显示,在资源匮乏地区,50%以上的产妇存在叶酸缺乏[102],另一项研究指出,即使食用叶酸强化食品,仍有约32%的妇女存在哺乳期叶酸缺乏[103]。我国2013年一项全国性调查研究发现,乳母血清叶酸状况总体改善,但居住在北方农村地区、少数民族、哺乳初期、收入较低、食用过多薯类和较少谷米类的乳母叶酸缺乏风险较高[32]。观察性研究表明,未补充叶酸的孕妇和哺乳期妇女叶酸相关性贫血(巨幼细胞贫血)的发生率高于叶酸补充人群[104]。一项随机对照试验结果显示,哺乳期补充叶酸可提高红细胞叶酸和血红蛋白水平,并防止Hcy水平升高[105]。WHO也建议应补充叶酸至产后3个月[106]。
推荐意见:①尽管现有的循证医学证据尚不足以证明补充叶酸可以降低心血管事件的发生风险,但叶酸水平降低导致的Hcy水平升高仍是心血管疾病的危险因素。目前不推荐使用叶酸来预防心血管疾病,但对于合并高Hcy血症的心血管高危人群和高血压患者推荐补充叶酸,以降低Hcy水平(Ⅱa类推荐,A 级证据)。②对于伴有高血压的高Hcy血症患者,为降低首次脑卒中发生风险,可以采用叶酸单药或包含叶酸的固定复方制剂(Ⅰ类推荐,A级证据)。③每日服用0.8 mg叶酸或联合服用维生素B12可以达到最佳的降低Hcy水平的效果(Ⅱa类推荐,A级证据)。
叶酸缺乏导致Hcy水平升高被认为是动脉粥样硬化和心血管疾病的独立危险因素。Hcy水平升高可导致冠状动脉和降主动脉钙化加重[108,109,110]。流行病学研究显示,当Hcy水平≥16 μmol·L-1时,心血管疾病发生风险明显增加,降低25%的Hcy水平,可以降低11%的冠心病发生风险和19%的脑卒中发生风险[111]。关于Hcy与心血管疾病发生的机制,可能与Hcy直接或间接导致血管内皮细胞损伤、促进血管平滑肌细胞增殖、影响低密度脂蛋白氧化、增强血小板功能和促进血栓形成等有关[112,113,114]。因此,理论上,补充叶酸使Hcy水平下降可以预防和降低心血管事件的发生风险[112,115-117]。
从循证医学角度看,补充叶酸能否带来心血管获益目前并没有获得一致结果,这些研究来源于前瞻性的病例分析、随机安慰剂对照试验和荟萃分析。一项通过食物问卷调查随访14年的一级预防研究发现:食物补充叶酸、维生素B6和维生素B12,与男性心力衰竭的死亡率和女性脑卒中、冠心病和心血管疾病总死亡率均呈负相关[118]。另一项纳入14 项研究的荟萃分析显示:食物摄入叶酸或血中叶酸水平与冠心病程度呈负相关,补充叶酸可使冠心病相对风险降低12%[119]。而多数二级预防研究如VISP 研究[120]、HOPE2研究[121]、NORVIT研究[122]及其他研究等[123]均发现,冠心病、急性心肌梗死患者补充叶酸,在降低Hcy水平的同时,并未带来更多的心血管获益。但一项荟萃分析发现,终末期肾衰竭或严重肾脏疾病患者通过补充叶酸使血Hcy水平降低,其主要心血管事件减少15%,分析显示:补充叶酸时间越长、Hcy水平降低越明显和居民食物中无叶酸强化或仅部分叶酸强化地区,心血管获益越大[124]。另一些荟萃分析显示,与对照组相比,既往有心脑血管疾病或肾脏疾病患者补充叶酸或维生素B族后,其心血管事件和全因死亡率之间差异并无统计学意义,但脑卒中的发生风险降低10%[125,126]。
推荐意见:①高Hcy血症是脑卒中明确的危险因素(A 级证据)。对于单纯高Hcy血症患者,为降低首次脑卒中发生风险,可以考虑每日补充叶酸0.8 mg,也可叶酸联合维生素B6、维生素B12治疗(Ⅱa类推荐,B级证据)。②对于近期发生缺血性脑卒中或短暂性脑缺血发作且Hcy水平轻至中度升高的患者,可以考虑使用叶酸、维生素B6及维生素B12降低脑卒中复发风险(Ⅱb类推荐,B级证据)。
叶酸可能部分通过降低Hcy水平影响脑卒中的发病。一项包含了9项前瞻性研究共13 284例受试者的荟萃分析显示,与较低Hcy水平组相比,高Hcy水平组患者缺血性脑卒中的累积相对风险为1.69[130],其Hcy水平降低25%,脑卒中风险降低19%[111,131]。Framingham后代队列研究发现,将Hcy等4项生物学标志物纳入Framingham脑卒中风险量表评分,可以提高其预测能力[132]。
补充叶酸等维生素可以降低Hcy水平,但能否降低脑卒中风险,各项研究结果并不一致。NORVIT 研究入组3749例急性心肌梗死患者,平均随访4个月,接受叶酸和维生素B12治疗后脑卒中风险并未下降[122]。SEARCH研究入组12 064例心肌梗死患者,随访6.7年,与安慰剂对照组相比,叶酸联合维生素B 治疗组患者的脑卒中发生率也无明显变化[123]。
HOPE2研究纳入了5522例年龄≥55岁既往有心血管疾病或糖尿病病史患者,随访5年,与安慰剂对照组相比,叶酸、维生素B6和维生素B12治疗组患者主要终点事件(心血管源性死亡、心肌梗死和脑卒中的复合终点)无明显减少,但治疗组患者脑卒中发生率(4.0%)较安慰剂对照组(5.3%) 降低25%,差异有统计学意义[121]。无论患者既往是否有脑卒中或短暂性脑缺血发作病史,联合应用维生素B族均可降低脑卒中发生风险[133]。
我国高血压患者Hcy水平较高,研究显示高血压伴高Hcy者发生脑卒中的比例明显高于高血压无高Hcy者,降压的同时补充叶酸有利于预防脑卒中。中国脑卒中一级预防研究(the China stroke primary prevention trial,CSPPT)纳入20 702例无脑卒中或心肌梗死病史的高血压患者,入选患者被随机分为依那普利联合叶酸治疗组(单片固定复方制剂)和单纯依那普利治疗组,随访4.5年,前者首次脑卒中发生率明显低于后者(2.7%:3.4%,HR=0.79,95%
叶酸剂量不同或是否联用其他维生素B族对脑卒中事件的影响存在差异。荟萃分析显示,每日服用≤ 0.8 mg叶酸的患者脑卒中发生率显著降低(
VITATOPS研究入组了8164例7个月内发生脑卒中或短暂性脑缺血发作的患者,随机分为维生素B族治疗组和安慰剂治疗组,平均随访3.4年。维生素B族治疗组和安慰剂治疗组主要终点事件(脑卒中、心肌梗死或血管死亡的复合事件)发生率分别为15%和17%(
综上,针对增加叶酸等维生素B族降低Hcy水平能否降低脑卒中发生风险,研究结果并不一致。主要影响因素包括:地区食物叶酸强化状态、治疗持续时间和Hcy水平下降程度等。降低Hcy水平能否减少脑卒中复发,目前仍缺乏足够证据。未来还需要深入研究Hcy引起动脉粥样硬化的作用和机制,进一步开展设计良好的大样本随机对照试验非常必要。
推荐意见:①认知障碍患者无叶酸缺乏证据时不提倡长期持续服用叶酸(Ⅲ类推荐,A级证据)。②认知障碍患者应常规检测叶酸和维生素B12的水平,合并叶酸缺乏者,可予以补充叶酸0.8 mg·d-1(Ⅱa类推荐,C级证据)。
补充叶酸可有效降低血浆Hcy水平。Hcy不仅是心脑血管疾病的危险因素,还是阿尔茨海默病(Alzheimer's disease,AD)和血管性痴呆的独立危险因素[140,141,142,143,144]。其中代表性研究是SESHADRI等[140]对平均年龄为76岁的1092例无痴呆患者(667例女性,425例男性)进行的一项前瞻性研究,平均随访8年,调整年龄、性别、载脂蛋白E基因型和血管危险因素后发现,血浆Hcy水平>14 μmol·L-1时,AD发生风险增加1倍。近年发表的荟萃分析纳入了多项前瞻性队列研究,也验证了高Hcy水平与痴呆和AD 的相关性[145,146]。推测其机制除与血管因素所致的神经元毒性作用相关外,还与tau蛋白活化异常聚集、抑制甲基化反应等相关[143]。其中一些横断面研究和前瞻性队列研究支持叶酸缺乏与认知功能降低相关,低水平叶酸与AD发生有关[140-141,143,147-148]。
DURGA等[149]在荷兰进行的一项前瞻性队列研究共纳入818例50~70岁的受试者,进行为期3年的随访,每日服用叶酸0.8 mg的受试者血浆Hcy水平降低了26%。虽然认知功能随着年龄增长均有下降趋势,但服用叶酸组受试者在记忆、信息处理速度和感觉运动速度方面均明显优于安慰剂组。然而,还有一些临床研究发现,补充叶酸即使降低了Hcy水平,也未能影响认知功能。目前尚没有足够证据表明补充叶酸能改善认知障碍[150,151]。对心血管疾病高危患者和轻、中度AD患者联合补充叶酸和维生素B12的随访观察揭示:与对照组相比,补充叶酸并未明显提高患者的平均认知功能[152,153],但在摄入维生素B族低的女性亚组中观察到认知功能下降延缓[152]。2年的随访研究发现,每日联合补充叶酸0.4 mg和维生素B12 0.1 mg,能够在一定程度上改善抑郁症成人患者的认知功能评分,尤其是记忆功能的改善更为明显[154]。多数研究者均认为单独补充叶酸或联合补充维生素B12 和维生素B6对于认知功能正常或有认知功能障碍的个体均无改善作用[155,156,157]。一项囊括了11项随机对照试验、超过20 000例老年人群的荟萃分析表明:联合补充叶酸、维生素B12和维生素B6能明显降低Hcy 水平,但对老年人总体认知功能和特定认知分区并无影响[158]。
综上,补充叶酸能有效降低Hcy水平,高Hcy 血症是痴呆的独立危险因素。但目前的循证医学证据尚不能证明补充叶酸可以明显改善认知功能,未来开展研究深入探索叶酸和Hcy在认知障碍中的作用和机制十分必要。
6.4.1 叶酸与ASD 推荐意见:叶酸缺乏可能与ASD相关,计划妊娠的育龄妇女常规补充叶酸0.8 mg·d-1能降低子代ASD的患病风险(Ⅰ类推荐,A级证据),但ASD患儿通过服用叶酸改善ASD症状的循证医学证据不足(Ⅲ类推荐,C级证据)。
ASD的病因和发病机制尚不清楚,目前认为是基因和环境共同作用的结果。孕前和孕期补充叶酸可降低出生儿童罹患ASD的风险。研究认为ASD患儿同样存在不同程度的叶酸代谢异常:一方面,很多ASD患儿有挑食、偏食、异食癖等不良饮食行为,且多合并胃肠道疾病,影响叶酸的摄入和吸收;另一方面,在一些关于ASD患儿的病例对照研究中发现了叶酸相关代谢水平异常与叶酸通路相关的基因突变有关。有研究应用7个叶酸相关代谢指标联合诊断ASD的灵敏度和特异度均在95%以上[159],这些异常表达的叶酸代谢产物作为诊断和预测ASD的生物标志物有潜在的临床应用价值。部分脑叶酸缺乏症的儿童[即血液中的5-甲基四氢叶酸(5-methyltetrahydrofolate,5-MTHF)水平正常,而脑脊液中5-MTHF水平很低的儿童]同时患有ASD。α型叶酸受体是叶酸转运至大脑的主要转运体,在部分ASD患儿中发现了α型叶酸受体自身抗体(folate receptor-α autoantibody,FRAA)[160],导致脑脊液中5-MTHF水平降低。通过大剂量亚叶酸治疗12周,ASD患儿语言交流能力明显改善,尤其是FRAA阳性患儿,对亚叶酸治疗的反应性更好[161]。虽然仍有类似研究发现补充叶酸可改善ASD症状[162],但目前尚缺乏大规模临床研究证据支持叶酸在ASD治疗中的作用。
综上,部分ASD患儿存在叶酸代谢异常,这些患儿补充叶酸可能对ASD有益,但尚需进一步研究叶酸代谢基因和叶酸相关抗体在ASD中的作用及机制,并针对ASD患儿叶酸缺乏的不同亚型进行随机对照试验以明确治疗效果。
6.4.2 叶酸与抑郁症 推荐意见:抑郁症患者在应用抗抑郁药尤其是5-羟色胺再摄取抑制剂的基础上,合理补充叶酸( 建议0.5~2.5 mg·d-1)可提高治疗的反应性(Ⅱa类推荐,B级证据)。
最近的一些研究发现叶酸缺乏与抑郁症和对抗抑郁药的低反应性相关,其机制可能涉及多个方面。首先,叶酸在体内转化为甲基活性成分方能通过血-脑脊液屏障,在脑内通过调控多巴胺和5-羟色胺的重要辅因子,间接影响这些神经递质的水平,从而参与抑郁症的发病[163,164]。其次,高Hcy血症与抑郁症相关,而叶酸能降解Hcy,从而与抑郁症相关。再次,在一些存在与抑郁症相关的继发因素(如不健康饮食、酒精或药物依赖等)人群中也能观察到低叶酸水平,表明其与抑郁症有相关性[165]。
美国进行的2项数千人参与的观察性研究发现,抑郁症患者的叶酸水平明显低于无抑郁症者[165],高血清叶酸水平与低抑郁症发生率相关[163]。但加拿大一项共纳入1368例年龄67~84岁健康人群的研究中并未发现叶酸摄取量与抑郁症存在明显的相关性[164]。
此外,一些临床研究表明叶酸单药和联合应用抗抑郁药对抑郁症有治疗作用。英国一项纳入127 例患者的队列研究中,抑郁症患者应用氟西汀联合叶酸治疗对比氟西汀联合安慰剂治疗10周,结果发现联合叶酸治疗的女性患者汉密尔顿评分明显降低,在服用叶酸的女性患者中,有93.9%对氟西汀反应良好(评分降低50%),对照组仅为61.1%[166]。而英国一项纳入475例中、重度抑郁症患者的随机对照试验发现,与联合安慰剂组相比,试验组患者采用抗抑郁药联合5 mg叶酸治疗12周,并未明显改善抑郁症状[167]。还有一些小样本的随机双盲对照试验提出补充叶酸能明显改善5-羟色胺再摄取抑制剂的抗抑郁效果[168]。一项荟萃分析对4项叶酸临床试验(2项试验叶酸剂量<5 mg·d-1,另2项试验叶酸剂量为5 mg·d-1)进行系统性分析,得出结论:每日补充<5 mg的叶酸可能是5-羟色胺再摄取抑制剂治疗的有益补充,但亦强调这只是基于低证据级别的推荐[169]。2015年英国精神药理协会修订的抑郁症治疗指南[170]和加拿大抑郁焦虑治疗网络[171]均推荐了叶酸可能作为5-羟色胺再摄取抑制剂治疗抑郁症的补充。
综上,叶酸缺乏与抑郁症相关,低叶酸水平与抗抑郁药低反应性相关。叶酸单药和联合抗抑郁药对抑郁症的治疗效果虽然尚存争议,但目前证据支持在抗抑郁药的基础上联合叶酸能提高抑郁症患者治疗的反应性,其机制尚待进一步研究。
推荐意见:①不建议将叶酸常规用于延缓慢性肾脏病(chronic kidney disease,CKD)进展;建议可考虑给叶酸偏低或缺乏的伴高血压的CKD患者使用叶酸单药(0.8 mg·d-1)或包含叶酸的固定复方制剂,这可能对延缓CKD进展有益(Ⅱa类推荐,B级证据)。②建议可考虑将叶酸常规用于伴高Hcy水平的CKD患者脑血管病的预防(Ⅱa类推荐,A级证据)。③CKD饮食配方可满足日常叶酸摄入量需求。叶酸补充可作为重组人红细胞生成素(reco- mbinant human erythropoietin,rhEPO)治疗肾性贫血的辅助手段;对于有叶酸缺乏证据的患者,补充叶酸有助于提高血红蛋白对rhEPO的反应性(Ⅱa 类推荐,B级证据)。
补充叶酸可降低Hcy水平,但对于其是否可以延缓CKD进展,目前的研究结论不一致。HOST研究显示补充中高剂量叶酸不能延缓CKD进展[176],而DIVINe研究则得出服用叶酸患者CKD进展更快的结论[177]。CSPPT的肾脏亚组研究显示,与单纯降压治疗相比,同时补充叶酸(0.8 mg·d-1)可降低CKD进展风险[174];在治疗前已有CKD的患者降低更明显。同时可显著降低糖尿病患者新发蛋白尿风险[178]。导致上述研究结论差异的可能原因是不同研究的叶酸基线水平不同,HOST和DIVINe研究人群均已食用强化叶酸食物,对于未进行强化食物补充叶酸的基线水平低的人群来说,补充叶酸可能有益于延缓CKD进展。
目前对补充叶酸是否可降低CKD患者的脑血管疾病风险仍存争议。虽然一些研究表明补充叶酸并不能降低CKD患者脑血管疾病的发病率和死亡率[176-177,179],但也有荟萃分析结果表明补充叶酸可降低CKD患者脑血管疾病发生风险,尤其是当Hcy 水平较高时更为明显[124,180]。
补充叶酸可作为rhEPO治疗肾性贫血的辅助手段。当有红细胞体积增大、血清叶酸水平降低等叶酸缺乏证据且血红蛋白对rhEPO反应不佳时,补充叶酸有助于纠正肾性贫血并可能有助于减少rhEPO 的使用剂量[181]。
CKD患者和血液透析或腹膜透析患者叶酸缺乏的主要原因是饮食摄入叶酸不足。如果叶酸自饮食的摄入不足,在准确评估叶酸状态后,可通过药物补充[182]。
推荐意见:服用小剂量甲氨蝶呤的患者应补充叶酸每周5~10 mg(Ⅰ类推荐,A级证据)。
6.6.1 甲氨蝶呤治疗与叶酸补充 甲氨蝶呤广泛用于风湿免疫性疾病的治疗,是类风湿关节炎(rheuma- toid arthritis,RA)治疗首选[183]。但即使采用小剂量(≤每周30 mg)甲氨蝶呤治疗,不良反应仍然常见[184]。在Cochrane系统综述中,补充叶酸或甲酰四氢叶酸使肝损伤(转氨酶水平升高)发生风险降低16.8%和15.2%,也显著降低甲氨蝶呤停药发生率(分别降低14.2%和16.2%)。补充叶酸或甲酰四氢叶酸也能减少胃肠道不良反应(恶心、呕吐、腹痛)和口腔溃疡的发生,但均未达统计学意义。而补充叶酸或甲酰四氢叶酸对RA疾病活动度无显著影响[185]。一项临床试验显示,每周补充10或30 mg叶酸,甲氨蝶呤不良反应发生率比较差异无统计学意义,提示更大剂量的叶酸补充不能使患者进一步获益[186]。服用甲氨蝶呤数小时后服用甲酰四氢叶酸有可能降低甲氨蝶呤疗效[187]。有学者建议将甲酰四氢叶酸作为甲氨蝶呤过量中毒解救用药,所有服用甲氨蝶呤的患者均补充叶酸(每周5~10 mg)可减少不良反应的发生[188]。
6.6.2 RA患者高Hcy血症与叶酸补充 RA患者出现心血管事件相关死亡的风险是普通人群的2倍,高Hcy水平是RA患者心脑血管死亡增加的危险因素之一[189]。高Hcy水平在RA患者中常见,与脑血管疾病的发生相关[190]。一项前瞻性队列研究提示,高Hcy水平是所有致死/非致死动脉血栓事件(心肌梗死、缺血性心脏病、脑卒中、短暂性脑缺血发作、深静脉血栓/肺栓塞)的危险因素(
综上,每周服用1次小剂量甲氨蝶呤的患者补充叶酸可减少不良反应的发生,推荐剂量为每周5~10 mg。应重视RA患者高Hcy血症的发生,但补充叶酸对RA患者心血管疾病的预防作用尚待随机对照临床试验进行研究。
人体叶酸缺乏可能带来不同的健康风险,中国人群对补充叶酸仍存在一些认识上的误区和不足。虽然国内外对于叶酸的研究非常多,但临床上对于叶酸缺乏的判断标准和治疗仍缺乏统一规范。《共识》基于现有研究证据,针对临床叶酸缺乏的筛查与预防及补充叶酸的适应人群、时机、剂量与疗程、联合用药等进行了统一和规范,通过多学科专家的研讨和大量循证医学证据的筛选,总结补充叶酸的推荐建议和证据等级,同时明确叶酸与其他药物的相互作用及相应的处理措施。未来随着研究的不断深入和更多证据的产生,《共识》将定期更新或转换为临床指南。
指导单位:中国医药教育协会
学术指导专家
孙宁玲 北京大学人民医院心脏中心
王玉平 首都医科大学宣武医院神经内科
联合组长(按姓氏拼音排序)
陈敦金 广州医科大学附属第三医院产科
陈源源 北京大学人民医院心脏中心
李光辉 首都医科大学附属北京妇产医院围产医学部
宋海庆 首都医科大学宣武医院神经内科
赵志刚 首都医科大学附属北京天坛医院药学部
编写专家组(按姓氏拼音排序)
贺 芳 广州医科大学附属第三医院产科
蒋真斌 北京大学人民医院肾内科
刘 蔚 北京医院心血管内科
秦海强 首都医科大学附属北京天坛医院神经病学中心
王乔宇 首都医科大学附属北京天坛医院药学部
王文志 北京市神经外科研究所
王志坚 南方医科大学南方医院妇产科
武明芬 首都医科大学附属北京天坛医院药学部
岳 伟 天津市环湖医院神经内科
郑 薇 首都医科大学附属北京妇产医院围产医学部
周 炜 首都医科大学附属北京天坛医院风湿免疫科
朱文丽 北京大学公共卫生学院
左 力 北京大学人民医院肾内科
咨询专家组(按姓氏拼音排序)
曹引丽 西北妇女儿童医院产科
陈 孝 中山大学附属第一医院药学部
陈会生 北部战区总医院神经内科
楚 兰 贵州医科大学附属医院神经内科
杜 光 华中科技大学同济咸宁医院
姜一农 大连医科大学附属第一医院高血压与心力衰竭中心
李 丽 吉林省人民医院神经内科
李国忠 哈尔滨医科大学附属第一医院神经内科
李南方 新疆维吾尔自治区人民医院高血压中心
李智文 北京大学生育健康研究所
刘皋林 上海市第一人民医院临床药学科
刘凯波 首都医科大学附属北京妇产医院围产保健科
柳 鹏 北京大学人民医院临床营养科
缪丽燕 苏州大学附属第一医院药学部
童荣生 四川省人民医院药学部
王翠兰 山东大学齐鲁医院神经内科
武新安 兰州大学第一医院药剂科
许予明 郑州大学第一附属医院神经内科
荫士安 中国疾病预防控制中心营养与健康所
于 红 东南大学附属中大医院妇产科
袁 洪 中南大学湘雅三医院临床药理中心
张 毅 甘肃省人民医院神经内科
张新军 四川大学华西医院老年医学中心
| [1] |
Hydroxyethyl methacrylate-derivative pullulan (pullulan-HEMA) was synthesized by activation of HEMA followed by catalyzed reaction for adjusting the degree of substitution (DS) of copolymer. Pullulan-HEMA was photocrosslinked using new three-components photoinitiating system composed of carboxylated camphorquinone-folic acid-iodonium salt under visible light. Folic acid was employed as new coinitiator for improving the entire hydrogel properties and avoiding harms of traditional used tertiary amine coinitiators. Pullulan-HEMA hydrogels were characterized by swelling, crosslinking density, and degree of conversion. It was observed that the increase of crosslinking density, Tg, degree of conversion are owing to increasing the DS of copolymer. However, water uptake of hydrogel decreased with increasing the DS value and folic acid concentrations, owing to increasing the crosslinking densities of hydrogels. Also, increasing DS of copolymer and folic acid improved sharply hydrogel surface morphology and prolonged the required time for enzymatic degradation. Notably, the alteration in DS of copolymer converted the in vitro release profile of dexamethasone from rapid and big burst release into sustained and low release behavior. Meanwhile, we could obtain progressive and tunable storage modulus ranged ca. 2.0-10KPa when DS of copolymer was altered from 0.025 to 0.086, showing that pullulan-HEMA hydrogels are promising biomaterial candidate for biomedical applications.
[本文引用:1]
|
| [2] |
|
| [3] |
DOI:10.1172/JCI104391
URL
[本文引用:1]
|
| [4] |
BACKGROUND: A quantitative understanding of human folate metabolism is needed. OBJECTIVE: The objective was to quantify and interpret human folate metabolism as it might occur in vivo. DESIGN: Adults (n = 13) received 0.5 nmol [(14)C]pteroylmonoglutamate (100 nCi radioactivity) plus 79.5 nmol pteroylmonoglutamate in water orally. (14)C was measured in plasma, erythrocytes, urine, and feces for >/=40 d. Kinetic modeling was used to analyze and interpret the data. RESULTS: According to the data, the population was healthy and had a mean dietary folate intake of 1046 nmol/d, and the apparent dose absorption of (14)C was 79%. The model predictions showed that only 0.25% of plasma folate was destined for marrow, mean bile folate flux was 5351 nmol/d, and the digestibility of the mix (1046 + 5351 nmol/d) was 92%. About 33% of visceral pteroylmonoglutamate was converted to the polyglutamate form, most of the body folate was visceral (>99%), most of the visceral folate was pteroylpolyglutamate (>98%), total body folate was 225 micromol, and pteroylpolyglutamate synthesis, recycling, and catabolism were 1985, 1429, and 556 nmol/d, respectively. Mean residence times were 0.525 d as visceral pteroylmonoglutamate, 119 d as visceral pteroylpolyglutamate, 0.0086 d as plasma folate, and 0.1 d as gastrointestinal folate. CONCLUSIONS: Across subjects, folate absorption, bile folate flux, and body folate stores were larger than prior estimates. Marrow folate uptake and pteroylpolyglutamate synthesis, recycling, and catabolism are saturable processes. Visceral pteroylpolyglutamate was an immediate precursor of plasma p-aminobenzoylglutamate. The model is a working hypothesis with derived features that are explicitly model-dependent. It successfully quantitated folate metabolism, encouraging further rigorous testing.
[本文引用:1]
|
| [5] |
BACKGROUND: In a new preparation of prenatal multivitamins, PregVit, two tablets a day (a.m. and p.m.) are given. Folic acid is separated from iron and zinc and is given in the p.m. tablet to overcome problems due to folic acid interactions with iron or zinc, and frequent presence of nausea and vomiting of pregnancy in the morning. The circadian variation of folate in humans has not been investigated. This is the first study attempting to determine whether circadian variation of folate pharmacokinetics exists in humans. OBJECTIVES: To determine whether circadian rhythm of folate pharmacokinetics exists in humans. METHODS: In a crossover design, six healthy, non-pregnant women were randomized to receive 1 tablet of PregVit p.m., containing 1.1 mg of folic acid, in the morning or evening. Serum folate levels were measured over 10 hours. The area under the concentration-time curve (AUC) was used to compare the extent of absorption between the two time periods. RESULTS: The mean AUC values for serum folate after administration of PregVit p.m. were 334.5+/-119.6 nM*h and 283.1+/-64.3 nM*h for morning and evening, respectively (P = 0.17). The morning and evening peak serum folate concentrations were also similar (135.3+/-41.7 nM and 130.3+/-14.2 nM, respectively) (P = 0.75). Similarly, the time to peak for the morning arm (1 0.5 hour) was similar to evening administration (1+/-0.4 hour). CONCLUSIONS: There is no evidence of circadian variation in folate pharmacokinetics. Thus, the introduction of folate in PregVit p.m. will not affect its effectiveness as compared to its routine administration in the morning.
[本文引用:1]
|
| [6] |
Following an introduction of the importance of folates and the rationale for seeking to estimate fractional folate absorption from foods (especially for countries not having a mandatory folic acid fortification policy), scientific papers covering the mechanisms of folate absorption and initial biotransformation are discussed. There appears (post-1983) to be a consensus that physiological doses of folic acid undergo biotransformation in the absorptive cells of the upper small intestine to 5-methyltetrahydrofolic acid (as happens for all naturally-occurring reduced 1-carbon-substituted folates). This 'validates' short-term experimental protocols assessing 'relative' folate absorption in human subjects that use folic acid as the 'reference' dose. The underlying scientific premise on which this consensus is based is challenged on three grounds: (i) the apparent absence of a 5-methyltetrahydrofolic acid response in the human hepatic portal vein following absorption of folic acid, (ii) the low dihydrofolate reductase activity peculiar to man and (iii) the implications derived from recent stable-isotope studies of folate absorption. It is concluded that the historically accepted case for folic acid being a suitable 'reference folate' for studies of the 'relative absorption' of reduced folates in human subjects is invalid. It is hypothesised that the liver, and not the absorptive cells of the upper small intestine, is the initial site of folic acid metabolism in man and that this may have important implications for its use as a supplement or fortificant since human liver's low capacity for reduction may eventually give rise to saturation, resulting in significant (and potentially deleterious) unmetabolised folic acid entering the systemic circulation.
[本文引用:1]
|
| [7] |
Data on the effect of combined genetic polymorphisms, involved in folate metabolism, on the concentration of serum folate after folic acid supplementation are scarce. Therefore, we investigated the impact of seven gene polymorphisms on the concentration of serum folate and p-tHcy in healthy subjects after short-term folic acid supplementation. In a randomized, double blind, crossover study, apparently healthy subjects were given either 0.8 mg folic acid per day (n = 46) or placebo (n = 45) for 14 days. The washout period was 14 days. Fasting blood samples were collected on day 1, 15, 30 and 45. Data on subjects on folic acid supplementation (n = 91) and on placebo (n = 45) were used for the statistical analysis. The concentration of serum folate increased higher in subjects with higher age (53.5 +/- 7.0 years) than in subjects with lower age (24.3 +/- 3.2 years) after folic acid supplementation (p = 0.006). The baseline concentration of serum folate in subjects with polymorphism combination, reduced folate carrier protein, RFC1-80 GA and methylenetetrahydrofolate reductase, MTHFR677 CT+TT, was lower than RFC1-80 AA and MTHFR677 CT+TT (p = 0.002). After folic acid supplementation, a higher increase in the concentration of serum folate was detected in subjects with polymorphism combination RFC1-80 GA and MTHFR677 CC than RFC1-80 GG and MTHFR CT+TT combination (p < 0.0001). The baseline concentration of plasma total homocysteine (p-tHcy) was altered by combined polymorphisms in genes associated with folate metabolism. After folic acid supplementation, in subjects with combined polymorphisms in methylenetetrahydrofolate dehydrogenase, MTHFD1-1958 and MTHFR-677 genes, the concentration of p-tHcy was changed (p = 0.002). The combination of RFC1-80 and MTHFR-677 polymorphisms had a profound affect on the concentration of serum folate in healthy subjects before and after folic acid supplementation.
[本文引用:1]
|
| [8] |
A pharmacokinetic study of folic acid and its metabolites was conducted to provide a basis to consider folic acid as a therapeutic alternative to leucovorin. Leucovorin has been used in various folate antagonist rescue regimens and to modulate fluorouracil activity in the treatment of solid tumors. Although leucovorin is typically administered intravenously in fluorouracil modulation therapy, limited oral administration trials have yielded equivalent responses. Because metabolites rather than leucovorin are the predominant circulating species after oral administration, these clinical results indicate that metabolites themselves can be modulating agents. Folic acid could be an attractive alternative to leucovorin provided it effectively elevates the same plasma metabolites. Hence, folic acid at doses of 25 and 125 mg/m2 was administered orally and intravenously to normal volunteers. Plasma folic acid and its reduced folate metabolites were monitored over a 24-hour period by use of a previously developed radioenzymatic method. The metabolites that accumulated--5-methyltetrahydrofolate, 5,10-methylenetetrahydrofolate, tetrahydrofolate, and 10-formyltetrahydrofolate--were the same metabolites that were observed previously after leucovorin administration. Folic acid metabolites accumulated more slowly and persisted longer than leucovorin metabolites, which can be attributed to slower metabolism of the fully oxidized vitamin. Based on these results, it is concluded that folic acid could be an attractive therapeutic alternative to leucovorin for fluorouracil modulation.
[本文引用:1]
|
| [9] |
There is a large body of evidence to suggest that improving periconceptional folate status reduces the risk of neonatal neural tube defects. Thus increased folate intake is now recommended before and during the early stages of pregnancy, through folic acid supplements or fortified foods. Furthermore, there is growing evidence that folic acid may have a role in the prevention of other diseases, including dementia and certain types of cancer. Folic acid is a synthetic form of the vitamin, which is only found in fortified foods, supplements and pharmaceuticals. It lacks coenzyme activity and must be reduced to the metabolically active tetrahydrofolate form within the cell. L-5-methyl-tetrahydrofolate (L-5-methyl-THF) is the predominant form of dietary folate and the only species normally found in the circulation, and hence it is the folate that is normally transported into peripheral tissues to be used for cellular metabolism. L-5-methyl-THF is also available commercially as a crystalline form of the calcium salt (Metafolin(R)), which has the stability required for use as a supplement. Studies comparing L-5-methyl-THF and folic acid have found that the two compounds have comparable physiological activity, bioavailability and absorption at equimolar doses. Bioavailability studies have provided strong evidence that L-5-methyl-THF is at least as effective as folic acid in improving folate status, as measured by blood concentrations of folate and by functional indicators of folate status, such as plasma homocysteine. Intake of L-5-methyl-THF may have advantages over intake of folic acid. First, the potential for masking the haematological symptoms of vitamin B(12) deficiency may be reduced with L-5-methyl-THF. Second, L-5-methyl-THF may be associated with a reduced interaction with drugs that inhibit dihydrofolate reductase.
[本文引用:1]
|
| [10] |
Anticonvulsants have been shown to cause folacin deficiency in chronically treated epileptic patients. However, a mechanism for this depletion has not been established. In the present study, the effects of chronic primidone treatment on folates in the rat were investigated. Using a continuously protective relatively nontoxic regimen of oral administration, it was found that primidone (100 mg/kg, twice per day) caused a decrease of pteroylpentaglutamates in the liver to less than half the control value within 1 wk. Total liver folacin concentration decreased by 30% in the first week followed by a slow gradual further decline with continuing treatment. Plasma folacin exhibited essentially the same pattern but no effect was observed on brain folacin concentration. Primidone was not detectable in plasma 12 h after gavage but phenobarbital was detectable. These data are consistent with the hypothesis that the anticonvulsant primidone (and/or phenobarbital) cause folate depletion via interaction with folate metabolism.
[本文引用:0]
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
OBJECTIVE: To assess the efficacy of folic acid and folinic acid in reducing the mucosal and gastrointestinal (GI) side effects of low dose methotrexate (MTX) in patients with rheumatoid arthritis (RA). METHODS: A systematic review was carried out using the methods recommended by the Cochrane Collaboration. We used MEDLINE and performed hand searches that included bibliographic references, Current Contents, abstracts of rheumatology meetings, and 4 rheumatology journals to select double blind randomized controlled trials (RCT) in which adult patients with RA were treated with low doses of MTX (< 20 mg/week), concurrently with folic or folinic acid. The quality of the RCT was assessed. The overall treatment effect across trials (reduction in toxicity) was estimated using a fixed effects model. Disease activity was evaluated using standardized mean differences to ensure comparability across outcome measures. Sensitivity analyses were conducted evaluating different doses and the quality of the trials. Costs per month in different countries were compared. RESULTS: Of 11 trials retrieved, 7 met inclusion criteria. The total sample included 307 patients, of which 147 were treated with folate supplementation, 67 patients with folic, and 80 with folinic acid. A 79% reduction in mucosal and GI side effects was observed for folic acid [OR = 0.21 (95% CI 0.10 to 0.44)]. For folinic acid, a clinically but nonstatistically significant reduction of 42% was found [OR = 0.58 (95% CI 0.29 to 1.16)]. No major differences were observed between low and high doses of folic or folinic acid. Hematologic side effects could not be analyzed, since details by patients of each event were not provided. No consistent differences in disease activity variables were observed when comparing placebo and folic acid or folinic acid at low doses; patients receiving high dose folinic acid had increased tender and swollen joint counts. Substantial differences in costs across countries were found; folinic acid was more expensive. CONCLUSION: Our results support the protective effect of folate supplementation in reducing MTX side effects related to the oral and GI systems.
[本文引用:0]
|
| [16] |
|
| [17] |
AbstractFolic acid (FA) is a vitamin that acts as a coenzyme in the biosynthesis of purine and pyrimidine precursors of nucleic acids, which are critically important during pregnancy. Our group has previously shown that both reduced folate carrier (RFC1) and folate receptor α (FRα) seem to be involved in the uptake of [3H]folic acid ([3H]FA) by a human trophoblast cell line (BeWo) and by human primary cultured cytotrophoblasts. Our aim was to study the interaction between FA and some nutrients/bioactive substances. For this, we tested the acute and chronic effects of some dietary compounds on [3H]FA apical uptake and on the expression of both RFC1 and FRα mRNA in BeWo cells. Our results show that [3H]FA uptake was significantly reduced by acute exposure to epicatechin, isoxanthohumol (1–400 μM) or theophylline (0.1–100 μM); isoxanthohumol seemed to act as a competitive inhibitor, whereas epicatechin and theophylline caused an increase in both Km and Vmax. On the other hand, [3H]FA uptake was significantly increased by chronic exposure to xanthohumol, quercetin or isoxanthohumol (0.1–10 μM), and this increase does not seem to result from changes in the level of RFC1 or FRα gene expression. Moreover, [3H]FA uptake was significantly reduced by chronic exposure to ethanol (0.01%). This reduction seems to be, at least in part, due to a reduction in FRα expression. These results are compatible with an association between a deficient FA supply to the placenta/fetus and ethanol toxicity in pregnancy. |
| [18] |
Triamterene, a diuretic agent, has been reported to cause megaloblastic anemia in some patients. Because this drug is a pteridine derivative, we investigated its effect on folic acid absorption in the rat jejunum. In an in vivo intestinal loop method, triamterene inhibited the intestinal absorption of folic acid in a dose-dependent fashion, with 50% inhibition of systemic absorption occurring at a luminal concentration of 0.01 mmol/L of triamterene. Kinetic analysis using the influx chamber method demonstrated that triamterene is a competitive inhibitor of intestinal folate transport, with a Ki of 0.125 mmol/L. Because therapeutic doses can result in luminal concentration of the drug approximating or exceeding the Ki, the interaction between triamterene and folate absorption is potentially of clinical interest.
[本文引用:0]
|
| [19] |
BACKGROUND/AIMS: Folic acid deficiency has been reported to elevate plasma homocysteine levels and result in hyperhomocystinemia, which is an independent risk factor for cardiovascular disease. Sevelamer hydrochloride has the potential to bind with folic acid. To determine this effect of sevelamer hydrochloride on plasma homocysteine levels, change in serum folic acid and plasma homocysteine levels after administration of sevelamer hydrochloride in chronic hemodialysis patients was evaluated. METHODS: Sevelamer hydrochloride was administered to 26 outpatients undergoing hemodialysis for 3 months. Serum and plasma samples were collected just before the dialysis session at baseline and 3 months. RESULTS: Three months after the administration of sevelamer hydrochloride, serum folic acid levels significantly decreased (baseline vs. 3 months; 5.48 +/- 1.81 vs. 4.79 +/- 1.79 ng/ml, p < 0.05), whereas plasma homocysteine levels significantly increased (baseline vs. 3 months; 50.8 +/- 35.9 vs. 67.6 +/- 44.7 nmol/ml, p < 0.01). CONCLUSION: These findings suggest that sevelamer hydrochloride elevates plasma homocysteine levels, possibly by inhibiting the absorption of folic acid. Thus, the effect of sevelamer hydrochloride should be excluded while evaluating the increased plasma levels of homocysteine.
[本文引用:0]
|
| [20] |
The term folate (vitamin B9) refers to a group of water-soluble compounds that are nutritionally essential for the support of optimal human health and development. Folates participate in numerous one-carbon transfer reactions, including the methylation of important biomolecules (lipids, amino acids, DNA). A deficiency of folate leads to pathological outcomes including anemia and impairments in reproductive health and fetal development. Due to the linkage of impaired folate status with an increased prevalence of neural tube defects (NTDs) in babies, several jurisdictions required the fortification of the food supply with folic acid, a synthetic and stable form of folate. Data from the postfortification era have provided strong evidence for the reduction of NTDs due to folic acid fortification. However, concern is now growing with respect to the amount of synthetic folic acid within the human food supply. Excess folic acid intake has been linked to a masking of vitamin B12 deficiency, and concerns regarding the promotion of folate-sensitive cancers, including colorectal cancer. New strategies to ensure the supply of optimal folate to at-risk populations may be needed, including the use of biofortification approaches, in order to address recent concerns.
[本文引用:5]
|
| [21] |
|
| [22] |
|
| [23] |
Folate (vitamin B9) plays a crucial role in fundamental cellular processes, including nucleic acid biosynthesis, methyl group biogenesis and amino acid metabolism. The detection and correction of folate deficiency prevents megaloblastic anaemia and reduces the risk of neural tube defects. Coexisting deficiencies of folate and vitamin B12 are associated with cognitive decline, depression and neuropathy. Folate deficiency and excess has also been implicated in some cancers. Excessive exposure to folic acid, a synthetic compound used in supplements and fortified foods, has also been linked to adverse health effects. Of at least three distinct laboratory markers of folate status, it is the total abundance of folate in serum/plasma that is used by the majority of laboratories. The analysis of folate in red cells is also commonly performed. Since the folate content of red cells is fixed during erythropoiesis, this marker is indicative of folate status over the preceding ~4 months. Poor stability, variation in polyglutamate chain length and unreliable extraction from red cells are factors that make the analysis of folate challenging. The clinical use of measuring specific folate species has also been explored. 5-Methyltetrahydrofolate, the main form of folate found in blood, is essential for the vitamin B12-dependent methionine synthase mediated remethylation of homocysteine to methionine. As such, homocysteine measurement reflects cellular folate and vitamin B12 use. When interpreting homocysteine results, age, sex and pregnancy, specific reference ranges should be applied. The evaluation of folate status using combined markers of abundance and cellular use has been adopted by some laboratories. In the presence of discordance between laboratory results and strong clinical features of deficiency, treatment should not be delayed. High folate status should be followed up with the assessment of vitamin B12 status, a review of previous results and reassessment of folic acid supplementation regime.
[本文引用:1]
|
| [24] |
|
| [25] |
The CDC's National Report on Biochemical Indicators of Diet and Nutrition in the U.S. Population (Nutrition Report) is a serial publication that provides ongoing assessment of the population's nutritional status. The Nutrition Report presents data on blood and urine biomarker concentrations (selected water- and fat-soluble vitamins and nutrients, trace elements, dietary bioactive compounds) from a representative sample of the population participating in the NHANES. The Second Nutrition Report (released in 2012) contains reference information (means and percentiles) for 58 biomarkers measured during all or part of 2003-2006, stratified by age, sex, and race-ethnicity. Where available, we presented cutoff-based prevalence data during 2003-2006 and data on changes in biomarker concentrations or prevalence since 1999. Blood vitamin concentrations were generally higher in older (>/= 60 y) than in younger (20-39 y) adults and lower in Mexican Americans and non-Hispanic blacks than in non-Hispanic whites. Nearly 80% of Americans (aged >/= 6 y) were not at risk of deficiencies in any of the 7 vitamins studied (vitamins A, B-6, B-12, C, D, and E and folate). Deficiency rates varied by age, sex, and race-ethnicity. Approximately 90% of women (aged 12-49 y) were not at risk of iron deficiency, but only 68% were not at risk of deficiencies in iron and all 7 vitamins. Young women (20-39 y) had median urine iodine concentrations bordering on insufficiency. First-time data are presented on plasma concentrations of 24 saturated and mono- and polyunsaturated fatty acids. Tabulation and graphical presentation of NHANES data in the Second Nutrition Report benefits those organizations involved in developing and evaluating nutrition policy.
[本文引用:2]
|
| [26] |
The aim of this new statement is to provide comprehensive and timely evidence-based recommendations on the prevention of ischemic stroke among survivors of ischemic stroke or transient ischemic attack. Evidence-based recommendations are included for the control of risk factors, interventional approaches for atherosclerotic disease, antithrombotic treatments for cardioembolism, and the use of antiplatelet agents for noncardioembolic stroke. Further recommendations are provided for the prevention of recurrent stroke in a variety of other specific circumstances, including arterial dissections; patent foramen ovale; hyperhomocysteinemia; hypercoagulable states; sickle cell disease; cerebral venous sinus thrombosis; stroke among women, particularly with regard to pregnancy and the use of postmenopausal hormones; the use of anticoagulation after cerebral hemorrhage; and special approaches for the implementation of guidelines and their use in high-risk populations.
[本文引用:1]
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
BACKGROUND: It has been reported that neural tube defects (NTD) can be prevented with periconceptional folic acid supplementation. The effects of different doses, forms and schemes of folate supplementation for the prevention of other birth defects and maternal and infant outcomes are unclear. OBJECTIVES: This review aims to examine whether periconceptional folate supplementation reduces the risk of neural tube and other congenital anomalies (including cleft palate) without causing adverse outcomes in mothers or babies. This is an update of a previously published Cochrane review on this topic. SEARCH METHODS: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 August 2015). Additionally, we searched the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (31 August 2015) and contacted relevant organisations to identify ongoing and unpublished studies. SELECTION CRITERIA: We included all randomised or quasi-randomised trials evaluating the effect of periconceptional folate supplementation alone, or in combination with other vitamins and minerals, in women independent of age and parity. DATA COLLECTION AND ANALYSIS: Two review authors independently assessed the eligibility of studies against the inclusion criteria, extracted data from included studies, checked data entry for accuracy and assessed the risk of bias of the included studies. We assessed the quality of the body of evidence using the GRADE approach. MAIN RESULTS: Five trials involving 7391 women (2033 with a history of a pregnancy affected by a NTD and 5358 with no history of NTDs) were included. Four comparisons were made: 1) supplementation with any folate versus no intervention, placebo or other micronutrients without folate (five trials); 2) supplementation with folic acid alone versus no treatment or placebo (one trial); 3) supplementation with folate plus other micronutrients versus other micronutrients without folate (four trials); and 4) supplementation with folate plus other micronutrients versus the same other micronutrients without folate (two trials). The risk of bias of the trials was variable. Only one trial was considered to be at low risk of bias. The remaining studies lacked clarity regarding the randomisation method or whether the allocation to the intervention was concealed. All the participants were blinded to the intervention, though blinding was unclear for outcome assessors in the five trials.The results of the first comparison involving 6708 births with information on NTDs and other infant outcomes, show a protective effect of daily folic acid supplementation (alone or in combination with other vitamins and minerals) in preventing NTDs compared with no interventions/placebo or vitamins and minerals without folic acid (risk ratio (RR) 0.31, 95% confidence interval (CI) 0.17 to 0.58); five studies; 6708 births; high quality evidence). Only one study assessed the incidence of NTDs and showed no evidence of an effect (RR 0.07, 95% CI 0.00 to 1.32; 4862 births) although no events were found in the group that received folic acid. Folic acid had a significant protective effect for reoccurrence (RR 0.34, 95% CI 0.18 to 0.64); four studies; 1846 births). Subgroup analyses suggest that the positive effect of folic acid on NTD incidence and recurrence is not affected by the explored daily folic acid dosage (400 microg (0.4 mg) or higher) or whether folic acid is given alone or with other vitamins and minerals. These results are consistent across all four review comparisons.There is no evidence of any preventive or negative effects on cleft palate (RR 0.73, 95% CI 0.05 to 10.89; three studies; 5612 births; low quality evidence), cleft lip ((RR 0.79, 95% CI 0.14 to 4.36; three studies; 5612 births; low quality evidence), congenital cardiovascular defects (RR 0.57, 95% CI 0.24 to 1.33; three studies; 5612 births; low quality evidence), miscarriages (RR 1.10, 95% CI 0.94 to 1.28; five studies; 7391 pregnancies; moderate quality evidence) or any other birth defects (RR 0.94, 95% CI 0.53 to 1.66; three studies; 5612 births; low quality evidence). There were no included trials assessing the effects of this intervention on neonatal death, maternal blood folate or anaemia at term. AUTHORS' CONCLUSIONS: Folic acid, alone or in combination with vitamins and minerals, prevents NTDs, but does not have a clear effect on other birth defects.
[本文引用:1]
|
| [42] |
OBJECTIVE: To summarize the recommendations on folate intake and folic acid supplementation and fortification in the periconceptional period, aimed at prevention of neural tube defects (NTD), provided by official health organizations in different countries worldwide and WHO. DESIGN: Information on recommendations for folate and folic acid intake in the periconceptional period was gathered from the websites of official national health organizations of several countries worldwide and from the WHO website. SETTING: WHO, selected developed countries and emerging economies, totalling thirty-six countries worldwide (some European, BRICS, G8, Asian Tiger/Asian Dragon and Australia). RESULTS: Recommendations differ between countries, although the majority (69.4 %) recommend a healthy diet plus a folic acid supplement of 400 microg/d from preconception (4-12 weeks) until the end of the first trimester of pregnancy (8-12 weeks). The same recommendation is issued by the WHO. Dosages for women at high risk of NTD are up to 4-5 mg/d (for 41.7 % of studied countries). The recommended intake for folate is in the range of 300-400 microg/d for women of childbearing age and 500-600 microg/d for pregnant women in different countries and WHO. Five countries emphasize the importance of a healthy diet rendering supplementation needless. By contrast, five others advise a healthy diet and supplementation plus mandatory fortification. Only one mentions the importance of ensuring an adequate folate status and refers to checking with a health-care provider on the need for supplements. CONCLUSIONS: Different recommendations regarding folate and folic acid, seeking NTD prevention, are available worldwide; however, most countries and WHO focus on a healthy diet and folic acid supplementation of 400 microg/d periconceptionally.
[本文引用:0]
|
| [43] |
BACKGROUND: During pregnancy, fetal growth causes an increase in the total number of rapidly dividing cells, which leads to increased requirements for folate. Inadequate folate intake leads to a decrease in serum folate concentration, resulting in a decrease in erythrocyte folate concentration, a rise in homocysteine concentration, and megaloblastic changes in the bone marrow and other tissues with rapidly dividing cells OBJECTIVES: To assess the effectiveness of oral folic acid supplementation alone or with other micronutrients versus no folic acid (placebo or same micronutrients but no folic acid) during pregnancy on haematological and biochemical parameters during pregnancy and on pregnancy outcomes. SEARCH METHODS: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 December 2012) and we contacted major organisations working in micronutrient supplementation, including UNICEF Nutrition Section, World Health Organization (WHO) Maternal and Reproductive Health, WHO Nutrition Division, and National Center on Birth defects and Developmnetal Disabilities, US Centers for Disease Control and Prevention (CDC). SELECTION CRITERIA: All randomised, cluster-randomised and cross-over controlled trials evaluating supplementation of folic acid alone or with other micronutrients versus no folic acid (placebo or same micronutrients but no folic acid) in pregnancy. DATA COLLECTION AND ANALYSIS: Two review authors independently assessed trials for inclusion, assessed risk of bias and extracted data. Data were checked for accuracy. MAIN RESULTS: Thirty-one trials involving 17,771 women are included in this review. This review found that folic acid supplementation has no impact on pregnancy outcomes such as preterm birth (risk ratio (RR) 1.01, 95% confidence interval (CI) 0.73 to 1.38; three studies, 2959 participants), and stillbirths/neonatal deaths (RR 1.33, 95% CI 0.96 to 1.85; three studies, 3110 participants). However, improvements were seen in the mean birthweight (mean difference (MD) 135.75, 95% CI 47.85 to 223.68). On the other hand, the review found no impact on improving pre-delivery anaemia (average RR 0.62, 95% CI 0.35 to 1.10; eight studies, 4149 participants; random-effects), mean pre-delivery haemoglobin level (MD -0.03, 95% CI -0.25 to 0.19; 12 studies, 1806 participants), mean pre-delivery serum folate levels (standardised mean difference (SMD) 2.03, 95% CI 0.80 to 3.27; eight studies, 1250 participants; random-effects), and mean pre-delivery red cell folate levels (SMD 1.59, 95% CI -0.07 to 3.26; four studies, 427 participants; random-effects). However, a significant reduction was seen in the incidence of megaloblastic anaemia (RR 0.21, 95% CI 0.11 to 0.38, four studies, 3839 participants). AUTHORS' CONCLUSIONS: We found no conclusive evidence of benefit of folic acid supplementation during pregnancy on pregnancy outcomes.
[本文引用:0]
|
| [44] |
|
| [45] |
Inadequate micronutrient intakes are relatively common in low- and middle-income countries (LMICs), especially among pregnant women, who have increased micronutrient requirements. This can lead to an increase in adverse pregnancy and birth outcomes. This review presents the conclusions of a task force that set out to assess the prevalence of inadequate micronutrient intakes and adverse birth outcomes in LMICs; the data from trials comparing multiple micronutrient supplements (MMS) that contain iron and folic acid (IFA) with IFA supplements alone; the risks of reaching the upper intake levels with MMS; and the cost-effectiveness of MMS compared with IFA. Recent meta-analyses demonstrate that MMS can reduce the risks of preterm birth, low birth weight, and small for gestational age in comparison with IFA alone. An individual-participant data meta-analysis also revealed even greater benefits for anemic and underweight women and female infants. Importantly, there was no increased risk of harm for the pregnant women or their infants with MMS. These data suggest that countries with inadequate micronutrient intakes should consider supplementing pregnant women with MMS as a cost-effective method to reduce the risk of adverse birth outcomes.
[本文引用:0]
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
OBJECTIVE: To provide input to Australian and New Zealand government decision making regarding an optimal strategy to reduce the rate of neural tube defects (NTD). DESIGN: Standard comparative health economic evaluation techniques were employed for a set of intervention options for promoting folate/folic acid consumption in women capable of or planning a pregnancy. Evidence of effectiveness was informed by the international literature and costs were derived for Australia and New Zealand. RESULTS: Population-wide campaigns to promote supplement use and mandatory fortification were the most effective at reducing NTD, at an estimated 36 and 31 fewer cases per annum respectively for Australia and New Zealand, representing an 8 % reduction in the current annual NTD rate. Population-wide and targeted approaches to increase supplement use were cost-effective, at less than $AU 12,500 per disability-adjusted life year (DALY) averted ($US 9893, pound 5074), as was extending voluntary fortification. Mandatory fortification was not cost-effective for New Zealand at $AU 138,500 per DALY ($US 109 609, pound 56,216), with results uncertain for Australia, given widely varying cost estimates. Promoting a folate-rich diet was least cost-effective, with benefits restricted to impact on NTD. CONCLUSIONS: Several options for reducing NTD appear to fall well within accepted societal cost-effectiveness norms. All estimates are subject to considerable uncertainty, exacerbated by possible interactions between interventions, including impacts on currently effective strategies. The Australian and New Zealand governments have decided to proceed with mandatory fortification; it is hoped they will support a rigorous evaluation which will contribute to the evidence base.
[本文引用:0]
|
| [50] |
|
| [51] |
BACKGROUND: It is estimated that 32 million pregnant women suffer from anaemia worldwide. Due to increased metabolic demands, pregnant women are particularly vulnerable to anaemia and vitamin and mineral deficiencies, leading to adverse health effects in both the mother and her baby. Despite the demonstrated benefits of prenatal supplementation with iron and folic acid or multiple micronutrients, poor adherence to routine supplementation has limited the effectiveness of this intervention in many settings. Micronutrient powders for point-of-use fortification are packed, single-dose sachets containing vitamins and minerals that can be added onto prepared food to improve its nutrient profile. The use of multiple micronutrient powders for point-of-use fortification of foods in pregnant women could be an alternative intervention to prenatal micronutrient supplementation. OBJECTIVES: To assess the effects of prenatal home (point-of-use) fortification of foods with multiple micronutrient powders on maternal and newborn health. SEARCH METHODS: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 January 2015) and the International Clinical Trials Registry Platform (ICTRP) (31 January 2015). We also contacted relevant agencies to identify ongoing and unpublished studies. SELECTION CRITERIA: Randomised controlled trials (both individual and cluster randomisation) and quasi-randomised trials, irrespective of language or publication status.The intervention was micronutrient powders for point-of-use fortification of foods, containing at least three micronutrients with one of them being iron, provided to pregnant women of any gestational age and parity. Five comparison groups were considered: no intervention/placebo, iron and folic acid supplements, iron-only supplements, folic-acid only supplements, and multiple micronutrients in supplements. DATA COLLECTION AND ANALYSIS: Two review authors independently assessed the eligibility of studies, extracted and checked data accuracy, and assessed the risk of bias of included studies. MAIN RESULTS: Our search identified 12 reports (relating to six studies). We included two cluster-randomised controlled trials (involving 1172 women) - these trials were considered to be at a moderate to high risk of bias due to methodological limitations. One trial is ongoing, and three studies were excluded. Micronutrient powders for point-of-use fortification of foods versus iron and folic acid supplementsOne trial (involving 478 pregnant women attending 42 antenatal care centres) compared micronutrient powders containing iron, folic acid, vitamin C and zinc with iron and folic acid tablets provided daily from 14 to 22 weeks to 32 weeks' gestation. The trial did not report on any of this review's primary outcomes: maternal anaemia at or near term, maternal iron deficiency, maternal mortality, adverse effects, low birthweight, preterm births. Nor did the trial report on the majority of this review's secondary outcomes, with the exception of maternal adherence. Adherence to micronutrient powders was lower than adherence to iron and folic acid supplements (risk ratio (RR) 0.76, 95% confidence interval (CI) 0.66 to 0.87, one study, n = 405). Micronutrient powders for point-of-use fortification of foods versus same multiple micronutrients in supplementsOne study (involving 694 pregnant women from 18 communities), compared micronutrient powders containing iron, folic acid, vitamin C, zinc, iodine, vitamin E and vitamin B12 with tablets containing the same seven micronutrients. There was no difference in maternal anaemia at 37 weeks of gestation (RR 0.92, 95% CI 0.53 to 1.59, one study, n = 470, very low quality evidence). The trial did not report on any of this review's other primary outcomes in relation to maternal iron deficiency, maternal mortality, adverse effects, low birthweight, or preterm birth. In terms of this review's secondary outcomes, the included trial did not report on the majority of this review's prespecified secondary outcomes with one exception - there was no clear difference in maternal haemoglobin Hb or near term (mean difference (MD) 1.0 g/L, 95% CI -1.77 to 3.77, one study, n = 470). AUTHORS' CONCLUSIONS: Limited evidence suggests that micronutrient powders for point-of-use fortification of foods have no clear difference as multiple micronutrient supplements on maternal anaemia (very low quality evidence) and Hb at or near term. There is limited evidence to suggest that women were more likely to adhere to taking tablets than using micronutrient powders.The overall quality of evidence was judged very low (due to methodological limitations), and no evidence was available for the majority of primary and secondary outcomes. Therefore, more evidence is needed to assess the potential benefits or harms of the use of micronutrient powders in pregnant women on maternal and infant health outcomes. Future trials should also assess adherence to micronutrient powders and be adequately powered to evaluate the effects on birth outcomes and morbidity.
[本文引用:0]
|
| [52] |
Introduction: The mandatory fortification of staple foods with folic acid to prevent neural tube defects (NTDs) began in the USA in 1998. Since then, more than 50 countries around the world have followed suit.
[本文引用:1]
Methods: Selective literature review including national study results. Results and discussion: Women of child-bearing age need sufficient body stores of folate before conception to prevent folate-sensitive NTDs, which make up 20% to 60% of all NTDs. Merely recommending folic acid supplementation before conception has been found to be an unsuitable strategy. Ingestion of folate-fortified food markedly increases folate intake, generally by about 50% of the recommended daily total intake. In Germany at present, debate surrounds the issue whether folate intake should be raised by mandatory folate supplementation, which will affect the entire population. Folate deficiency is associated with a higher risk of cancer and other diseases; on the other hand, there is concern that very high folic acid intake might promote the growth of pre-neoplastic lesions. There are no consistent study findings to support the latter hypothesis, and the evidence for it is derived from research in animals whose folate metabolism differs from that in humans. About 800 pregnancies with NTD are diagnosed each year in Germany; in most cases, the pregnancy is terminated after positive prenatal screening. The incidence of NTDs in Germany is estimated at 12.36 per 10 000 births (a mean figure derived from registry data in Mainz and Saxony-Anhalt) and is thus much higher than the mean incidence across Europe, 7.88 per 10 000 births (EUROCAT data for 2004-2008). Mandatory folic acid fortification should be adopted, as it is a highly effective and inexpensive way to prevent NTDs. |
| [53] |
Scope By increasing blood folate concentrations, folic acid supplementation reduces risk for neural tube defect-affected pregnancies, and lowers homocysteine concentrations. We assessed response of red blood cell (RBC) and serum folate to folic acid supplementation, and examined association of response with the genetic polymorphism C677T of the methylenetetrahydrofolate NAD(P)H (MTHFR) gene. Methods and results Randomized, controlled, crossover trial with two folic acid supplement treatment periods and a 30-week washout period. The primary outcome is blood folate (serum and RBC) concentrations. Volunteers (n = 142) aged 1869 were randomized to two of three doses (0, 200, and 400 g) of folic acid for 12 weeks. Serum folate response depended on treatment period with significant responses to 200 g seen only in the second treatment periods (4.4 ng/mL or 3.4 ng/mL). Additionally, serum folate increased as folic acid dose increased to 400 g (p < 0.01) and response was greater after the washout period (8.7 ng/mL), than after a 6-week run-in (2.3 ng/mL). The differential change attributable to a daily supplement of 400 g compared to 200 g was 96.8 ng/mL; while the change attributable to 400 g compared to 0 g was 121.4. Increases in RBC folate concentrations with 400 g occurred within MTHFR gene mutation (C677T); and in the African American group. Conclusion Serum folate concentration is responsive to modest increases in folic acid intake. RBC folate increases only with higher additional doses of folic acid supplementation, and this is true for each MTHFR C677T genotype.
[本文引用:1]
|
| [54] |
|
| [55] |
Using data from a recent case-control study, a woman's risk of having a child with a neural tube defect (NTD) was found to be associated with early pregnancy red cell folate levels in a continuous dose-response relationship. These findings were used to calculate the reduction in NTD cases that would be expected under two different strategies to raise folate levels. Targeting high-risk individuals has a small effect on the population prevalence but can substantially change an individual's risk. Targeting the population produces a small change in individual risk but has a large effect on the population prevalence. Supplementation of high-risk women would be the most efficient method to implement the high-risk strategy, while food fortification would be preferable for the population approach. The current guidelines for the prevention of NTD are for an increased folic acid intake of 0.4 mg per day. This would result in a 48% reduction in NTDs, which may be near optimal. The two intervention strategies should be considered complementary in prevention of NTDs.
[本文引用:1]
|
| [56] |
|
| [57] |
BACKGROUND AND METHODS: Periconceptional administration of folic acid can reduce a woman's risk of having a fetus or infant with a neural-tube defect. As part of a public health campaign conducted from 1993 to 1995 in an area of China with high rates of neural-tube defects (the northern region) and one with low rates (the southern region), we evaluated the outcomes of pregnancy in women who were asked to take a pill containing 400 microg of folic acid alone daily from the time of their premarital examination until the end of their first trimester of pregnancy. RESULTS: Among the fetuses or infants of 130,142 women who took folic acid at any time before or during pregnancy and 117,689 women who had not taken folic acid, we identified 102 and 173, respectively, with neural-tube defects. Among the fetuses or infants of women who registered before their last menstrual period and who did not take any folic acid, the rates of neural-tube defects were 4.8 per 1000 pregnancies of at least 20 weeks' gestation in the northern region and 1.0 per 1000 in the southern region. Among the fetuses or infants of the women with periconceptional use of folic acid, the rates were 1.0 per 1000 in the northern region and 0.6 per 1000 in the southern region. The greatest reduction in risk occurred among the fetuses or infants of a subgroup of women in the northern region with periconceptional use who took folic acid pills more than 80 percent of the time (reduction in risk, 85 percent as compared with the fetuses or infants of women who registered before their last menstrual period and who took no folic acid; 95 percent confidence interval, 62 to 94 percent) [corrected]. In the southern region the reduction in risk among the fetuses or infants of women with periconceptional use of folic acid was also significant (reduction in risk, 41 percent; 95 percent confidence interval, 3 to 64 percent). CONCLUSIONS: Periconceptional intake of 400 microg of folic acid daily can reduce the risk of neural-tube defects in areas with high rates of these defects and in areas with low rates.
[本文引用:1]
|
| [58] |
In accordance with a previous protocol, a second cohort of 254 mothers with a history of previous neural tube defect (NTD) births was before a subsequent conception and continued until the time of the second missed menstrual period. There were 2 NTD recurrences (0.9% of 234 infants/fetuses examined), which is significantly fewer than the 11 NTD recurrences (5.1% of 215 infants/fetuses examined) born to 219 unsupplemented (US) mothers in the same centres over the same period. When the data for the two cohorts were combined, the overall recurrence rates were 0.7% for 454 fully supplemented (FS) mothers and 4.7% for 519 US mothers. The recurrence rates after 1 previous NTD were 0.5% for FS and 4.2% for US mothers: after 2 or more previous NTDs, 2.3% for FS and 9.6% for US. There were no recurrences among the offspring of a further 114 mothers whose duration of supplementation fell short of the full regimen (partially supplemented, PS).
[本文引用:1]
|
| [59] |
Objective: To review the impact of folic acid fortification of flour on the prevalence of neural tube defects (NTD).
[本文引用:1]
Design: Systematic review of the literature on MEDLINE via PubMed, Scopus, OvidSP and LILACS (Latin American and Caribbean Health Sciences Literature) reporting the impact of folic acid fortification of flour on the prevalence of NTD in 2000-2011. Focusing on Santiago of Chile's birth defects registry (1999-2009) and the monitoring of flour fortification, we analysed the prevalence (NTD cases/10 000 births) pre and post flour fortification and the percentile distribution of folic acid content in flour (2005-2009). We explored the potential association between median folic acid in flour (mg/kg) and the prevalence of NTD. Setting: Chile, Argentina, Brazil, Canada, Costa Rica, Iran, Jordan, South Africa and the USA. Subjects: Live births and stillbirths. Results: Twenty-seven studies that met inclusion criteria were evaluated. Costa Rica showed a significant reduction in NTD (similar to 60%). Prevalence in Chile decreased from 18.6 to 7.3/10 000 births from 1999 to 2007 and showed a slight increase to 8.5 in 2008-2009, possibly due to changes in fortification limits. When we related the prevalence of NTD with levels of flour fortification, the lowest prevalence was observed at a folic acid level of 1.5 mg/kg. Conclusions: Fortification of flour with folic acid has had a major impact on NTD in all countries where this has been reported. Chile showed a 55% reduction in NTD prevalence between 1999 and 2009. There is a need to constantly monitor the levels of flour fortification to maximize benefits and prevent the potential risk of folic acid excess, moreover to be vigilant for any new adverse effects associated with excess. |
| [60] |
PURPOSE: Folate required to achieve desirable red blood cell (RBC) folate concentrations within 4-8 weeks pre-pregnancy is not known. We studied the effect of supplementation with 400 or 800 microg/day folate in achieving RBC-folate >/=906 nmol/L. METHODS: Non-pregnant women were randomized to receive multinutrient supplements containing 400 microg/day (n = 100) or 800 microg/day (n = 101) folate [folic acid and (6S)-5-CH3-H4folate-Ca (1:1)]. The changes of folate biomarkers were studied after 4 and 8 weeks in the 198 women who returned at least for visit 2. RESULTS: At baseline, 12 of the 198 participants (6.1%) had RBC-folate <340 nmol/L, but 88% had levels <906 nmol/L. The RBC-folate concentrations increased significantly in the 800 microg/day (mean +/- SD = 652 +/- 295 at baseline; 928 +/- 330 at 4 weeks; and 1218 +/- 435 nmol/L at 8 weeks) compared with the 400 microg/day [632 +/- 285 at baseline (p = 0.578); 805 +/- 363 at 4 weeks (p < 0.001); 1021 +/- 414 nmol/L at 8 weeks (p < 0.001)]. The changes of RBC-folate were greater in the 800 microg/day than in the 400 microg/day at any time (changes after 8 weeks: 566 +/- 260 vs. 389 +/- 229 nmol/L; p < 0.001). Significantly more women in the 800 microg group achieved desirable RBC-folate concentrations at 4 weeks (45.5 vs. 31.3%; p = 0.041) or 8 weeks (83.8 vs. 54.5%; p < 0.001) compared with the 400 microg group. RBC-folate levels below the population median (590 nmol/L) were associated with a reduced response to supplements. CONCLUSIONS: 88% of the women had insufficient RBC-folate to prevent birth defects, while 6.1% had deficiency. Women with low RBC-folate were unlikely to achieve desirable levels within 4-8 weeks, unless they receive 800 microg/day. The current supplementation recommendations are not sufficient in countries not applying fortification. TRIALS REGISTER: The trial was registered at The German Clinical Trials Register: DRKS-ID: DRKS00009770.
[本文引用:1]
|
| [61] |
BACKGROUND: Folic acid supplementation is recommended for all women of child-bearing age to prevent neural tube defects (NTDs). A nation-wide folic acid supplementation program was implemented in rural areas of China since 2009; however, changes in plasma folate levels in pregnant women were unknown. METHODS: A cross-sectional survey was conducted in 2011 to 2012, with 1736 pregnant women enrolled, and results were compared with a previous survey in 2002 to 2004. A microbiological method was used to determine plasma folate levels. Preprogram and postprogram median plasma folate concentrations were compared while stratified by prevalence of NTDs and residence. RESULTS: In the high NTD prevalence population, plasma folate concentration increased to 33.4 (18.7, 58.4) nmol/L in the postprogram sample, which is 2.9 times of the preprogram. In the low NTD prevalence population, plasma folate increased to 67.9 (44.5, 101.9) nmol/L, which is 1.9 times of the preprogram. Gaps remained in plasma folate levels with respect to prevalence of NTDs and residence. Folic acid supplementation has a strong impact on plasma folate concentrations. Earlier supplementation (before the last menstrual period), increased supplementation frequency and more total days of supplementation were associated with a higher plasma folate concentration as demonstrated in both the high- and low-prevalence populations. CONCLUSION: Plasma folate levels among pregnant Chinese women increased dramatically after the nation-wide folic acid supplementation program in both rural and urban areas, and in populations of high and low NTD prevalence. The nation-wide program should have a component to ensure that supplementation begins before pregnancy.
[本文引用:1]
|
| [62] |
BACKGROUND: Optimal blood folate levels of women before pregnancy are critical to the prevention of neural tube defects (NTDs). However, few studies have focused on blood folate levels of women planning to become pregnant. The aims of this study were to assess plasma folate levels in women who planned to become pregnant in a population with high prevalence of NTDs, to identify factors associated with plasma folate levels, and to evaluate the risk of NTDs at the population level. METHODS: A total of 2065 women were enrolled at the time of premarital health check-up in two rural counties in northern China from November 2009 to December 2012. Fasting venous blood samples were collected and plasma folate concentrations were measured by microbiological method. RESULTS: The overall median of plasma folate was 10.5 nmol/L. 50% of the women had a plasma folate level below 10.5 nmol/L, a cutoff for megaloblastic anemia, and 88% below 18 nmol/L, a proposed optimal plasma folate level for the prevention of NTDs. Folic acid supplementation was the only factor to be associated with plasma folate concentrations, but only 1.9% of the women reported having taken folic acid supplements. A population risk of 29.3 NTD cases per 10,000 births was predicted. CONCLUSION: Women who planned to become pregnant had very low plasma folate in the population. Folic acid supplementation was the only factor to be associated with a high plasma folate concentration. High NTD risk would remain if women would get pregnant without having taken folic acid supplements. Birth Defects Research 109:1039-1047, 2017. (c) 2017 Wiley Periodicals, Inc.
[本文引用:1]
|
| [63] |
BACKGROUND: There are no large randomized trials of the effect of folic acid dosing regimens on blood folate and homocysteine concentrations. OBJECTIVE: We aimed to evaluate the changes in folate and homocysteine concentrations in response to different folic acid doses and to withdrawal in young women not exposed to other sources of folic acid. DESIGN: Women (n = 1108) were randomly assigned to 1 of 6 intervention groups for which daily intakes of folic acid for 6 mo were 100 microg 1 time/d, 25 microg 4 times/d, 400 microg 1 time/d, 100 microg 4 times/d, 4000 microg 1 time/d, or 4000 microg 1 time/wk. Plasma and red blood cell folate and homocysteine concentrations were measured at baseline; at 1, 3, and 6 mo; and 3 mo after the discontinuation of folic acid. RESULTS: Folate and homocysteine concentrations were not different at baseline between the groups who had the same daily intake of folic acid as a single dose or multiple doses (P = 0.058). Plasma folate concentrations plateaued at 3 mo with 108% (95% CI: 97.7%, 120%), 259% (95% CI: 240%, 279%), 460% (95% CI: 417%, 503%), and 142% (95% CI: 123%, 162%) observed increases for the folic acid groups receiving 100, 400, and 4000 microg/d and 4000 microg/wk, respectively. The rate of reduction in folate concentrations during the 3 mo after cessation of folic acid was dose-dependent-higher intakes were associated with faster reductions. CONCLUSIONS: Changes in folate and homocysteine concentrations were unaffected by different dosing schedules. After folic acid cessation, blood folate declined rapidly, which indicated that the intervention-enhanced folate status was rapidly diminished.
[本文引用:1]
|
| [64] |
AbstractPURPOSE: To investigate whether dietary folate or multivitamin folic acid taken 3 months before conception and during the first 3 months of pregnancy reduces the risk of isolated occurrent neural tube defect (NTD)-affected pregnancies. METHODS: This population-based case control study conducted between 1992 and 1997 included 179 women with NTD-affected pregnancies and 288 randomly selected controls. Women completed a food frequency questionnaire and were interviewed about lifestyle behaviors, pregnancy histories and use of multivitamins. RESULTS: Use of 0.4 mg or more of multivitamin folic acid at least 3 times per week during the periconceptional period showed no statistically significant reduction in NTD risk [adjusted odds ratio (AOR) = 0.55, 95% confidence interval (CI) = 025, 1.22]. After adjusting for covariates, protective effects for NTDs were observed at the highest quartiles of dietary folate and total folate (daily dietary folate plus daily multivitamin folic acid); the respective odds ratios were 0.40 (95% CI = 0.19, 0.84) and 0.35 (95% CI = 0.17, 0.72). CONCLUSIONS: This study illustrates some of the difficulties in determining effects of folic acid and dietary folate in a population where the consumption of foods rich in folate and the use of multivitamins are increasing and the rate of NTDs is declining. Studies are needed to monitor future changes in folate levels and their effect on health. |
| [65] |
With a case-control study, we investigated whether periconceptional intake of supplemental or dietary folate reduced the risk of having a neural tube defect (NTD)-affected pregnancy. Mothers of 549 (88% of eligible) cases and 540 (88%) controls were interviewed in person about vitamin supplements used in either the 3 months before or the 3 months after conception and also about usual diet in the 3 months before conception. Women with any use of a folic acid-containing vitamin in the 3 months before conception had a lower risk of having an NTD-affected pregnancy [odds ratio (OR) = 0.65; 95% confidence interval (CI) = 0.45-0.94]. ORs were similar for 3 levels (< 0.4, 0.4-0.9, and > 0.9 mg per day) of average daily intake of folic acid. Any level of use in the first 3 months after conception resulted in a lowered risk as well (OR = 0.60; 95% CI = 0.46-0.79). Reduced risks were less marked for Hispanics and were not observed among women who graduated from college. Modest reduced risks were noted among non-vitamin users whose estimated daily dietary intake of folate was more than 0.227 mg. We observed decreasing risk with increasing folate intake from combined dietary sources and vitamin supplements. A reduction in NTD risk associated with folate intake is consistent with other studies; however, the reduced risk may be particular to subsets of the population, primarily non-Hispanic women and women whose education does not exceed high school.
[本文引用:1]
|
| [66] |
Erythropoiesis is the process in which new erythrocytes are produced. These new erythrocytes replace the oldest erythrocytes (normally about one percent) that are phagocytosed and destroyed each day. Folate, vitamin B12, and iron have crucial roles in erythropoiesis. Erythroblasts require folate and vitamin B12 for proliferation during their differentiation. Deficiency of folate or vitamin B12 inhibits purine and thymidylate syntheses, impairs DNA synthesis, and causes erythroblast apoptosis, resulting in anemia from ineffective erythropoiesis. Erythroblasts require large amounts of iron for hemoglobin synthesis. Large amounts of iron are recycled daily with hemoglobin breakdown from destroyed old erythrocytes. Many recently identified proteins are involved in absorption, storage, and cellular export of nonheme iron and in erythroblast uptake and utilization of iron. Erythroblast heme levels regulate uptake of iron and globin synthesis such that iron deficiency causes anemia by retarded production rates with smaller, less hemoglobinized erythrocytes.
[本文引用:2]
|
| [67] |
OBJECTIVE: The present prospective study examines the levels of maternal plasma folate, vitamin B12 and homocysteine in normotensive control (NC) women and women with preeclampsia (PE) from early pregnancy till delivery. METHODS: The present study includes 126 NC and 62 PE women. Maternal blood was collected at 3 time points during pregnancy (T1 = 16th-20th weeks, T2 = 26th-30th weeks and T3 = at delivery). Levels of folate, vitamin B12 and homocysteine were estimated by the chemiluminescent microparticle immunoassay technology. RESULTS: Maternal plasma folate levels were similar between NC and PE women at all the time points across gestation. Maternal plasma vitamin B12 levels were significantly higher in PE (p < 0.05) as compared with NC at T2. Maternal plasma homocysteine levels were higher in PE as compared with NC at all the time points, i.e. T1, T2 (p < 0.05 for both) and T3 (p < 0.01). CONCLUSION: Our results indicate that higher homocysteine levels exist in women with PE from early pregnancy and continue till delivery.
[本文引用:2]
|
| [68] |
BACKGROUND: Although taking supplements that contain 400 microg of folic acid before and during early pregnancy reduces a woman's risk for having a baby with a neural-tube defect (NTD), the effects of such supplements on other pregnancy outcomes remain unclear. We examined whether the use of such supplements affects the occurrence of miscarriage. METHODS: Participants were women in China who had taken part in a recent folic acid campaign to prevent NTDs and who had registered in this campaign before they became pregnant for the first time. We examined the risk for miscarriage among women who had confirmed pregnancies and who had or had not taken pills containing only 400 microg of folic acid before and during early pregnancy. RESULTS: The overall rate of miscarriage was 9.1% (2155/23806). The rates of miscarriage among women who had and had not taken folic acid pills before and during the first trimester were 9.0% and 9.3%, respectively (risk ratio 0.97 [95% CI 0.84-1.12]). The distributions of gestational age at pregnancy diagnosis and at miscarriage were similar for both groups of women. INTERPRETATION: In this population-based study of a cohort of women whose use of folic acid supplements while pregnant had been previously documented and who had been pregnant for the first time, we found no evidence that daily consumption of 400 microg of folic acid before and during early pregnancy influenced their risk for miscarriage.
[本文引用:1]
|
| [69] |
Current results regarding the effect of folic acid (FA) supplement use on gestational hypertension (GH) and preeclampsia are limited and inconsistent. We aimed to investigate whether FA supplement use was associated with GH and preeclampsia. Participants from the Tongji Maternal and Child Health Cohort with information on periconceptional FA supplement use and diagnosis of GH/preeclampsia were included (n=4853). Robust Poisson regression was used to assess the association of FA supplement use and GH and preeclampsia. Among the 4853 participants in this study, 1161 (23.9%) and 161 (3.3%) women were diagnosed with GH and preeclampsia, respectively. The risk ratio of developing GH was higher in women who used >/=800 microg/d FA supplement from prepregnancy through midpregnancy than nonusers (risk ratio, 1.33 [1.08-1.65]). After adjusting for social-demographic, reproductive, lifestyle factors, family history of hypertension, other supplement use, and gestational weight gain, the adverse association remained significant (risk ratio, 1.32 [1.06-1.64]). Restricting the analysis among women with normal weight, without family history of hypertension, and without gestational diabetes mellitus, the positive FA-GH association still existed. We did not find any significant association between FA supplement use and preeclampsia regardless of adjustment. High-dose (>/=800 microg/d) FA supplement use from prepregnancy through midpregnancy was associated with increased risk of GH. Attention should be given to avoid the potential risk of GH due to inappropriate FA supplement use in women who are planning or capable of pregnancy.
[本文引用:1]
|
| [70] |
|
| [71] |
IMPORTANCE: Prenatal folic acid supplements reduce the risk of neural tube defects in children, but it has not been determined whether they protect against other neurodevelopmental disorders. OBJECTIVE: To examine the association between maternal use of prenatal folic acid supplements and subsequent risk of autism spectrum disorders (ASDs) (autistic disorder, Asperger syndrome, pervasive developmental disorder-not otherwise specified [PDD-NOS]) in children. DESIGN, SETTING, AND PATIENTS: The study sample of 85,176 children was derived from the population-based, prospective Norwegian Mother and Child Cohort Study (MoBa). The children were born in 2002-2008; by the end of follow-up on March 31, 2012, the age range was 3.3 through 10.2 years (mean, 6.4 years). The exposure of primary interest was use of folic acid from 4 weeks before to 8 weeks after the start of pregnancy, defined as the first day of the last menstrual period before conception. Relative risks of ASDs were estimated by odds ratios (ORs) with 95% CIs in a logistic regression analysis. Analyses were adjusted for maternal education level, year of birth, and parity. MAIN OUTCOME MEASURE: Specialist-confirmed diagnosis of ASDs. RESULTS: At the end of follow-up, 270 children in the study sample had been diagnosed with ASDs: 114 with autistic disorder, 56 with Asperger syndrome, and 100 with PDD-NOS. In children whose mothers took folic acid, 0.10% (64/61,042) had autistic disorder, compared with 0.21% (50/24,134) in those unexposed to folic acid. The adjusted OR for autistic disorder in children of folic acid users was 0.61 (95% CI, 0.41-0.90). No association was found with Asperger syndrome or PDD-NOS, but power was limited. Similar analyses for prenatal fish oil supplements showed no such association with autistic disorder, even though fish oil use was associated with the same maternal characteristics as folic acid use. CONCLUSIONS AND RELEVANCE: Use of prenatal folic acid supplements around the time of conception was associated with a lower risk of autistic disorder in the MoBa cohort. Although these findings cannot establish causality, they do support prenatal folic acid supplementation.
[本文引用:1]
|
| [72] |
Importance: The association of maternal use of folic acid and multivitamin supplements before and during pregnancy with the risk of autism spectrum disorder (ASD) in offspring is unclear. Objective: To examine the associations between the use of maternal folic acid and multivitamin supplements before and during pregnancy and the risk of ASD in offspring. Design, Setting, and Participants: A case-control cohort study of 45300 Israeli children born between January 1, 2003, and December 31, 2007, were followed up from birth to January 26, 2015, for the risk of ASD. The cases were all children diagnosed with ASD and the controls were a random sample of 33% of all live-born children. Exposures: Maternal vitamin supplements were classified for folic acid (vitamin B9), multivitamin supplements (Anatomical Therapeutic Chemical A11 codes vitamins A, B, C, and D), and any combination thereof exposed in the intervals before and during pregnancy. Main Outcomes and Measures: The association between maternal vitamin supplementation and the risk of ASD in offspring was quantified with relative risks (RRs) and their 95% CIs fitting Cox proportional hazards regression models adjusted for confounders. Sensitivity analyses were performed to test the robustness of the results. Results: Of the 45300 children in the study (22090 girls and 23210 boys; mean [SD] age, 10.0 [1.4] years at the end of follow-up), 572 (1.3%) received a diagnosis of ASD. Maternal exposure to folic acid and/or multivitamin supplements before pregnancy was statistically significantly associated with a lower likelihood of ASD in the offspring compared with no exposure before pregnancy (RR, 0.39; 95% CI, 0.30-0.50; P < .001). Maternal exposure to folic acid and/or multivitamin supplements during pregnancy was statistically significantly associated with a lower likelihood of ASD in offspring compared with no exposure during pregnancy (RR, 0.27; 95% CI, 0.22-0.33; P < .001). Corresponding RRs were estimated for maternal exposure to folic acid before pregnancy (RR, 0.56; 95% CI, 0.42-0.74; P = .001), maternal exposure to folic acid during pregnancy (RR, 0.32; 95% CI, 0.26-0.41; P < .001), maternal exposure to multivitamin supplements before pregnancy (RR, 0.36; 95% CI, 0.24-0.52; P < .001), and maternal exposure to multivitamin supplements during pregnancy (RR, 0.35; 95% CI, 0.28-0.44; P < .001). The results generally remained statistically significant across sensitivity analyses. Conclusions and Relevance: Maternal exposure to folic acid and multivitamin supplements before and during pregnancy is associated with a reduced risk of ASD in the offspring compared with the offspring of mothers without such exposure.
[本文引用:1]
|
| [73] |
BACKGROUND: Periconceptional folate is essential for proper neurodevelopment. OBJECTIVE: Maternal folic acid intake was examined in relation to the risk of autism spectrum disorder (ASD) and developmental delay (DD). DESIGN: Families enrolled in the CHARGE (CHildhood Autism Risks from Genetics and Environment) Study from 2003 to 2009 were included if their child had a diagnosis of ASD (n = 429), DD (n = 130), or typical development (TD; n = 278) confirmed at the University of California Davis Medical Investigation of Neurodevelopmental Disorders Institute by using standardized clinical assessments. Average daily folic acid was quantified for each mother on the basis of dose, brands, and intake frequency of vitamins, supplements, and breakfast cereals reported through structured telephone interviews. RESULTS: Mean (+/-SEM) folic acid intake was significantly greater for mothers of TD children than for mothers of children with ASD in the first month of pregnancy (P1; 779.0 +/- 36.1 and 655.0 +/- 28.7 mug, respectively; P < 0.01). A mean daily folic acid intake of >/=600 mug (compared with <600 mug) during P1 was associated with reduced ASD risk (adjusted OR: 0.62; 95% CI: 0.42, 0.92; P = 0.02), and risk estimates decreased with increased folic acid (P-trend = 0.001). The association between folic acid and reduced ASD risk was strongest for mothers and children with MTHFR 677 C>T variant genotypes. A trend toward an association between lower maternal folic acid intake during the 3 mo before pregnancy and DD was observed, but not after adjustment for confounders. CONCLUSIONS: Periconceptional folic acid may reduce ASD risk in those with inefficient folate metabolism. The replication of these findings and investigations of mechanisms involved are warranted.
[本文引用:1]
|
| [74] |
BACKGROUND: To examine the prospective association between multivitamin supplementation during pregnancy and biomarker measures of maternal plasma folate and vitamin B12 levels at birth and child's Autism Spectrum Disorder (ASD) risk. METHODS: This report included 1257 mother-child pairs, who were recruited at birth and prospectively followed through childhood at the Boston Medical Center. ASD was defined from diagnostic codes in electronic medical records. Maternal multivitamin supplementation was assessed via questionnaire interview; maternal plasma folate and B12 were measured from samples taken 2-3 days after birth. RESULTS: Moderate (3-5 times/week) self-reported supplementation during pregnancy was associated with decreased risk of ASD, consistent with previous findings. Using this as the reference group, low (5 times/week) supplementation was associated with increased risk of ASD. Very high levels of maternal plasma folate at birth (>/=60.3 nmol/L) had 2.5 times increased risk of ASD [95% confidence interval (CI) 1.3, 4.6] compared to folate levels in the middle 80th percentile, after adjusting for covariates including MTHFR genotype. Similarly, very high B12 (>/=536.8 pmol/L) showed 2.5 times increased risk (95% CI 1.4, 4.5). CONCLUSION: There was a 'U shaped' relationship between maternal multivitamin supplementation frequency and ASD risk. Extremely high maternal plasma folate and B12 levels at birth were associated with ASD risk. This hypothesis-generating study does not question the importance of consuming adequate folic acid and vitamin B12 during pregnancy; rather, raises new questions about the impact of extremely elevated levels of plasma folate and B12 exposure in-utero on early brain development.
[本文引用:1]
|
| [75] |
The 'Clinical Guidelines for Obstetrical Practice, 2011 edition' were revised and published as a 2014 edition (in Japanese) in April 2014 by the Japan Society of Obstetrics and Gynecology and the Japan Association of Obstetricians and Gynecologists. The aims of this publication include the determination of current standard care practices for pregnant women in Japan, the widespread use of standard care practices, the enhancement of safety in obstetrical practice, the reduction of burdens associated with medico-legal and medico-economical problems, and a better understanding between pregnant women and maternity-service providers. The number of Clinical Questions and Answers items increased from 87 in the 2011 edition to 104 in the 2014 edition. The Japanese 2014 version included a Discussion, a List of References, and some Tables and Figures following the Answers to the 104 Clinical Questions; these additional sections covered common problems and questions encountered in obstetrical practice, helping Japanese readers to achieve a comprehensive understanding. Each answer with a recommendation level of A, B or C was prepared based principally on 'evidence' or a consensus among Japanese obstetricians in situations where 'evidence' was weak or lacking. Answers with a recommendation level of A or B represent current standard care practices in Japan. All 104 Clinical Questions and Answers items, with the omission of the Discussion, List of References, and Tables and Figures, are presented herein to promote a better understanding among English readers of the current standard care practices for pregnant women in Japan.
[本文引用:1]
|
| [76] |
|
| [77] |
Neural tube defects (NTDs) are congenital structural abnormalities of the central nervous system and vertebral column. Neural tube defects may occur as an isolated malformation, in combination with other malformations, as part of a genetic syndrome, or as a result of teratogenic exposure (1). Neural tube defects are the second-most-common major congenital anomaly (2) after cardiac malformations, and their prevalence varies by geographic region, race, and environmental factors (3). Outcomes and disabilities depend on level and extent of lesion; for instance, anencephaly is incompatible with life but most infants with spina bifida will survive after surgical repair (4). Importantly, and in contrast to many other congenital abnormalities, primary prevention of NTDs is possible with folic acid. In addition, prenatal screening and diagnosis are widely available, and fetal surgery has improved outcomes for some newborns. The purpose of this document is to provide information about NTDs and make management recommendations for the pregnancy complicated by a fetal NTD.
[本文引用:0]
|
| [78] |
Preconception wellness reflects a woman's overall health before conception as a strategy to affect health outcomes for the woman, the fetus, and the infant. Preconception wellness is challenging to measure because it attempts to capture health status before a pregnancy, which may be affected by many different service points within a health care system. The Clinical Workgroup of the National Preconception Health and Health Care Initiative proposes nine core measures that can be assessed at initiation of prenatal care to index a woman's preconception wellness. A two-stage web-based modified Delphi survey and a face-to-face meeting of key opinion leaders in women's reproductive health resulted in identifying seven criteria used to determine the core measures. The Workgroup reached unanimous agreement on an aggregate of nine preconception wellness measures to serve as a surrogate but feasible assessment of quality preconception care within the larger health community. These include indicators for: 1) pregnancy intention, 2) access to care, 3) preconception multivitamin with folic acid use, 4) tobacco avoidance, 5) absence of uncontrolled depression, 6) healthy weight, 7) absence of sexually transmitted infections, 8) optimal glycemic control in women with pregestational diabetes, and 9) teratogenic medication avoidance. The focus of the proposed measures is to quantify the effect of health care systems on advancing preconception wellness. The Workgroup recommends that health care systems adopt these nine preconception wellness measures as a metric to monitor performance of preconception care practice. Over time, monitoring these baseline measures will establish benchmarks and allow for comparison within and among regions, health care systems, and communities to drive improvements.
[本文引用:0]
|
| [79] |
|
| [80] |
|
| [81] |
A randomised double-blind prevention trial with a factorial design was conducted at 33 centres in seven countries to determine whether supplementation with folic acid (one of the vitamins in the B group) or a mixture of seven other vitamins (A,D,B1,B2,B6,C and nicotinamide) around the time of conception can prevent neural tube defects (anencephaly, spina bifida, encephalocele). A total of 1817 women at high risk of having a pregnancy with a neural tube defect, because of a previous affected pregnancy, were allocated at random to one of four groups--namely, folic acid, other vitamins, both, or neither. 1195 had a completed pregnancy in which the fetus or infant was known to have or not have a neural tube defect; 27 of these had a known neural tube defect, 6 in the folic acid groups and 21 in the two other groups, a 72% protective effect (relative risk 0.28, 95% confidence interval 0.12-0.71). The other vitamins showed no significant protective effect (relative risk 0.80, 95% Cl 0.32-1.72). There was no demonstrable harm from the folic acid supplementation, though the ability of the study to detect rare or slight adverse effects was limited. Folic acid supplementation starting before pregnancy can now be firmly recommended for all women who have had an affected pregnancy, and public health measures should be taken to ensure that the diet of all women who may bear children contains an adequate amount of folic acid.
[本文引用:1]
|
| [82] |
Although peri-conceptional folic acid (FA) supplementation can prevent a proportion of neural tube defects (NTD), there is increasing evidence that many NTD are FA non-responsive. The vitamin-like molecule inositol may offer a novel approach to preventing FA-non-responsive NTD. Inositol prevented NTD in a genetic mouse model, and was well tolerated by women in a small study of NTD recurrence. In the present study, we report the Prevention of Neural Tube Defects by Inositol (PONTI) pilot study designed to gain further experience of inositol usage in human pregnancy as a preliminary trial to a future large-scale controlled trial to evaluate efficacy of inositol in NTD prevention. Study subjects were UK women with a previous NTD pregnancy who planned to become pregnant again. Of 117 women who made contact, ninety-nine proved eligible and forty-seven agreed to be randomised (double-blind) to peri-conceptional supplementation with inositol plus FA or placebo plus FA. In total, thirty-three randomised pregnancies produced one NTD recurrence in the placebo plus FA group (n 19) and no recurrences in the inositol plus FA group (n 14). Of fifty-two women who declined randomisation, the peri-conceptional supplementation regimen and outcomes of twenty-two further pregnancies were documented. Two NTD recurred, both in women who took only FA in their next pregnancy. No adverse pregnancy events were associated with inositol supplementation. The findings of the PONTI pilot study encourage a large-scale controlled trial of inositol for NTD prevention, but indicate the need for a careful study design in view of the unwillingness of many high-risk women to be randomised.
[本文引用:1]
|
| [83] |
Hyperhomocysteinaemia has been identified as a risk factor for cerebrovascular, peripheral vascular and coronary heart disease. Elevated levels of plasma homocysteine can result from genetic or nutrient-related disturbances in the trans-sulphuration or re-methylation pathways for homocysteine metabolism. 5, 10-Methylenetetrahydrofolate reductase (MTHFR) catalyzes the reduction of 5, 10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, the predominant circulatory form of folate and carbon donor for the re-methylation of homocysteine to methionine. Reduced MTHFR activity with a thermolabile enzyme has been reported in patients with coronary and peripheral artery disease. We have identified a common mutation in MTHFR which alters a highly-conserved amino acid; the substitution occurs at a frequency of approximately 38% of unselected chromosomes. The mutation in the heterozygous or homozygous state correlates with reduced enzyme activity and increased thermolability in lymphocyte extracts; in vitro expression of a mutagenized cDNA containing the mutation confirms its effect on thermolability of MTHFR. Finally, individuals homozygous for the mutation have significantly elevated plasma homocysteine levels. This mutation in MTHFR may represent an important genetic risk factor in vascular disease.
[本文引用:1]
|
| [84] |
BACKGROUND: The methylenetetrahydrofolate reductase (MTHFR) genotype is associated with modification of disease and risk of neural tube defects. Plasma and red blood cell (RBC) folate and plasma homocysteine concentrations change in response to daily intakes of folic acid supplements, but no large-scale or population-based randomized trials have examined whether the MTHFR genotype modifies the observed response. OBJECTIVE: We sought to determine whether the MTHFR 677C-->T genotype modifies the response to folic acid supplementation during and 3 mo after discontinuation of supplementation. DESIGN: Northern Chinese women of childbearing age were enrolled in a 6-mo supplementation trial of different folic acid doses: 100, 400, and 4000 mug/d and 4000 mug/wk. Plasma and RBC folate and plasma homocysteine concentrations were measured at baseline; after 1, 3, and 6 mo of supplementation; and 3 mo after discontinuation of supplementation. MTHFR genotyping was performed to identify a C-->T mutation at position 677 (n = 932). RESULTS: Plasma and RBC folate and homocysteine concentrations were associated with MTHFR genotype throughout the supplementation trial, regardless of folic acid dose. MTHFR TT was associated with lower folate concentrations, and the trend of TT < CC was maintained at even the highest doses. Folic acid doses of 100 mug/d or 4000 mug/wk did not reduce high homocysteine concentrations in those with the MTHFR TT genotype. CONCLUSION: MTHFR genotype was an independent predictor of plasma and RBC folate and plasma homocysteine concentrations and did not have a significant interaction with folic acid dose during supplementation. This trial was registered at clinicaltrials.gov as NCT00207558.
[本文引用:1]
|
| [85] |
BACKGROUND: Increased total homocysteine (tHcy) may be associated with placental-mediated adverse pregnancy outcomes, but few prospective studies have measured tHcy before pregnancy outcome. This study was undertaken to determine whether increased tHcy measured in early pregnancy is associated with pregnancy loss, gestational hypertension (GH), preeclampsia, or small for gestational age (SGA) infants. METHODS: We conducted a prospective cohort study between 2002 and 2005. We measured tHcy and serum folate in blood samples from pregnant women (<20 weeks' gestation) and collected detailed pregnancy information through a questionnaire and medical record review. RESULTS: Of the 2119 women included in the study, 103 had a pregnancy loss, 115 had gestational hypertension, 65 had preeclampsia, and 129 had an SGA infant. Subjects with increased tHcy concentrations were at increased risk of pregnancy loss [relative risk (RR) 2.1, 95% CI 1.2-3.6] or preeclampsia (RR 2.7, 95% CI 1.4-5.0) than subjects with lower tHcy concentrations, but increased tHcy concentration was not associated with increased risk of developing GH or having an SGA infant. CONCLUSION: The finding of high tHcy in early pregnancy as a risk factor for pregnancy loss and preeclampsia is consistent with a hypothesis that increased tHcy results in abnormalities of the placental vasculature.
[本文引用:1]
|
| [86] |
OBJECTIVE: To determine the size of reduction in homocysteine concentrations produced by dietary supplementation with folic acid and with vitamins B-12 or B-6. DESIGN: Meta-analysis of randomised controlled trials that assessed the effects of folic acid based supplements on blood homocysteine concentrations. Multivariate regression analysis was used to determine the effects on homocysteine concentrations of different doses of folic acid and of the addition of vitamin B-12 or B-6. SUBJECTS: Individual data on 1114 people included in 12 trials. FINDINGS: The proportional and absolute reductions in blood homocysteine produced by folic acid supplements were greater at higher pretreatment blood homocysteine concentrations (P < 0.001) and at lower pretreatment blood folate concentrations (P < 0.001). After standardisation to pretreatment blood concentrations of homocysteine of 12 mumol/l and of folate of 12 nmol/l (approximate average concentrations for Western populations), dietary folic acid reduced blood homocysteine concentrations by 25% (95% confidence interval 23% to 28%; P < 0.001), with similar effects in the range of 0.5-5 mg folic acid daily. Vitamin B-12 (mean 0.5 mg daily) produced an additional 7% (3% to 10%) reduction in blood homocysteine. Vitamin B-6 (mean 16.5 mg daily) did not have a significant additional effect. CONCLUSIONS: Typically in Western populations, daily supplementation with both 0.5-5 mg folic acid and about 0.5 mg vitamin B-12 would be expected to reduce blood homocysteine concentrations by about a quarter to a third (for example, from about 12 mumol/l to 8-9 mumol/l). Large scale randomised trials of such regimens in high risk populations are now needed to determine whether lowering blood homocysteine concentrations reduces the risk of vascular disease.
[本文引用:1]
|
| [87] |
We analyzed the spectrum of neural-tube defects associated with maternal exposure to antiepileptic drugs (AEDs) and the possible contribution of familial and genetic factors to epilepsy or neural-tube defects. No specific association with maternal family history of neural-tube defects or epilepsy was seen. The ratio of spina bifida to anencephaly (33:1) suggested a specific association with caudal defects. Hydrocephaly was documented in at least 21 cases. Other midline defects, all associated with valproate (VPA), were hypospadias (two), hypertelorism (two), partial agenesis of corpus callosum, agenesis of septum pellucidum with lissencephaly of medial sides of occipital lobes, Dandy-Walker anomaly, and ventricular septal defect. This study shows that most neural-tube defects following maternal VPA use are severe open defects. They are frequently complicated by hydrocephaly and other midline defects. Prenatal diagnosis is possible.
[本文引用:1]
|
| [88] |
|
| [89] |
Intestinal folic acid transport is a saturable process with a pH optimum of 5.5 to 6.0. Because of the possible effects of antacids and acid-lowering drugs on the pH of the proximal small intestine, the influence of these drugs on folic acid absorption was studied by using tritium-labeled pteroylmonoglutamic acid (PGA) in 30 subjects (21 women, nine men) of 56 to 89 years of age. Both cimetidine and an antacid containing aluminum and magnesium hydroxide reduced folate absorption from a liquid formula meal (p less than 0.01, p less than 0.001, respectively). Although ranitidine also caused a fall in folic acid absorption from the liquid meal, the change was not statistically significantly different from when PGA was given with the meal alone. Both histamine receptor antagonists tended to maintain a high intraluminal pH in the proximal small intestine after meals, which in part could explain the inhibition of folate absorption. However, neither drug was found to chemically interact with folic acid, and neither drug inhibited the dihydrofolate reductase. The antacid was found to precipitate folic acid at a pH of greater than 4.0, thus removing it from the aqueous phase. This appears to be the explanation for the lowered folate absorption in the presence of antacid. Although the effects of these drugs on reducing folic acid absorption were relatively small, such reductions could become clinically significant in chronic antacid or H2 receptor antagonist use or intensive antacid or H2 receptor antagonist use by individuals eating diets that are marginal in folate content.
[本文引用:1]
|
| [90] |
|
| [91] |
Importance: Strategies to prevent autism in children exposed to antiepileptic drugs (AEDs) during pregnancy are important. Objective: To explore whether folic acid supplementation and folate status in pregnancy are associated with reduced risk of autistic traits owing to in utero AED exposure. Design, Setting, and Participants: The population-based, prospective Norwegian Mother and Child Cohort Study approached Norwegian-speaking women attending routine ultrasonographic examinations from June 1999 through December 31, 2008 (163844 of 277702 women refused). No exclusion criteria were applied beyond language. Questionnaires during and after pregnancy, analysis of blood samples, and linkage to the Medical Birth Registry of Norway were performed. Children aged 18 to 36 months of women with available information on use of AEDs and of folic acid supplementation (n = 104946) were included in the analysis from March 1, 2016, through June 13, 2017. Exposures: Maternal folic acid supplementation 4 weeks before to 12 weeks after conception. Plasma folate concentration was analyzed at gestational weeks 17 to 19. Main Outcomes and Measures: Autistic traits were evaluated using the Modified Checklist for Autism in Toddlers and Social Communication Questionnaire. Odds ratios (ORs) for autistic traits in children by maternal use vs nonuse of folic acid supplements were adjusted for maternal health and socioeconomic factors. Folate concentrations and folic acid doses were associated with the degree of autistic traits. Results: The overall mean (SD) age of the 104946 mothers of participating children was 29.8 (4.6) years, with complete information available for analysis in 103 868. Mean (SD) age of women with epilepsy who received AED treatment was 29.4 (4.9); women with epilepsy who did not receive AED treatment, 29.1 (4.9); and without epilepsy, 29.8 (4.6) years. In the 335 children exposed to AEDs, the risk for autistic traits was significantly higher at 18 months of age (adjusted OR [AOR], 5.9; 95% CI, 2.2-15.8) and 36 months of age (AOR, 7.9; 95% CI, 2.5-24.9) when their mothers had not used folic acid supplements compared with children of mothers who had used supplements. Among women without epilepsy, the corresponding risks were lower at 18 months of age (AOR, 1.3; 95% CI, 1.2-1.4) and 36 months of age (AOR, 1.7; 95% CI, 1.5-1.9); among the 389 children of women with untreated epilepsy, the corresponding risks were not significant at 18 months of age (AOR, 1.0; 95% CI, 0.4-3.0) and 36 months of age (AOR, 2.5; 95% CI, 0.4-16.6). Degree of autistic traits was inversely associated with maternal plasma folate concentrations (beta = -0.3; P = .03) and folic acid doses (beta = -0.5; P < .001). Concentrations of AEDs were not associated with the degree of autistic traits. Conclusions and Relevance: Risk of autistic traits in children exposed to AEDs in utero may be mitigated by periconceptional folic acid supplementation and folate status. Fertile women using AEDs should take folic acid supplements continuously.
[本文引用:1]
|
| [92] |
Background Many women of childbearing potential take antiepileptic drugs, but the cognitive effects of fetal exposure are uncertain. We aimed to assess effects of commonly used antiepilepfic drugs on cognitive outcomes in children up to 6 years of age.
[本文引用:1]
Methods In this prospective, observational, assessor-masked, multicentre study, we enrolled pregnant women with epilepsy on antiepileptic drug monotherapy (carbamazepine, lamotrigine, phenytoin, or valproate) between October, 1999, and February, 2004, at 25 epilepsy centres in the UK and the USA. Our primary outcome was intelligence quotient (IQ) at 6 years of age (age-6 IQ) in all children, assessed with linear regression adjusted for maternal IQ, antiepilepfic drug type, standardised dose, gestational birth age, and use of periconceptional folate. We also assessed multiple cognitive domains and compared findings with outcomes at younger ages. This study is registered with ClinicalTrials.gov, number NCT00021866. Findings We included 305 mothers and 311 children (six twin pairs) in the primary analysis. 224 children completed 6 years of follow-up (6-year-completer sample). Multivariate analysis of all children showed that age-6 IQ was lower after exposure to valproate (mean 97, 95% CI 94-101) than to carbamazepine (105, 102-108; p=0.0015), lamotrigine (108, 105-110; p=0.0003), or phenytoin (108, 104-112; p=0.0006). Children exposed to valproate did poorly on measures of verbal and memory abilities compared with those exposed to the other antiepileptic drugs and on non-verbal and executive functions compared with lamotrigine (but not carbamazepine or phenytoin). High doses of valproate were negatively associated with IQ (r=-0.56, p<0.0001), verbal ability (r=-0.40, p=0.0045), non-verbal ability (r=-0.42, p=0.0028), memory (r=-0.30, p=0.0434), and executive function (r=-0.42, p=0.0004), but other antiepileptic drugs were not. Age-6 IQ correlated with IQs at younger ages, and IQ improved with age for infants exposed to any antiepileptic drug. Compared with a normative sample (173 [93%] of 187 children), right-handedness was less frequent in children in our study overall (185 [86%] of 215; p=0.0404) and in the lamotrigine (59 [83%] of 71; p=0.0287) and valproate (38 [79%] of 40; p=0.0089) groups. Verbal abilities were worse than non-verbal abilities in children in our study overall and in the lamotrigine and valproate groups. Mean IQs were higher in children exposed to periconceptional folate (108, 95% CI 106-111) than they were in unexposed children (101, 98-104; p=0.0009). Interpretation Fetal valproate exposure has dose-dependent associations with reduced cognitive abilities across a range of domains at 6 years of age. Reduced right-handedness and verbal (vs non-verbal) abilities might be attributable to changes in cerebral lateralisation induced by exposure to antiepileptic drugs. The positive association of periconceptional folate with IQ is consistent with other recent studies. |
| [93] |
OBJECTIVE: To delineate the risk to child IQ associated with frequently prescribed antiepileptic drugs. METHODS: Children born to women with epilepsy (n = 243) and women without epilepsy (n = 287) were recruited during pregnancy and followed prospectively. Of these, 408 were blindly assessed at 6 years of age. Maternal and child demographics were collected and entered into statistical models. RESULTS: The adjusted mean IQ was 9.7 points lower (95% confidence interval [CI] -4.9 to -14.6; p < 0.001) for children exposed to high-dose (>800 mg daily) valproate, with a similar significant effect observed for the verbal, nonverbal, and spatial subscales. Children exposed to high-dose valproate had an 8-fold increased need of educational intervention relative to control children (adjusted relative risk, 95% CI 8.0, 2.5-19.7; p < 0.001). Valproate at doses <800 mg daily was not associated with reduced IQ, but was associated with impaired verbal abilities (-5.6, 95% CI -11.1 to -0.1; p = 0.04) and a 6-fold increase in educational intervention (95% CI 1.4-18.0; p = 0.01). In utero exposure to carbamazepine or lamotrigine did not have a significant effect on IQ, but carbamazepine was associated with reduced verbal abilities (-4.2, 95% CI -0.6 to -7.8; p = 0.02) and increased frequency of IQ <85. CONCLUSIONS: Consistent with data from younger cohorts, school-aged children exposed to valproate at maternal doses more than 800 mg daily continue to experience significantly poorer cognitive development than control children or children exposed to lamotrigine and carbamazepine.
[本文引用:1]
|
| [94] |
CONTEXT: Evidence suggests an association between maternal obesity and some congenital anomalies. OBJECTIVE: To assess current evidence of the association between maternal overweight, maternal obesity, and congenital anomaly. DATA SOURCES: MEDLINE, EMBASE, CINAHL, and Scopus (January 1966 through May 2008) were searched for English-language studies using a list of keywords. Reference lists from relevant review articles were also searched. STUDY SELECTION: Observational studies with an estimate of prepregnancy or early pregnancy weight or body mass index (BMI) and data on congenital anomalies were considered. Of 1944 potential articles, 39 were included in the systematic review and 18 in the meta-analysis. Data Extraction and Synthesis Information was extracted on study design, quality, participants, congenital anomaly groups and subtypes, and risk estimates. Pooled odds ratios (ORs) comparing risk among overweight, obese, and recommended-weight mothers (defined by BMI) were determined for congenital anomaly groups and subtypes for which at least 150 cases had been reported in the literature. RESULTS: Pooled ORs for overweight and obesity were calculated for 16 and 15 anomaly groups or subtypes, respectively. Compared with mothers of recommended BMI, obese mothers were at increased odds of pregnancies affected by neural tube defects (OR, 1.87; 95% confidence interval [CI], 1.62-2.15), spina bifida (OR, 2.24; 95% CI, 1.86-2.69), cardiovascular anomalies (OR, 1.30; 95% CI, 1.12-1.51), septal anomalies (OR, 1.20; 95% CI, 1.09-1.31), cleft palate (OR, 1.23; 95% CI, 1.03-1.47), cleft lip and palate (OR, 1.20; 95% CI, 1.03-1.40), anorectal atresia (OR, 1.48; 95% CI, 1.12-1.97), hydrocephaly (OR, 1.68; 95% CI, 1.19-2.36), and limb reduction anomalies (OR, 1.34; 95% CI, 1.03-1.73). The risk of gastroschisis among obese mothers was significantly reduced (OR, 0.17; 95% CI, 0.10-0.30). CONCLUSIONS: Maternal obesity is associated with an increased risk of a range of structural anomalies, although the absolute increase is likely to be small. Further studies are needed to confirm whether maternal overweight is also implicated.
[本文引用:1]
|
| [95] |
|
| [96] |
BACKGROUND: Maternal pregestational diabetes is a well-known risk factor for congenital anomalies. This study analyses the spectrum of congenital anomalies associated with maternal diabetes using data from a large European database for the population-based surveillance of congenital anomalies. METHODS: Data from 18 population-based EUROCAT registries of congenital anomalies in 1990-2005. All malformed cases occurring to mothers with pregestational diabetes (diabetes cases) were compared to all malformed cases in the same registry areas to mothers without diabetes (non-diabetes cases). RESULTS: There were 669 diabetes cases and 92,976 non diabetes cases. Odds ratios in diabetes pregnancies relative to non-diabetes pregnancies comparing each EUROCAT subgroup to all other non-chromosomal anomalies combined showed significantly increased odds ratios for neural tube defects (anencephaly and encephalocele, but not spina bifida) and several subgroups of congenital heart defects. Other subgroups with significantly increased odds ratios were anotia, omphalocele and bilateral renal agenesis. Frequency of hip dislocation was significantly lower among diabetes (odds ratio 0.15, 95% CI 0.05-0.39) than non-diabetes cases. Multiple congenital anomalies were present in 13.6 % of diabetes cases and 6.1 % of non-diabetes cases. The odds ratio for caudal regression sequence was very high (26.40,95% CI 8.98-77.64), but only 17% of all caudal regression cases resulted from a pregnancy with pregestational diabetes. CONCLUSIONS: The increased risk of congenital anomalies in pregnancies with pregestational diabetes is related to specific non-chromosomal congenital anomalies and multiple congenital anomalies and not a general increased risk.
[本文引用:1]
|
| [97] |
|
| [98] |
BACKGROUND: Maternal folic acid (FA) protects against developmental toxicity from certain environmental chemicals. OBJECTIVE: We examined combined exposures to maternal FA and pesticides in relation to autism spectrum disorder (ASD). METHODS: Participants were California children born from 2000-2007 who were enrolled in the Childhood Autism Risks from Genetics and the Environment (CHARGE) case-control study at age 2-5 y, were clinically confirmed to have ASD (n=296) or typical development (n=220), and had information on maternal supplemental FA and pesticide exposures. Maternal supplemental FA and household pesticide product use were retrospectively collected in telephone interviews from 2003-2011. High vs. low daily FA intake was dichotomized at 800mug (median). Mothers' addresses were linked to a statewide database of commercial applications to estimate agricultural pesticide exposure. RESULTS: High FA intake (>/=800mug) during the first pregnancy month and no known pesticide exposure was the reference group for all analyses. Compared with this group, ASD was increased in association with <800mug FA and any indoor pesticide exposure {adjusted odds ratio [OR]=2.5 [95% confidence interval (CI): 1.3, 4.7]} compared with low FA [OR=1.2 (95% CI: 0.7, 2.2)] or indoor pesticides [OR=1.7 (95% CI: 1.1, 2.8)] alone. ORs for the combination of low FA and regular pregnancy exposure (>/=6 mo) to pet pesticides or to outdoor sprays and foggers were 3.9 (95% CI: 1.4, 11.5) and 4.1 (95% CI: 1.7, 10.1), respectively. ORs for low maternal FA and agricultural pesticide exposure 3 mo before or after conception were 2.2 (95% CI: 0.7, 6.5) for chlorpyrifos, 2.3 (95% CI: 0.98, 5.3) for organophosphates, 2.1 (95% CI: 0.9, 4.8) for pyrethroids, and 1.5 (95% CI: 0.5, 4.8) for carbamates. Except for carbamates, these ORs were approximately two times greater than those for either exposure alone or for the expected ORs for combined exposures under multiplicative or additive models. CONCLUSIONS: In this study population, associations between pesticide exposures and ASD were attenuated among those with high versus low FA intake during the first month of pregnancy. Confirmatory and mechanistic studies are needed. https://doi.org/10.1289/EHP604.
[本文引用:1]
|
| [99] |
BACKGROUND: Hypertensive disorders of pregnancy are among the leading causes of maternal morbidity and mortality. Studies suggest that the use of folic acid may lower the risk of hypertensive disorders in pregnant women. AIM: The aim of this study was to assess the effects of timing and duration of folic acid-containing supplement use on the risk for gestational hypertension and preeclampsia. METHODS: Exposures and outcomes data were obtained through interviews and review of participant's medical records from the MotherToBaby cohort studies across the United States and Canada. Demographics, medical history, lifestyle factors, substance use, and fetal sex were assessed as potential confounders. Unadjusted and adjusted risks for gestational hypertension and preeclampsia were examined using odds ratios and 95% confidence intervals. FINDINGS: 3247 women were included in the study. Compared to non-supplement use, early and late supplement use were not significantly associated with the development of gestational hypertension or preeclampsia. The odds of developing gestational hypertension and preeclampsia were significantly reduced as the duration of folic acid-containing supplement use increased. CONCLUSION: Findings from this study suggest that the use of folic acid-containing supplements may mitigate the risk for gestational hypertension and preeclampsia.
[本文引用:1]
|
| [100] |
|
| [101] |
The influence of folate nutritional status on various pregnancy outcomes has long been recognized. Studies conducted in the 1950s and 1960s led to the recognition of prenatal folic acid supplementation as a means to prevent pregnancy-induced megaloblastic anemia. In the 1990s, the utility of periconceptional folic acid supplementation and folic acid food fortification emerged when they were proven to prevent the occurrence of neural tube defects. These distinctively different uses of folic acid may well be ranked among the most significant public health measures for the prevention of pregnancy-related disorders. Folate is now viewed not only as a nutrient needed to prevent megaloblastic anemia in pregnancy but also as a vitamin essential for reproductive health. This review focuses on the relation between various outcomes of human reproduction (ie, pregnancy, lactation, and male reproduction) and folate nutrition and metabolism, homocysteine metabolism, and polymorphisms of genes that encode folate-related enzymes or proteins, and we identify issues for future research.
[本文引用:1]
|
| [102] |
|
| [103] |
Many women are advised to consume a folic acid-containing prenatal supplement for the duration of pregnancy and lactation. Whether this remains necessary after folic acid fortification of the food supply in North America has yet to be determined. Our objective was to assess the dietary folate intake of a sample of pregnant and lactating women at mandated and predicted folic acid-fortification levels and determine the prevalence of inadequate and excessive intakes. Weighed food records (for 3 d) were collected from predominantly university-educated women (32 +/- 4 y of age) at 36 wk of pregnancy (n = 61) and at 4 and 16 wk of lactation (n = 60). Dietary folate intakes during pregnancy and lactation, assuming fortification at mandated levels (140-150 micro g/100 g), were 562 +/- 106 and 498 +/- 99 micro g/d dietary folate equivalents (DFE), respectively. The prevalence of inadequacy for folate, or the proportion of individuals with usual folate intakes less than their nutrient requirement, was 36% for women during pregnancy (estimated average requirement of 520 micro g/d DFE), and 32% during lactation (estimated average requirement of 450 micro g/d DFE). Assuming fortification at twice the mandated level, mean dietary intakes during pregnancy and lactation were 786 +/- 132 and 716 +/- 150 micro g/d DFE, respectively, producing only a 3% prevalence of folate inadequacy. Grains contributed approximately 41% of total folate intake followed by fruits and vegetables (approximately 21%). To conclude, at mandated levels of fortification many pregnant and lactating women are unlikely to meet their folate requirements from dietary sources alone; however, the actual level of inadequacy cannot be determined until the level of folic acid in the food supply is known with greater precision.
[本文引用:1]
|
| [104] |
Folate is a B-vitamin with particular importance during reproduction due to its role in the synthesis and maintenance of DNA. Folate is well known for its role in preventing neural tube defects (NTDs) during the periconceptional period. There is also an increased need for folate throughout pregnancy to support optimal growth and development of the fetus and blood volume expansion and tissue growth of the mother. During lactation, women are at risk of folate deficiency due to increased demands to accommodate milk folate levels. Nutrient Intake Values (NIVs) for folate have been calculated to take into account additional needs during pregnancy and lactation. However, these values vary widely between countries. For example, the folate requirement that is set to meet the needs of almost all healthy women during pregnancy varies from 300 mu g/day in the United Kingdom to 750 mu g/day in Mexico. Currently, there is no accepted standardized terminology or framework for establishing NIVs. This article reviews country-specific NIVs for folate during pregnancy and lactation and the basis for setting these reference values.
DOI:10.3390/nu5103920
URL
[本文引用:2]
|
| [105] |
BACKGROUND: Folate requirements during lactation are not well established. OBJECTIVE: We assessed the effects of dietary and supplemental folate intakes during extended lactation. DESIGN: Lactating women (n = 42) were enrolled in a double-blind, randomized, longitudinal supplementation trial and received either 0 or 1 mg folic acid/d. At 3 and 6 mo postpartum, maternal folate status was assessed by measuring erythrocyte, plasma, milk, and dietary folate concentrations; plasma homocysteine; and hematologic indexes. Infant anthropometric measures of growth, milk intake, and folate intake were also assessed. RESULTS: In supplemented women, values at 6 mo for erythrocyte and milk folate concentrations and for plasma homocysteine were not significantly different from those at 3 mo. In supplemented women compared with unsupplemented women at 6 mo, values for erythrocyte folate (840 compared with 667 nmol/L; P < 0.05), hemoglobin (140 compared with 134 g/L; P < 0.02), and hematocrit (0.41 compared with 0.39; P < 0.02) were higher and values for reticulocytes were lower. In unsupplemented women, milk folate declined from 224 to 187 nmol/L (99 to 82 ng/mL), whereas plasma homocysteine increased from 6.7 to 7.4 micromol/L. Dietary folate intake was not significantly different between groups (380+/-19 microg/d) and at 6 mo was correlated with plasma homocysteine in unsupplemented women (r = -0.53, P < 0.01) and with plasma folate in supplemented women (r = 0.49, P < 0.02). CONCLUSIONS: A dietary folate intake of approximately 380 microg/d may not be sufficient to prevent mobilization of maternal folate stores during lactation.
[本文引用:2]
|
| [106] |
|
| [107] |
|
| [108] |
|
| [109] |
Background: Coronary artery disease (CAD) still represents the major cause of mortality in developed countries. Large research programs have been focused on the identification of new risk factors to prevent CAD, with special attention to homocysteine (Hcy), due to the known associated increased thrombogenicity, oxidative stress status and endothelial dysfunction. However, controversy still exists on the association between Hcy and CAD. Therefore, aim of the current study was to investigate the association of Hcy with the prevalence and extent of CAD in a large consecutive cohort of patients undergoing coronary angiography.
[本文引用:1]
Methods: Our population is represented by a total of 3056 consecutive patients undergoing coronary angiography between at the Azienda Ospedaliera "Maggiore della Carita", Novara, Italy. Fasting samples were collected for homocysteine levels assessment. Coronary disease was defined for at least 1 vessel stenosis > 50% as evaluated by QCA. Results: Study population was divided according to Hcy tertiles (<13,3, 13,3-18.2, >18.2 nmol/ml). High plasmatic level of homocysteine was related with age (p < 0.001), male gender (p < 0.001), hypertension (p < 0.001) renal failure (p < 0.001), family history of CAD (p < 0.001), previous cerebrovascular accident (p < 0.001), previous MI (p = 0.002), previous CABG (p = 0.003), ejection fraction (p < 0.001), higher baseline creatinine (p < 0.001), in treatment with nitrates (p < 0.001), calcium antagonists (p < 0.001), diuretics (p < 0.001), Ace inhibitors (ACE-I) (p = 0.006), Clopidogrel (p = 0.05), haemoglobin (p = 0.001), white blood cells (WBC) count (p = 0.008), total cholesterol (p = 0.04), Low-Density Lipoproteins (LDL) (p = 0.01). A significant relationship was found between Hcy levels and the extent of coronary artery disease (71.8% vs 77.8% vs 77.4%, OR[95% CI] = 1.18[1.11-1.252.], p < 0.001 and severe CAD (23.6% vs 29.5% vs 32.1%, OR [95% CI] = 1.275 [1.209-1.344], p < 0.001). Elevated Hcy was significantly associated with increased risk of CAD (adjusted OR [95% CI] = 1.087[1.009-1.171], p = 0.02 and severe CAD (adjusted OR [95% CI] = 1.07 [1.01-1.16, P = 0.04]). The results were confirmed in the majority of high risk subsets of patients. Conclusions: This study showed that high levels of plasmatic Hcy are independently associated with CAD. Further large studies are certainly needed to explore the adjunctive benefits from vitamin administration in patients with elevated Hcy to prevent the occurrence and progression of CAD. (C) 2014 Elsevier Ltd. |
| [110] |
Background While elevated homocysteine has been associated with calcification in several studies, its importance as a cardiovascular risk factor remains unclear. This study examines the relationship between homocysteine and vascular and valve calcification in the MESA (Multi-ethnic Study of Atherosclerosis) cohort. Methods and Results MESA participants with baseline homocysteine measurements and cardiac computed tomography scans were included (N=6789). Baseline and follow-up assessment of vascular (coronary artery [CAC], descending thoracic aorta [DTAC]) and valve (aortic valve [AVC], mitral annular [MAC]) calcification was performed. Prevalence ratio/relative risk regression was used to assess the relationship of homocysteine with prevalent and incident calcification, and multivariable logistic regression was used to assess associations between homocysteine and calcification progression. Elevated homocysteine was associated with greater relative risk of prevalent and incident CAC and incident DTAC. We also identified a strong association between elevated homocysteine and CAC and DTAC progression. Elevated homocysteine was found to confer a >2-fold increased risk of severe CAC progression (defined as DeltaCAC >/=100/year) and an approximately 1.5-fold increased risk for severe DTAC progression (defined as DeltaDTAC >/=100/year). Conclusions To our knowledge, this is the first study demonstrating an association between elevated homocysteine and both incidence and progression of coronary and extra-coronary vascular calcification. Our findings suggest a potential role for elevated homocysteine as a risk factor for severe vascular calcification progression. Future studies are warranted to further assess the utility of homocysteine as a biomarker for vascular calcification incidence and progression. Clinical Trial Registration https://www.clinicaltrials.gov/. Unique identifier: NCT00005487.
[本文引用:1]
|
| [111] |
CONTEXT: It has been suggested that total blood homocysteine concentrations are associated with the risk of ischemic heart disease (IHD) and stroke. OBJECTIVE: To assess the relationship of homocysteine concentrations with vascular disease risk. DATA SOURCES: MEDLINE was searched for articles published from January 1966 to January 1999. Relevant studies were identified by systematic searches of the literature for all reported observational studies of associations between IHD or stroke risk and homocysteine concentrations. Additional studies were identified by a hand search of references of original articles or review articles and by personal communication with relevant investigators. STUDY SELECTION: Studies were included if they had data available by January 1999 on total blood homocysteine concentrations, sex, and age at event. Studies were excluded if they measured only blood concentrations of free homocysteine or of homocysteine after a methionine-loading test or if relevant clinical data were unavailable or incomplete. DATA EXTRACTION: Data from 30 prospective or retrospective studies involving a total of 5073 IHD events and 1113 stroke events were included in a meta-analysis of individual participant data, with allowance made for differences between studies, for confounding by known cardiovascular risk factors, and for regression dilution bias. Combined odds ratios (ORs) for the association of IHD and stroke with blood homocysteine concentrations were obtained by using conditional logistic regression. DATA SYNTHESIS: Stronger associations were observed in retrospective studies of homocysteine measured in blood collected after the onset of disease than in prospective studies among individuals who had no history of cardiovascular disease when blood was collected. After adjustment for known cardiovascular risk factors and regression dilution bias in the prospective studies, a 25% lower usual (corrected for regression dilution bias) homocysteine level (about 3 micromol/L [0.41 mg/L]) was associated with an 11% (OR, 0.89; 95% confidence interval [CI], 0.83-0.96) lower IHD risk and 19% (OR, 0.81; 95% CI, 0.69-0.95) lower stroke risk. CONCLUSIONS: This meta-analysis of observational studies suggests that elevated homocysteine is at most a modest independent predictor of IHD and stroke risk in healthy populations. Studies of the impact on disease risk of genetic variants that affect blood homocysteine concentrations will help determine whether homocysteine is causally related to vascular disease, as may large randomized trials of the effects on IHD and stroke of vitamin supplementation to lower blood homocysteine concentrations.
[本文引用:2]
|
| [112] |
Background Arterial stiffness and homocysteine are both powerful predictors of cardiovascular disease, especially in older populations. Previous studies have investigated the association of homocysteine with arterial stiffness in human subjects, while the relationship between homocysteine and arterial stiffness in the elderly is still indefinite. The current study examined the association of homocysteine with arterial stiffness in Chinese community-based elderly persons.
[本文引用:2]
Methods We related serum levels of homocysteine to two measures of arterial stiffness (carotid-femoral pulse wave velocity (PWV) and carotid-radial PWV) in 780 participants (46.3% men, mean age 71.9 years (ranging 65-96 years old)) from two communities of Beijing, China. Arterial stiffness were measured within two days of the time of biomarker measurement. Results In multiple-adjusted models, homocysteine levels was strongly associated with the carotid-femoral PWV (standardized beta = 0.13, P < 0.001), even after adjustment for classical risk factors of cardiovascular disease. The association is also stronger when the carotid-femoral PWV is elevated above normal, whereas no significant association with homocysteine was observed for carotid- radial PWV. Conclusions In Chinese elderly persons, serum homocysteine levels are associated with alterations of aortic stiffness. |
| [113] |
|
| [114] |
BACKGROUND: Hyperhomocyst(e)inemia is a risk factor for atherosclerosis and is prevalent in the elderly. The objective of this study was to determine whether hyperhomocyst(e)inemia is associated with impaired endothelium-dependent vasodilation in humans. METHODS AND RESULTS: High-resolution vascular ultrasonography was used to study endothelium-dependent and -independent vasodilation in a nonatherosclerotic peripheral conduit artery of 26 elderly hyperhomocyst(e)inemic subjects and 15 age- and sex-matched subjects with normal homocysteine levels. Flow-mediated, endothelium-dependent (nitric oxide-mediated) vasodilation was assessed by measuring the percent change in brachial artery diameter during reactive hyperemia. Endothelium-independent vasodilation was assessed after the administration of 0.4 mg sublingual nitroglycerin. Endothelium-dependent vasodilation was significantly impaired in the hyperhomocyst(e)inemic subjects compared with control subjects (3.7 +/- 0.6% versus 8.1 +/- 1.2%; P = .004), whereas endothelium-independent vasodilation was not different between the two groups (10.1 +/- 1.6% versus 9.3 +/- 1.5%; P = NS). In a linear regression analysis with serum homocysteine concentration, folic acid, age, sex, cholesterol (serum total, LDL, or HDL cholesterol), mean arterial blood pressure, use of antihypertensive medication, and baseline brachial artery diameter included as covariates, serum homocysteine concentration emerged as the only significant predictor of flow-mediated vasodilation. CONCLUSIONS: These data indicate that hyperhomocyst(e)inemia is associated with impaired endothelium-dependent vasodilation in humans and suggest that the bioavailability of nitric oxide is decreased in hyperhomocyst(e)inemic humans.
[本文引用:1]
|
| [115] |
OBJECTIVE: To assess whether the association of serum homocysteine concentration with ischaemic heart disease, deep vein thrombosis and pulmonary embolism, and stroke is causal and, if so, to quantify the effect of homocysteine reduction in preventing them. DESIGN: Meta-analyses of the above three diseases using (a) 72 studies in which the prevalence of a mutation in the MTHFR gene (which increases homocysteine) was determined in cases (n=16 849) and controls, and (b) 20 prospective studies (3820 participants) of serum homocysteine and disease risk. MAIN OUTCOME MEASURES: Odds ratios of the three diseases for a 5 micromol/l increase in serum homocysteine concentration. RESULTS: There were significant associations between homocysteine and the three diseases. The odds ratios for a 5 micromol/l increase in serum homocysteine were, for ischaemic heart disease, 1.42 (95% confidence interval 1.11 to 1.84) in the genetic studies and 1.32 (1.19 to 1.45) in the prospective studies; for deep vein thrombosis with or without pulmonary embolism, 1.60 (1.15 to 2.22) in the genetic studies (there were no prospective studies); and, for stroke, 1.65 (0.66 to 4.13) in the genetic studies and 1.59 (1.29 to 1.96) in the prospective studies. CONCLUSIONS: The genetic studies and the prospective studies do not share the same potential sources of error, but both yield similar highly significant results-strong evidence that the association between homocysteine and cardiovascular disease is causal. On this basis, lowering homocysteine concentrations by 3 micromol/l from current levels (achievable by increasing folic acid intake) would reduce the risk of ischaemic heart disease by 16% (11% to 20%), deep vein thrombosis by 25% (8% to 38%), and stroke by 24% (15% to 33%).
[本文引用:1]
|
| [116] |
|
| [117] |
Homocystinuria, an abnormality of methionine metabolism is associated with severe vascular disease in infancy and childhood. Homocysteine is formed during the metabolism of methionine and accumulations of this and of cysteine-homocysteine mixed disulfide in the plasma indicate a partial block in the methionine degradation pathway. Methionine metabolism was investigated in 25 patients aged under 50 with angiographically proved coronary artery disease and in 22 control patients, of whom 17 had normal coronary arteries at angiography and 5 were healthy volunteers. After an overnight fast, venous blood was drawn before and 4 h after oral L-methionine, 100 mg/kg. Plasma methionine levels at 4 h were not different in the two groups, but there were significant differences in the levels of cysteine-homocysteine mixed disulfide. This was detected in 5 of 22 in the noncoronary group and in higher concentration in 17 of 25 coronary patients (P less than 0-01). Age, weight, height, body-mass index, glucose tolerance, fasting serum urate, and triglycerides were not different, but serum cholesterol was higher in the coronary patients (P lessthan 0.01). These results suggest a reduced ability to metabolise homocysteine in some patients with premature coronary artery disease when this pathway is stressed.
[本文引用:1]
|
| [118] |
BACKGROUND AND PURPOSE: The association of dietary folate and B vitamin intakes with risk of cardiovascular disease is controversial, and the evidence in Asian populations is limited. METHODS: A total of 23 119 men and 35 611 women, age 40 to 79 years, completed a food frequency questionnaire in the Japan Collaborative Cohort Study. During the median 14-year follow-up, there were 986 deaths from stroke, 424 from coronary heart disease, and 2087 from cardiovascular disease. RESULTS: Dietary folate and vitamin B(6) intakes were inversely associated with mortality from heart failure for men and with mortality from stroke, coronary heart disease, and total cardiovascular disease for women. These inverse associations did not change materially after adjustment for cardiovascular risk factors. No association was found between vitamin B(12) intake and mortality risk. CONCLUSIONS: High dietary intakes of folate and vitamin B(6) were associated with reduced risk of mortality from stroke, coronary heart disease, and heart failure among Japanese.
[本文引用:1]
|
| [119] |
BACKGROUND AND AIMS: Epidemiologic studies are inconsistent regarding the association between folate and coronary heart disease (CHD) risk. The aim was to perform a meta-analysis to determine whether an association exists between folate and total CHD endpoints in prospective studies. METHODS AND RESULTS: We searched the PUBMED and EMBASE databases for studies conducted from 1966 through August 2010. Data were independently abstracted by 2 investigators using a standardized protocol. Study-specific risk estimates were combined by using a random effects model. A total of 14 studies were included in the meta-analysis: 7 studies on dietary folate intake and 8 studies on blood folate levels. For dietary intake, the summary relative risk (RR) indicated a significant association between the highest folate intake and reduced risk of CHD (summary RR: 0.69; 95% CI: 0.60, 0.80). Furthermore, an increase in folate intake of 200 ug/day was associated with a 12% decrease in the risk of developing CHD (summary RR: 0.88; 95% CI: 0.82, 0.94). For blood folate levels, we also found a borderline inverse association of highest blood folate levels on CHD risk (summary RR: 0.74; 95% CI: 0.53, 1.02); our dose-response analysis indicated that an increment in blood folate levels of 5 mmol/l was associated with an 8% decrease in the risk of developing CHD (summary RR: 0.92; 95% CI: 0.84, 1.00). CONCLUSION: This meta-analysis suggests that dietary folate intake and blood folate level are inversely associated with CHD risk.
[本文引用:1]
|
| [120] |
CONTEXT: In observational studies, elevated plasma total homocysteine levels have been positively associated with ischemic stroke risk. However the utility of homocysteine-lowering therapy to reduce that risk has not been confirmed by randomized trials. OBJECTIVE: To determine whether high doses of folic acid, pyridoxine (vitamin B6), and cobalamin (vitamin B12), given to lower total homocysteine levels, reduce the risk of recurrent stroke over a 2-year period compared with low doses of these vitamins. DESIGN: Double-blind randomized controlled trial (September 1996-May 2003). SETTING AND PARTICIPANTS: 3680 adults with nondisabling cerebral infarction at 56 university-affiliated hospitals, community hospitals, private neurology practices, and Veterans Affairs medical centers across the United States, Canada, and Scotland. INTERVENTIONS: All participants received best medical and surgical care plus a daily multivitamin containing the US Food and Drug Administration's reference daily intakes of other vitamins; patients were randomly assigned to receive once-daily doses of the high-dose formulation (n = 1827), containing 25 mg of pyridoxine, 0.4 mg of cobalamin, and 2.5 mg of folic acid; or the low-dose formulation (n = 1853), containing 200 microg of pyridoxine, 6 microg of cobalamin and 20 microg of folic acid. MAIN OUTCOME MEASURES: Recurrent cerebral infarction (primary outcome); coronary heart disease (CHD) events and death (secondary outcomes). RESULTS: Mean reduction of total homocysteine was 2 micromol/L greater in the high-dose group than in the low-dose group, but there was no treatment effect on any end point. The unadjusted risk ratio for any stroke, CHD event, or death was 1.0 (95% confidence interval [CI], 0.8-1.1), with chances of an event within 2 years of 18.0% in the high-dose group and 18.6% in the low-dose group. The risk of ischemic stroke within 2 years was 9.2% for the high-dose and 8.8% for the low-dose groups (risk ratio, 1.0; 95% CI, 0.8-1.3) (P =.80 by log-rank test of the primary hypothesis of difference in ischemic stroke between treatment groups). There was a persistent and graded association between baseline total homocysteine level and outcomes. A 3- micromol/L lower total homocysteine level was associated with a 10% lower risk of stroke (P =.05), a 26% lower risk of CHD events (P<.001), and a 16% lower risk of death (P =.001) in the low-dose group and a nonsignificantly lower risk in the high-dose group by 2% for stroke, 7% for CHD events, and 7% for death. CONCLUSIONS: In this trial, moderate reduction of total homocysteine after nondisabling cerebral infarction had no effect on vascular outcomes during the 2 years of follow-up. However, the consistent findings of an association of total homocysteine with vascular risk suggests that further exploration of the hypothesis is warranted and longer trials in different populations with elevated total homocysteine may be necessary.
[本文引用:1]
|
| [121] |
BACKGROUND: In observational studies, lower homocysteine levels are associated with lower rates of coronary heart disease and stroke. Folic acid and vitamins B6 and B12 lower homocysteine levels. We assessed whether supplementation reduced the risk of major cardiovascular events in patients with vascular disease. METHODS: We randomly assigned 5522 patients 55 years of age or older who had vascular disease or diabetes to daily treatment either with the combination of 2.5 mg of folic acid, 50 mg of vitamin B6, and 1 mg of vitamin B12 or with placebo for an average of five years. The primary outcome was a composite of death from cardiovascular causes, myocardial infarction, and stroke. RESULTS: Mean plasma homocysteine levels decreased by 2.4 micromol per liter (0.3 mg per liter) in the active-treatment group and increased by 0.8 micromol per liter (0.1 mg per liter) in the placebo group. Primary outcome events occurred in 519 patients (18.8 percent) assigned to active therapy and 547 (19.8 percent) assigned to placebo (relative risk, 0.95; 95 percent confidence interval, 0.84 to 1.07; P=0.41). As compared with placebo, active treatment did not significantly decrease the risk of death from cardiovascular causes (relative risk, 0.96; 95 percent confidence interval, 0.81 to 1.13), myocardial infarction (relative risk, 0.98; 95 percent confidence interval, 0.85 to 1.14), or any of the secondary outcomes. Fewer patients assigned to active treatment than to placebo had a stroke (relative risk, 0.75; 95 percent confidence interval, 0.59 to 0.97). More patients in the active-treatment group were hospitalized for unstable angina (relative risk, 1.24; 95 percent confidence interval, 1.04 to 1.49). CONCLUSIONS: Supplements combining folic acid and vitamins B6 and B12 did not reduce the risk of major cardiovascular events in patients with vascular disease. (ClinicalTrials.gov number, NCT00106886; Current Controlled Trials number, ISRCTN14017017.).
[本文引用:2]
|
| [122] |
BACKGROUND: Homocysteine is a risk factor for cardiovascular disease. We evaluated the efficacy of homocysteine-lowering treatment with B vitamins for secondary prevention in patients who had had an acute myocardial infarction. METHODS: The trial included 3749 men and women who had had an acute myocardial infarction within seven days before randomization. Patients were randomly assigned, in a two-by-two factorial design, to receive one of the following four daily treatments: 0.8 mg of folic acid, 0.4 mg of vitamin B12, and 40 mg of vitamin B6; 0.8 mg of folic acid and 0.4 mg of vitamin B12; 40 mg of vitamin B6; or placebo. The primary end point during a median follow-up of 40 months was a composite of recurrent myocardial infarction, stroke, and sudden death attributed to coronary artery disease. RESULTS: The mean total homocysteine level was lowered by 27 percent among patients given folic acid plus vitamin B12, but such treatment had no significant effect on the primary end point (risk ratio, 1.08; 95 percent confidence interval, 0.93 to 1.25; P=0.31). Also, treatment with vitamin B6 was not associated with any significant benefit with regard to the primary end point (relative risk of the primary end point, 1.14; 95 percent confidence interval, 0.98 to 1.32; P=0.09). In the group given folic acid, vitamin B12, and vitamin B6, there was a trend toward an increased risk (relative risk, 1.22; 95 percent confidence interval, 1.00 to 1.50; P=0.05). CONCLUSIONS: Treatment with B vitamins did not lower the risk of recurrent cardiovascular disease after acute myocardial infarction. A harmful effect from combined B vitamin treatment was suggested. Such treatment should therefore not be recommended. (ClinicalTrials.gov number, NCT00266487.).
[本文引用:2]
|
| [123] |
CONTEXT: Blood homocysteine levels are positively associated with cardiovascular disease, but it is uncertain whether the association is causal. OBJECTIVE: To assess the effects of reducing homocysteine levels with folic acid and vitamin B(12) on vascular and nonvascular outcomes. DESIGN, SETTING, AND PATIENTS: Double-blind randomized controlled trial of 12,064 survivors of myocardial infarction in secondary care hospitals in the United Kingdom between 1998 and 2008. INTERVENTIONS: 2 mg folic acid plus 1 mg vitamin B(12) daily vs matching placebo. MAIN OUTCOME MEASURES: First major vascular event, defined as major coronary event (coronary death, myocardial infarction, or coronary revascularization), fatal or nonfatal stroke, or noncoronary revascularization. RESULTS: Allocation to the study vitamins reduced homocysteine by a mean of 3.8 micromol/L (28%). During 6.7 years of follow-up, major vascular events occurred in 1537 of 6033 participants (25.5%) allocated folic acid plus vitamin B(12) vs 1493 of 6031 participants (24.8%) allocated placebo (risk ratio [RR], 1.04; 95% confidence interval [CI], 0.97-1.12; P = .28). There were no apparent effects on major coronary events (vitamins, 1229 [20.4%], vs placebo, 1185 [19.6%]; RR, 1.05; 95% CI, 0.97-1.13), stroke (vitamins, 269 [4.5%], vs placebo, 265 [4.4%]; RR, 1.02; 95% CI, 0.86-1.21), or noncoronary revascularizations (vitamins, 178 [3.0%], vs placebo, 152 [2.5%]; RR, 1.18; 95% CI, 0.95-1.46). Nor were there significant differences in the numbers of deaths attributed to vascular causes (vitamins, 578 [9.6%], vs placebo, 559 [9.3%]) or nonvascular causes (vitamins, 405 [6.7%], vs placebo, 392 [6.5%]) or in the incidence of any cancer (vitamins, 678 [11.2%], vs placebo, 639 [10.6%]). CONCLUSION: Substantial long-term reductions in blood homocysteine levels with folic acid and vitamin B(12) supplementation did not have beneficial effects on vascular outcomes but were also not associated with adverse effects on cancer incidence. TRIAL REGISTRATION: isrctn.org Identifier: ISRCTN74348595.
[本文引用:2]
|
| [124] |
BACKGROUND AND OBJECTIVES: The efficacy of folic acid therapy to lower homocysteine (Hcy) levels in an effort to reduce cardiovascular disease (CVD) risk in patients with ESRD or advanced chronic kidney disease (ACKD; creatinine clearance, <30 ml/min) remains inconclusive. We conducted a meta-analysis of relevant randomized trials to further examine this issue. DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: This meta-analysis included 3886 patients with ESRD/ACKD from seven qualified randomized trials using folic acid therapy and with CVD reported as one of the end points. RESULTS: When pooling the seven trials, folic acid therapy reduced the risk of CVD by 15% (RR, 0.85; 95% CI, 0.76 to 0.96; P = 0.009). A greater beneficial effect was observed among those trials with a treatment duration >24 months (RR, 0.84; 95% CI, 0.72 to 0.98; P = 0.02), a decrease in Hcy level >20% (RR, 0.83; 95% CI, 0.73 to 0.95; P = 0.007), and no or partial folic acid fortification (RR, 0.80; 95% CI, 0.65 to 0.99; P = 0.04). The beneficial effect also was seen when Hcy levels decreased >20%, even in the presence of folic acid fortification (RR, 0.85; 95% CI, 0.73 to 0.99; P = 0.04). In the corresponding comparison groups, the estimated RRs were attenuated and insignificant. CONCLUSIONS: Folic acid therapy can reduce CVD risk in patients with ESRD/ACKD by 15%. A greater beneficial effect was observed among those trials with no or partial folic acid fortification or a decrease in Hcy level >20% regardless of folic acid fortification.
[本文引用:2]
|
| [125] |
AIMS: To evaluate the effects of homocysteine lowering intervention on the risk of cardiocerebrovascular events and all-cause mortality in randomised controlled trials among people with preexisting cardiocerebrovascular or renal disease. METHODS: Studies were retrieved by searching MEDLINE and OVID (from January 1966 to December 2008) using the following keywords: homocysteine, hyperhomocysteinaemia, cardiovascular disease, coronary disease, cerebrovascular disease, B vitamins, folic acid, randomised controlled trial. References of all retrieved articles were also searched. Randomised controlled trials which compared folic acid or plus B vitamins supplementation with either placebo or usual care were evaluated with cardiocerebrovascular disease events or all-cause mortality reported as an end-point. Data on study design, characteristics of participants, changes in homocysteine levels, and cardiocerebrovascular events and all-cause mortality were independently abstracted by two investigators using a standardised protocol. RESULTS: Seventeen trials involving 39,107 patients with preexisting cardiocerebrovascular or renal disease were included. Results of meta-analyses showed that no significant differences were identified between the intervention group and the control group. The overall relative risks (95% confidence intervals) of outcomes for patients treated with folic acid or plus B vitamins supplementation compared with controls were 1.01 (0.97-1.05) for cardiovascular events, 1.01 (0.94-1.07) for coronary heart disease, 0.94 (0.85-1.04) for stroke and 1.00 (0.95-1.05) for all-cause mortality. In the exclusion of low-quality trials and seven trials in grain fortification countries respectively, sensitivity analyses did not change the overall results. CONCLUSION: There is no sufficient evidence to show that homocysteine lowering intervention can reduce the risk of cardiocerebrovascular diseases or all-cause mortality among people with preexisting vascular disease. Folic acid supplementation should not be recommended for the secondary prevention of cardiocerebrovascular diseases. More evidence from large-scale randomised controlled trials is needed to confirm this.
[本文引用:1]
|
| [126] |
BACKGROUND: Results from observational and genetic epidemiological studies suggest that lower serum homocysteine levels are associated with lower incidence of cardiovascular disease (CVD). Numerous randomized controlled trials have investigated the efficacy of lowering homocysteine with folic acid supplementation for CVD risk, but conflicting results have been reported. METHODS AND RESULTS: Three bibliographic databases (Medline, Embase, and the Cochrane Database of Systematic Reviews) were searched from database inception until December 1, 2015. Of the 1933 references reviewed for eligibility, 30 randomized controlled trials involving 82 334 participants were included in the final analysis. The pooled relative risks of folic acid supplementation compared with controls were 0.90 (95% CI 0.84-0.96; P=0.002) for stroke, 1.04 (95% CI 0.99-1.09; P=0.16) for coronary heart disease, and 0.96 (95% CI 0.92-0.99; P=0.02) for overall CVD. The intervention effects for both stroke and combined CVD were more pronounced among participants with lower plasma folate levels at baseline (both P<0.02 for interaction). In stratified analyses, a greater beneficial effect for overall CVD was seen in trials among participants without preexisting CVD (P=0.006 for interaction) or in trials with larger reduction in homocysteine levels (P=0.009 for interaction). CONCLUSIONS: Our meta-analysis indicated a 10% lower risk of stroke and a 4% lower risk of overall CVD with folic acid supplementation. A greater benefit for CVD was observed among participants with lower plasma folate levels and without preexisting CVD and in studies with larger decreases in homocysteine levels. Folic acid supplementation had no significant effect on risk of coronary heart disease.
[本文引用:1]
|
| [127] |
|
| [128] |
|
| [129] |
BACKGROUND: Dietary supplementation with B vitamins that lower blood homocysteine concentrations is expected to reduce cardiovascular disease risk, but there has been uncertainty about the optimum regimen to use for this purpose. OBJECTIVE: The objectives were to ascertain the lowest dose of folic acid associated with the maximum reduction in homocysteine concentrations and to determine the additional relevance of vitamins B-12 and B-6. DESIGN: A meta-analysis of 25 randomized controlled trials involving individual data on 2596 subjects assessed the effect on plasma homocysteine concentrations of different doses of folic acid and of the addition of vitamins B-12 and B-6. RESULTS: The proportional reductions in plasma homocysteine concentrations produced by folic acid were greater at higher homocysteine (P < 0.001) and lower folate (P < 0.001) pretreatment concentrations; they were also greater in women than in men (P < 0.001). After standardization for sex and to pretreatment plasma concentrations of 12 micromol homocysteine/L and 12 nmol folate/L, daily doses of 0.2, 0.4, 0.8, 2.0, and 5.0 mg folic acid were associated with reductions in homocysteine of 13% (95% CI: 10%, 16%), 20% (17%, 22%), 23% (21%, 26%), 23% (20%, 26%), and 25% (22%, 28%), respectively. Vitamin B-12 (x: 0.4 mg/d) produced 7% (95% CI: 4%, 9%) further reduction in homocysteine concentrations, but vitamin B-6 had no significant effect. CONCLUSIONS: Daily doses of > or =0.8 mg folic acid are typically required to achieve the maximal reduction in plasma homocysteine concentrations produced by folic acid supplementation. Doses of 0.2 and 0.4 mg are associated with 60% and 90%, respectively, of this maximal effect.
[本文引用:1]
|
| [130] |
BACKGROUND AND AIMS: Inconsistent findings have been reported regarding the association between elevated plasma homocysteine (Hcy) levels and the risk of different types of strokes. We conducted this meta-analysis to identify the association between homocysteine (Hcy) levels and different kinds of strokes or recurrences of strokes. METHODS AND RESULTS: PubMed and Embase databases were searched for relevant studies published prior to April 2013. Only prospective studies that compared elevated Hcy levels with the risk of different types of strokes were selected. Results were presented as the relative risk (RR) and the corresponding 95% confidence intervals (CI) comparing the highest Hcy category group with the lowest Hcy category group. Nine studies composed of 13,284 participants were included. The pooled RR of ischemic strokes when comparing the highest Hcy category group with the lowest Hcy category group was 1.69 (95% CI: 1.29-2.20) in a fixed-effect model. The pooled RR of hemorrhagic strokes and recurrent strokes when comparing the highest Hcy category group with the lowest Hcy category group in a fixed-effect model was 1.65 (95% CI: 0.61-4.45) and 1.76 (95% CI: 1.37-2.24), respectively. CONCLUSIONS: This meta-analysis indicated that elevated Hcy levels are associated with an increased risk for ischemic strokes and recurrent strokes but had no distinct association with hemorrhagic strokes.
[本文引用:1]
|
| [131] |
OBJECTIVE: To assess whether the association of serum homocysteine concentration with ischaemic heart disease, deep vein thrombosis and pulmonary embolism, and stroke is causal and, if so, to quantify the effect of homocysteine reduction in preventing them. DESIGN: Meta-analyses of the above three diseases using (a) 72 studies in which the prevalence of a mutation in the MTHFR gene (which increases homocysteine) was determined in cases (n=16 849) and controls, and (b) 20 prospective studies (3820 participants) of serum homocysteine and disease risk. MAIN OUTCOME MEASURES: Odds ratios of the three diseases for a 5 micromol/l increase in serum homocysteine concentration. RESULTS: There were significant associations between homocysteine and the three diseases. The odds ratios for a 5 micromol/l increase in serum homocysteine were, for ischaemic heart disease, 1.42 (95% confidence interval 1.11 to 1.84) in the genetic studies and 1.32 (1.19 to 1.45) in the prospective studies; for deep vein thrombosis with or without pulmonary embolism, 1.60 (1.15 to 2.22) in the genetic studies (there were no prospective studies); and, for stroke, 1.65 (0.66 to 4.13) in the genetic studies and 1.59 (1.29 to 1.96) in the prospective studies. CONCLUSIONS: The genetic studies and the prospective studies do not share the same potential sources of error, but both yield similar highly significant results-strong evidence that the association between homocysteine and cardiovascular disease is causal. On this basis, lowering homocysteine concentrations by 3 micromol/l from current levels (achievable by increasing folic acid intake) would reduce the risk of ischaemic heart disease by 16% (11% to 20%), deep vein thrombosis by 25% (8% to 38%), and stroke by 24% (15% to 33%).
[本文引用:1]
|
| [132] |
OBJECTIVE: We related a panel of inflammatory biomarkers to risk of incident ischemic stroke (IIS) in a community-dwelling sample. METHODS: Stroke-free Framingham offspring attending examination cycle 7 (1998-2001) had 15 circulating inflammatory biomarkers measured. Cox proportional hazard models were used to calculate the hazard ratios (HRs) of IIS per SD increment of each biomarker. Model 1 included age and sex. Model 2 additionally adjusted for systolic blood pressure, hypertension treatment, current smoking, diabetes, cardiovascular disease, and atrial fibrillation. The continuous net reclassification improvement was used to assess the improvement in IIS risk prediction of statistically significant biomarkers from our main analysis over traditional stroke risk factors. RESULTS: In 3,224 participants (mean age 61 +/- 9 years, 54% women), 98 experienced IIS (mean follow-up of 9.8 [+/-2.2] years). In model 1, ln-C-reactive protein (ln-CRP) (HR 1.28, 95% confidence interval [CI] 1.04-1.56), ln-tumor necrosis factor receptor 2 (ln-TNFR2) (HR 1.33, 95% CI 1.09-1.63), ln-total homocysteine (ln-tHcy) (HR 1.32, 95% CI 1.11-1.58), and vascular endothelial growth factor (VEGF) (HR 1.25, 95% CI 1.07-1.46) were associated with risk of IIS. All associations, except for ln-CRP, remained significant in model 2 (ln-TNFR2: HR 1.24, 95% CI 1.02-1.51; ln-tHcy: HR 1.20, 95% CI 1.01-1.43; and VEGF: HR 1.21, 95% CI 1.04-1.42). The addition of these 4 biomarkers to the clinical Framingham Stroke Risk Profile score improved stroke risk prediction (net reclassification improvement: 0.34, 0.12-0.57; p < 0.05). CONCLUSIONS: Higher levels of 4 biomarkers-CRP, tHcy, TNFR2, and VEGF-increased risk of IIS and improved the predictive ability of the Framingham Stroke Risk Profile score. Further research is warranted to explore their role as potential therapeutic targets.
[本文引用:1]
|
| [133] |
BACKGROUND AND PURPOSE: Elevated total homocysteine is associated with a higher risk of cerebrovascular disease. It is not known whether lowering homocysteine impacts on stroke risk, both in terms of severity and ischemic vs hemorrhagic stroke subtypes. Our aim was to determine whether vitamin therapy reduces the risk of ischemic and hemorrhagic stroke, as well as stroke-related disability. METHODS: We analyzed stroke outcomes among participants of the Heart Outcomes Prevention Evaluation 2 (HOPE 2) trial that randomized 5522 adults with known cardiovascular disease to a daily combination of 2.5 mg of folic acid, 50 mg of vitamin B6, and 1 mg of vitamin B12, or matching placebo, for 5 years. RESULTS: Among 5522 participants, stroke occurred in 258 (4.7%) individuals during a mean of 5 years of follow-up. The geometric mean homocysteine concentration decreased by 2.2 micromol/L in the vitamin therapy group and increased by 0.80 micromol/L in the placebo group. The incidence rate of stroke was 0.88 per 100 person-years in the vitamin therapy group and 1.15 per 100 person-years in the placebo group (hazard ratio [HR], 0.75; 95% CI, 0.59-0.97). Vitamin therapy also reduced the risk of nonfatal stroke (HR, 0.72; 95% CI, 0.54-0.95) but did not impact on neurological deficit at 24 hours (P=0.45) or functional dependence at discharge or at 7 days (OR, 0.95; 95% CI, 0.57-1.56). In subgroup analysis, patients aged younger than 69 years, from regions without folic acid food fortification, with higher baseline cholesterol and homocysteine levels, and those not receiving antiplatelet or lipid-lowering drugs at enrollment had a larger treatment benefit. CONCLUSIONS: Lowering of homocysteine with folic acid and vitamins B6 and B12 did reduce the risk of overall stroke, but not stroke severity or disability.
[本文引用:1]
|
| [134] |
IMPORTANCE: Uncertainty remains about the efficacy of folic acid therapy for the primary prevention of stroke because of limited and inconsistent data. OBJECTIVE: To test the primary hypothesis that therapy with enalapril and folic acid is more effective in reducing first stroke than enalapril alone among Chinese adults with hypertension. DESIGN, SETTING, AND PARTICIPANTS: The China Stroke Primary Prevention Trial, a randomized, double-blind clinical trial conducted from May 19, 2008, to August 24, 2013, in 32 communities in Jiangsu and Anhui provinces in China. A total of 20,702 adults with hypertension without history of stroke or myocardial infarction (MI) participated in the study. INTERVENTIONS: Eligible participants, stratified by MTHFR C677T genotypes (CC, CT, and TT), were randomly assigned to receive double-blind daily treatment with a single-pill combination containing enalapril, 10 mg, and folic acid, 0.8 mg (n = 10,348) or a tablet containing enalapril, 10 mg, alone (n = 10,354). MAIN OUTCOMES AND MEASURES: The primary outcome was first stroke. Secondary outcomes included first ischemic stroke; first hemorrhagic stroke; MI; a composite of cardiovascular events consisting of cardiovascular death, MI, and stroke; and all-cause death. RESULTS: During a median treatment duration of 4.5 years, compared with the enalapril alone group, the enalapril-folic acid group had a significant risk reduction in first stroke (2.7% of participants in the enalapril-folic acid group vs 3.4% in the enalapril alone group; hazard ratio [HR], 0.79; 95% CI, 0.68-0.93), first ischemic stroke (2.2% with enalapril-folic acid vs 2.8% with enalapril alone; HR, 0.76; 95% CI, 0.64-0.91), and composite cardiovascular events consisting of cardiovascular death, MI, and stroke (3.1% with enalapril-folic acid vs 3.9% with enalapril alone; HR, 0.80; 95% CI, 0.69-0.92). The risks of hemorrhagic stroke (HR, 0.93; 95% CI, 0.65-1.34), MI (HR, 1.04; 95% CI, 0.60-1.82), and all-cause deaths (HR, 0.94; 95% CI, 0.81-1.10) did not differ significantly between the 2 treatment groups. There were no significant differences between the 2 treatment groups in the frequencies of adverse events. CONCLUSIONS AND RELEVANCE: Among adults with hypertension in China without a history of stroke or MI, the combined use of enalapril and folic acid, compared with enalapril alone, significantly reduced the risk of first stroke. These findings are consistent with benefits from folate use among adults with hypertension and low baseline folate levels. TRIAL REGISTRATION: clinicaltrials.gov Identifier: NCT00794885.
[本文引用:1]
|
| [135] |
Folic acid is generally used to lower homocysteine concentrations and prevent stroke and cardiovascular disease (CVD) at present. However, the efficacy of therapies that lower homocysteine concentrations in reducing the risk of CVD and stroke remains controversial. Our objective was to do a meta-analysis of relevant randomized controlled trials (RCTs) to evaluate the efficacy of folic acid supplementation among patients with hypertension and Hyperhomocysteinemia (HT/HHcy). We included RCTs examining the effects of folic acid plus antihypertensive therapy compared to antihypertensive alone. Weighted Mean Difference (WMD) and Relative risk (RR) were used as a measure of the effect of folic acid on the outcome measures with a random effect model. Sixty-five studies including 7887 patients met all inclusion criteria. Among them, 49 trials reported significant effect of combination therapy for reducing SBP (systolic Blood Pressure) and DBP (Diastolic Blood Pressure) levels compared with antihypertensive alone (WMD = -7.85, WMD = -6.77, respectively). Meanwhile, folic acid supplementation apparently reduced the level of total homocysteine (WMD = 5.5). In addition, folic acid supplementation obviously reduced the risk of cardiovascular and cerebrovascular events (CVCE) by 12.9% compared with control groups. In terms of the stratified analyses, a bigger beneficial effect was seen in those RCTs with treatment duration of more than 12 weeks, a decrease in the concentration of total homocysteine of more than 25%, with folic acid fortification. Our findings indicated that folic acid supplementation was effective in the primary prevention of CVCE among HT/HHcy patients, as well as reducing the blood pressure and total homocysteine levels.
[本文引用:1]
|
| [136] |
BACKGROUND: Controversy remains regarding the efficacy of folic acid supplementation in reducing the risk of stroke. This study aimed to evaluate the effect of folic acid supplementation on stroke prevention in patients with cardiovascular disease (CVD). MATERIALS AND METHODS: We searched the PubMed, EMBASE and Cochrane Library databases through October 2016 to identify randomized clinical trials of folic acid supplementation to prevent stroke in patients with CVD. Relative risks (RRs) with 95% CIs were used to examine the association between folic acid supplementation and the risk of stroke with a fixed-effect model. Stratified analyses were performed according to modifiers that may affect the efficacy of folic acid supplementation. RESULTS: Eleven studies with a total of 65,790 participants were included. Folic acid supplementation was associated with a significant benefit in reducing the risk of stroke in patients with CVD (RR = 0.90; 95% CI: 0.84-0.97; P = 0.005). In the stratified analysis, greater beneficial effects were observed in participants with a decrease in homocysteine concentrations of 25% or greater (RR = 0.85; 95% CI: 0.74-0.97; P = 0.03), those with a daily folate dose of less than 2mg (RR = 0.78; 95% CI: 0.68-0.89; P = 0.01), and populations in regions with no or partly fortified grain (RR = 0.87; 95% CI: 0.81-0.94; P = 0.04). CONCLUSIONS: Our meta-analysis demonstrated that folic acid supplementation is effective in stroke prevention in patients with CVD.
[本文引用:1]
|
| [137] |
OBJECTIVE: To examine the efficacy and effect modifiers of folic acid supplementation in the prevention of stroke in regions without folic acid fortification based on relevant, up-to-date published randomized trials. METHODS: Relative risk (RR) was used to measure the effect of folic acid supplementation on risk of stroke using a fixed effects model. FINDINGS: Overall, folic acid supplementation significantly reduced the stroke risk by 11% (22 trials, n = 82,723; RR 0.89, 95% confidence interval [CI] 0.84-0.96). The effect was greater in low folate regions (2 trials, n = 24,020; Asia, 0.78, 0.67-0.90) compared to high folate regions (7 trials, n = 14,655; America, 1.05, 0.90-1.23), and among patients without folic acid fortification (11 trials, n = 49,957; 0.85; 0.77-0.94) compared with those with folic acid fortification (7 trials, n = 14,655; 1.05, 0.90-1.23). In further stratified analyses among trials without folic acid fortification, a larger beneficial effect was found in those trials that used a low dosage of folic acid (
[本文引用:1]
|
| [138] |
Background Previous studies have suggested that any benefits of folic acid-based therapy to lower serum homocysteine in prevention of cardiovascular events might be offset by concomitant use of antiplatelet therapy. We aimed to establish whether there is an interaction between antiplatelet therapy and the effects of folic acid-based homocysteine-lowering therapy on major vascular events in patients with stroke or transient ischaemic attack enrolled in the vitamins to prevent stroke (VITATOPS) trial.
[本文引用:1]
Methods In the VITATOPS trial, 8164 patients with recent stroke or transient ischaemic attack were randomly allocated to double-blind treatment with one tablet daily of placebo or B vitamins (2 mg folic acid, 25 mg vitamin B-6, and 500 mu g vitamin B-12) and followed up for a median 3.4 years (IQR 2-0-5.5) for the primary composite outcome of stroke, myocardial infarction, or death from vascular causes. In our post-hoc analysis of the interaction between antiplatelet therapy and the effects of treatment with B vitamins on the primary outcome, we used Cox proportional hazards regression before and after adjusting for imbalances in baseline prognostic factors in participants who were and were not taking antiplatelet drugs at baseline and in participants assigned to receive B vitamins or placebo. We also assessed the interaction in different subgroups of patients and different secondary outcomes. The VITATOPS trial is registered with ClinicalTrials.gov, number NCT00097669, and Current Controlled Trials, number ISRCTN74743444. Findings At baseline, 6609 patients were taking antiplatelet therapy and 1463 were not. Patients not receiving antiplatelet therapy were more likely to be younger, east Asian, and disabled, to have a haemorrhagic stroke or cardioembolic ischaemic stroke, and to have a history of hypertension or atrial fibrillation. They were less likely to be smokers and to have a history of peripheral artery disease, hypercholesterolaemia, diabetes, ischaemic heart disease, and a revascularisation procedure. Of the participants taking antiplatelet drugs at baseline, B vitamins had no significant effect on the primary outcome (488 patients in the B-vitamins group [15%] vs 519 in the placebo group [16%]; hazard ratio [HA] 0.94, 95% CI 0.83-1.07). By contrast, of the participants not taking antiplatelet drugs at baseline, B vitamins had a significant effect on the primary outcome (123 in the B-vitamins group [17%] vs 153 in the placebo group [21%]; HR 0.76, 0.60-0.96). The interaction between antiplatelet therapy and the effect of B vitamins on the primary outcome was significant after adjusting for imbalance in the baseline variables (adjusted p for interaction=0.0204). Interpretation Our findings support the hypothesis that antiplatelet therapy modifies the potential benefits of lowering homocysteine with B-vitamin supplementation in the secondary prevention of major vascular events. If validated, B vitamins might have a role in the prevention of ischaemic events in high-risk individuals with an allergy, intolerance, or lack of indication for antiplatelet therapy. Funding Australia National Health and Medical Research Council, UK Medical Research Council, Singapore Biomedical Research Council, and Singapore National Medical Research Council. |
| [139] |
BACKGROUND: Epidemiological studies suggest that raised plasma concentrations of total homocysteine might be a risk factor for major vascular events. Whether lowering total homocysteine with B vitamins prevents major vascular events in patients with previous stroke or transient ischaemic attack is unknown. We aimed to assess whether the addition of once-daily supplements of B vitamins to usual medical care would lower total homocysteine and reduce the combined incidence of non-fatal stroke, non-fatal myocardial infarction, and death attributable to vascular causes in patients with recent stroke or transient ischaemic attack of the brain or eye. METHODS: In this randomised, double-blind, parallel, placebo-controlled trial, we assigned patients with recent stroke or transient ischaemic attack (within the past 7 months) from 123 medical centres in 20 countries to receive one tablet daily of placebo or B vitamins (2 mg folic acid, 25 mg vitamin B6, and 0.5 mg vitamin B12). Patients were randomly allocated by means of a central 24-h telephone service or an interactive website, and allocation was by use of random permuted blocks stratified by hospital. Participants, clinicians, carers, and investigators who assessed outcomes were masked to the assigned intervention. The primary endpoint was the composite of stroke, myocardial infarction, or vascular death. All patients randomly allocated to a group were included in the analysis of the primary endpoint. This trial is registered with ClinicalTrials.gov, NCT00097669, and Current Controlled Trials, ISRCTN74743444. FINDINGS: Between Nov 19, 1998, and Dec 31, 2008, 8164 patients were randomly assigned to receive B vitamins (n=4089) or placebo (n=4075). Patients were followed up for a median duration of 3.4 years (IQR 2.0-5.5). 616 (15%) patients assigned to B vitamins and 678 (17%) assigned to placebo reached the primary endpoint (risk ratio [RR] 0.91, 95% CI 0.82 to 1.00, p=0.05; absolute risk reduction 1.56%, -0.01 to 3.16). There were no unexpected serious adverse reactions and no significant differences in common adverse effects between the treatment groups. INTERPRETATION: Daily administration of folic acid, vitamin B6, and vitamin B12 to patients with recent stroke or transient ischaemic attack was safe but did not seem to be more effective than placebo in reducing the incidence of major vascular events. These results do not support the use of B vitamins to prevent recurrent stroke. The results of ongoing trials and an individual patient data meta-analysis will add statistical power and precision to present estimates of the effect of B vitamins. FUNDING: Australia National Health and Medical Research Council, UK Medical Research Council, Singapore Biomedical Research Council, Singapore National Medical Research Council, Australia National Heart Foundation, Royal Perth Hospital Medical Research Foundation, and Health Department of Western Australia.
[本文引用:1]
|
| [140] |
BACKGROUND: In cross-sectional studies, elevated plasma homocysteine levels have been associated with poor cognition and dementia. Studies of newly diagnosed dementia are required in order to establish whether the elevated homocysteine levels precede the onset of dementia or result from dementia-related nutritional and vitamin deficiencies. METHODS: A total of 1092 subjects without dementia (667 women and 425 men; mean age, 76 years) from the Framingham Study constituted our study sample. We examined the relation of the plasma total homocysteine level measured at base line and that measured eight years earlier to the risk of newly diagnosed dementia on follow-up. We used multivariable proportional-hazards regression to adjust for age, sex, apolipoprotein E genotype, vascular risk factors other than homocysteine, and plasma levels of folate and vitamins B12 and B6. RESULTS: Over a median follow-up period of eight years, dementia developed in 111 subjects, including 83 given a diagnosis of Alzheimer's disease. The multivariable-adjusted relative risk of dementia was 1.4 (95 percent confidence interval, 1.1 to 1.9) for each increase of 1 SD in the log-transformed homocysteine value either at base line or eight years earlier. The relative risk of Alzheimer's disease was 1.8 (95 percent confidence interval, 1.3 to 2.5) per increase of 1 SD at base line and 1.6 (95 percent confidence interval, 1.2 to 2.1) per increase of 1 SD eight years before base line. With a plasma homocysteine level greater than 14 micromol per liter, the risk of Alzheimer's disease nearly doubled. CONCLUSIONS: An increased plasma homocysteine level is a strong, independent risk factor for the development of dementia and Alzheimer's disease.
[本文引用:3]
|
| [141] |
BACKGROUND: In cross-sectional studies, elevated plasma total homocysteine (tHcy) concentrations have been associated with cognitive impairment and dementia. Incidence studies of this issue are few and have produced conflicting results. OBJECTIVE: We investigated the relation between high plasma tHcy concentrations and risk of dementia and Alzheimer disease (AD) in an elderly population. DESIGN: A dementia-free cohort of 816 subjects (434 women and 382 men; mean age: 74 y) from an Italian population-based study constituted our study sample. The relation of baseline plasma tHcy to the risk of newly diagnosed dementia and AD on follow-up was examined. A proportional hazards regression model was used to adjust for age, sex, education, apolipoprotein E genotype, vascular risk factors, and serum concentrations of folate and vitamin B-12. RESULTS: Over an average follow-up of 4 y, dementia developed in 112 subjects, including 70 who received a diagnosis of AD. In the subjects with hyperhomocysteinemia (plasma tHcy > 15 micromol/L), the hazard ratio for dementia was 2.08 (95% CI: 1.31, 3.30; P = 0.002). The corresponding hazard ratio for AD was 2.11 (95% CI: 1.19, 3.76; P = 0.011). Independently of hyperhomocysteinemia and other confounders, low folate concentrations (< or = 11.8 nmol/L) were also associated with an increased risk of both dementia (1.87; 95% CI: 1.21, 2.89; P = 0.005) and AD (1.98; 95% CI: 1.15, 3.40; P = 0.014), whereas the association was not significant for vitamin B-12. CONCLUSIONS: Elevated plasma tHcy concentrations and low serum folate concentrations are independent predictors of the development of dementia and AD.
[本文引用:2]
|
| [142] |
Elevated plasma homocysteine (Hcy) concentrations have been implicated with risk of cognitive impairment and dementia, but it is unclear whether low vitamin B12 or folate status is responsible for cognitive decline. Most studies reporting associations between cognitive function and Hcy or B-vitamins have used a cross-sectional or case-control design and have been unable to exclude the possibility that such associations are a result of the disease rather than being causal. The Hcy hypothesis of dementia has attracted considerable interest, as Hcy can be easily lowered by folic acid and vitamin B12, raising the prospect that B-vitamin supplementation could lower the risk of dementia. While some trials assessing effects on cognitive function have used folic acid alone, vitamin B12 alone or a combination, few trials have included a sufficient number of participants to provide reliable evidence. An individual-patient-data meta-analysis of all randomised trials of the effects on cognitive function and vascular risk of lowering Hcy with B-vitamins will maximise the power to assess the epidemiologically-predicted differences in risk. Among the twelve large randomised Hcy-lowering trials for prevention of vascular disease, data should be available on about 30 000 participants with cognitive function. The principal investigators of such trials have agreed to combine individual-participant data from their trials after their separate publication.
[本文引用:1]
|
| [143] |
Moderately elevated plasma total homocysteine (tHcy) is a strong modifiable risk factor for vascular dementia and Alzheimer's disease. Prospectively, elevated tHcy is associated with cognitive decline, white matter damage, brain atrophy, neurofibrillary tangles, and dementia. Most homocysteine-lowering trials with folate and vitamins B6 and/or B12 tested as protective agents against cognitive decline were poorly designed by including subjects unlikely to benefit during the trial period. In contrast, trials in high-risk subjects, which have taken into account the baseline B vitamin status, show a slowing of cognitive decline and of atrophy in critical brain regions, results that are consistent with modification of the Alzheimer's disease process. Homocysteine may interact with both risk factors and protective factors, thereby identifying people at risk but also providing potential strategies for early intervention. Public health steps to slow cognitive decline should be promoted in individuals who are at risk of dementia, and more trials are needed to see if simple interventions with nutrients can prevent progression to dementia.
[本文引用:3]
|
| [144] |
Identification of modifiable risk factors provides a crucial approach to the prevention of dementia. Nutritional or nutrient-dependent risk factors are especially important because dietary modifications or use of dietary supplements may lower the risk factor level. One such risk factor is a raised concentration of the biomarker plasma total homocysteine, which reflects the functional status of three B vitamins (folate, vitamins B12, B6). A group of experts reviewed literature evidence from the last 20 years. We here present a Consensus Statement, based on the Bradford Hill criteria, and conclude that elevated plasma total homocysteine is a modifiable risk factor for development of cognitive decline, dementia, and Alzheimer's disease in older persons. In a variety of clinical studies, the relative risk of dementia in elderly people for moderately raised homocysteine (within the normal range) ranges from 1.15 to 2.5, and the Population Attributable risk ranges from 4.3 to 31%. Intervention trials in elderly with cognitive impairment show that homocysteine-lowering treatment with B vitamins markedly slows the rate of whole and regional brain atrophy and also slows cognitive decline. The findings are consistent with moderately raised plasma total homocysteine (>11 mumol/L), which is common in the elderly, being one of the causes of age-related cognitive decline and dementia. Thus, the public health significance of raised tHcy in the elderly should not be underestimated, since it is easy, inexpensive, and safe to treat with B vitamins. Further trials are needed to see whether B vitamin treatment will slow, or prevent, conversion to dementia in people at risk of cognitive decline or dementia.
[本文引用:1]
|
| [145] |
Alzheimer's disease (AD) is considered the most frequent cause of dementia. It is known that vascular risk factors play an important role in the development and progression of this condition. Alterations in vascular walls represent documented findings in patients with AD and other dementias affecting elderly people. The authors performed a systematic review and meta-analysis, aiming to synthesize observational studies that evaluated how the hemostatic system may contribute to cognitive decline in the elderly, using papers published until April 2018 and as indexed in Medline (PubMed), Scopus, Web of Science, ScienceDirect, Lilacs, Cinahl, PsycINFO, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews. Among 5,278 studies identified, 32 were included in the final synthesis, and these included 485 patients with mild cognitive impairment, 568 with vascular dementia (VD), 1,781 with AD, and 2,855 participants without dementia. AD patients had increased plasma von Willebrand factor (VWF) (standardized mean difference [SMD]: 2.53; 95% confidence interval [CI]: 0.10-4.95), D-dimer (SMD: 0.50; 95% CI: 0.35-0.66), plasminogen activator inhibitor-1 (SMD: 3.34; 95% CI: 1.01-5.67), thrombomodulin (SMD: 1.08; 95% CI: 0.53-1.62), and homocysteine levels (SMD: 0.65; 95% CI: 0.15-1.15). In contrast, the VD group showed increased fibrinogen levels (SMD: 0.77; 95% CI: 0.13-1.41), activated factor VII (SMD: 0.36; 95% CI: 0.05-0.67), factor VIII (SMD: 0.57; 95% CI: 0.22-0.91), VWF (SMD: 2.34; 95% CI: 0.38-4.29), D-dimer (SMD: 1.14; 95% CI: 0.51-1.78), and homocysteine (SMD: 2.17; 95% CI: 1.67-2.68). AD showed an elevation in some markers of endothelial dysfunction, whereas VD presented mostly an involvement of coagulation cascade components.
[本文引用:1]
|
| [146] |
OBJECTIVE: This study aimed to comprehensively assess the dose-response relationship between blood homocysteine levels and risk of all cause, Alzheimer and vascular dementia, as well as cognitive impairment without dementia (CIND). METHOD: We searched for all related prospective cohort studies reporting homocysteine as an exposure from patients with cognitive disorders as a result in the PubMed and EMBASE databases up to June 18, 2018. Pooled relative risks (RRs) and corresponding 95% confidence intervals (CIs) were extracted. The dose-response meta-analyses were conducted to assess potential linear and non-linear dose-response relations. Summary RRs and 95% CIs were calculated using a random- or fixed-effects model. RESULTS: Twenty-eight prospective cohort studies were eligible in this meta-analysis. During average follow-up periods ranging from 2.7 to 35 years there were 2557 cases (1035 all-cause dementia, 530 Alzheimer's disease, 92 vascular dementia and > 900 CIND) among 28,257 participants. There was a clear linear dose-response relationship between blood homocysteine concentration and risk of Alzheimer-type dementia (P > 0.05 for non-linearity). The pooled RR of Alzheimer-type dementia was 1.15 (95% CI: 1.04 to 1.26; I(2) = 56.6%, n = 5) for every 5 mumol/L increase in blood homocysteine. Sensitivity analysis showed similar results, and there was no clear evidence of publication bias with Begg's and Egger's tests for Alzheimer dementia (P = 0.806, 0.084, respectively), strengthening the linear relationship between blood homocysteine levels and risk of Alzheimer dementia. Due to the presence of publication bias and low statistical power, elevated levels of blood homocysteine were not appreciably associated with risk of all-cause, vascular dementia and CIND. CONCLUSIONS: Every 5 mumol/L increase in blood homocysteine is linearly associated with a 15% increase in relative risk of Alzheimer-type dementia. This meta-analysis provides further evidence that a higher concentration of blood homocysteine is associated with a higher risk of Alzheimer-type dementia.
[本文引用:1]
|
| [147] |
|
| [148] |
|
| [149] |
BACKGROUND: Low folate and raised homocysteine concentrations in blood are associated with poor cognitive performance in the general population. As part of the FACIT trial to assess the effect of folic acid on markers of atherosclerosis in men and women aged 50-70 years with raised plasma total homocysteine and normal serum vitamin B12 at screening, we report here the findings for the secondary endpoint: the effect of folic acid supplementation on cognitive performance. METHODS: Our randomised, double blind, placebo controlled study took place between November, 1999, and December, 2004, in the Netherlands. We randomly assigned 818 participants 800 mug daily oral folic acid or placebo for 3 years. The effect on cognitive performance was measured as the difference between the two groups in the 3-year change in performance for memory, sensorimotor speed, complex speed, information processing speed, and word fluency. Analysis was by intention-to-treat. This trial is registered with clinicaltrials.gov with trial number NCT00110604. FINDINGS: Serum folate concentrations increased by 576% (95% CI 539 to 614) and plasma total homocysteine concentrations decreased by 26% (24 to 28) in participants taking folic acid compared with those taking placebo. The 3-year change in memory (difference in Z scores 0.132, 95% CI 0.032 to 0.233), information processing speed (0.087, 0.016 to 0.158) and sensorimotor speed (0.064, -0.001 to 0.129) were significantly better in the folic acid group than in the placebo group. INTERPRETATION: Folic acid supplementation for 3 years significantly improved domains of cognitive function that tend to decline with age.
[本文引用:1]
|
| [150] |
BACKGROUND: Vitamin B-12 deficiency is associated with cognitive impairment in older people. However, evidence from randomized trials of the effects of vitamin B-12 supplementation on cognitive function is limited and inconclusive. OBJECTIVE: The objective was to investigate whether daily supplementation with high doses of oral vitamin B-12 alone or in combination with folic acid has any beneficial effects on cognitive function in persons aged >/=70 y with mild vitamin B-12 deficiency. DESIGN: In a double-blind, placebo-controlled trial, 195 subjects were randomly assigned to receive 1000 microg vitamin B-12, 1000 microg vitamin B-12 + 400 microg folic acid, or placebo for 24 wk. Vitamin B-12 status was assessed on the basis of methylmalonic acid, total homocysteine (tHcy), and holotranscobalamin (holoTC) concentrations before and after 12 and 24 wk of treatment. Cognitive function was assessed before and after 24 wk of treatment with the use of an extensive neuropsychologic test battery that included the domains of attention, construction, sensomotor speed, memory, and executive function. RESULTS: Vitamin B-12 status did not change significantly after treatment in the placebo group; however, oral vitamin B-12 supplementation corrected mild vitamin B-12 deficiency. Vitamin B-12 + folic acid supplementation increased red blood cell folate concentrations and decreased tHcy concentrations by 36%. Improvement in memory function was greater in the placebo group than in the group who received vitamin B-12 alone (P = 0.0036). Neither supplementation with vitamin B-12 alone nor that in combination with folic acid was accompanied by any improvement in other cognitive domains. CONCLUSION: Oral supplementation with vitamin B-12 alone or in combination with folic acid for 24 wk does not improve cognitive function.
[本文引用:1]
|
| [151] |
|
| [152] |
|
| [153] |
CONTEXT: Blood levels of homocysteine may be increased in Alzheimer disease (AD) and hyperhomocysteinemia may contribute to disease pathophysiology by vascular and direct neurotoxic mechanisms. Even in the absence of vitamin deficiency, homocysteine levels can be reduced by administration of high-dose supplements of folic acid and vitamins B(6) and B(12). Prior studies of B vitamins to reduce homocysteine in AD have not had sufficient size or duration to assess their effect on cognitive decline. OBJECTIVE: To determine the efficacy and safety of B vitamin supplementation in the treatment of AD. DESIGN, SETTING, AND PATIENTS: A multicenter, randomized, double-blind controlled clinical trial of high-dose folate, vitamin B(6), and vitamin B(12) supplementation in 409 (of 601 screened) individuals with mild to moderate AD (Mini-Mental State Examination scores between 14 and 26, inclusive) and normal folic acid, vitamin B(12), and homocysteine levels. The study was conducted between February 20, 2003, and December 15, 2006, at clinical research sites of the Alzheimer Disease Cooperative Study located throughout the United States. INTERVENTION: Participants were randomly assigned to 2 groups of unequal size to increase enrollment (60% treated with high-dose supplements [5 mg/d of folate, 25 mg/d of vitamin B(6), 1 mg/d of vitamin B(12)] and 40% treated with identical placebo); duration of treatment was 18 months. MAIN OUTCOME MEASURE: Change in the cognitive subscale of the Alzheimer Disease Assessment Scale (ADAS-cog). RESULTS: A total of 340 participants (202 in active treatment group and 138 in placebo group) completed the trial while taking study medication. Although the vitamin supplement regimen was effective in reducing homocysteine levels (mean [SD], -2.42 [3.35] in active treatment group vs -0.86 [2.59] in placebo group; P < .001), it had no beneficial effect on the primary cognitive measure, rate of change in ADAS-cog score during 18 months (0.372 points per month for placebo group vs 0.401 points per month for active treatment group, P = .52; 95% confidence interval of rate difference, -0.06 to 0.12; based on the intention-to-treat generalized estimating equations model), or on any secondary measures. A higher quantity of adverse events involving depression was observed in the group treated with vitamin supplements. CONCLUSION: This regimen of high-dose B vitamin supplements does not slow cognitive decline in individuals with mild to moderate AD. TRIAL REGISTRATION: clinicaltrials.gov Identifier: NCT00056225.
[本文引用:1]
|
| [154] |
BACKGROUND: Evidence remains unclear as to whether folic acid (FA) and vitamin B-12 supplementation is effective in reducing depressive symptoms. OBJECTIVES: The objective was to determine whether oral FA + vitamin B-12 supplementation prevented cognitive decline in a cohort of community-dwelling older adults with elevated psychological distress. DESIGN: A randomized controlled trial (RCT) with a completely crossed 2 x 2 x 2 factorial design comprising daily oral 400 mug FA + 100 mug vitamin B-12 supplementation (compared with placebo), physical activity promotion, and depression literacy with comparator control interventions for reducing depressive symptoms was conducted in 900 adults aged 60-74 y with elevated psychological distress (Kessler Distress 10-Scale; scores >15). The 2-y intervention was delivered in 10 modules via mail with concurrent telephone tracking calls. Main outcome measures examined change in cognitive functioning at 12 and 24 mo by using the Telephone Interview for Cognitive Status-Modified (TICS-M) and the Brief Test of Adult Cognition by Telephone (processing speed); the Informant Questionnaire on Cognitive Decline in the Elderly was administered at 24 mo. RESULTS: FA + vitamin B-12 improved the TICS-M total (P = 0.032; effect size d = 0.17), TICS-M immediate (P = 0.046; d = 0.15), and TICS-M delayed recall (P = 0.013; effect size d = 0.18) scores at 24 mo in comparison with placebo. No significant changes were evident in orientation, attention, semantic memory, processing speed, or informant reports. CONCLUSION: Long-term supplementation of daily oral 400 mug FA + 100 mug vitamin B-12 promotes improvement in cognitive functioning after 24 mo, particularly in immediate and delayed memory performance. This trial was registered at clinicaltrials.gov as NCT00214682.
[本文引用:1]
|
| [155] |
|
| [156] |
|
| [157] |
|
| [158] |
|
| [159] |
|
| [160] |
|
| [161] |
|
| [162] |
|
| [163] |
|
| [164] |
|
| [165] |
|
| [166] |
|
| [167] |
|
| [168] |
OBJECTIVE: The authors conducted two multicenter sequential parallel comparison design trials to investigate the effect of L-methylfolate augmentation in the treatment of major depressive disorder in patients who had a partial response or no response to selective serotonin reuptake inhibitors (SSRIs). METHOD: In the first trial, 148 outpatients with SSRI-resistant major depressive disorder were enrolled in a 60-day study divided into two 30-day periods. Patients were randomly assigned, in a 2:3:3 ratio, to receive L-methylfolate for 60 days (7.5 mg/day for 30 days followed by 15 mg/day for 30 days), placebo for 30 days followed by L-methylfolate (7.5 mg/day) for 30 days, or placebo for 60 days. SSRI dosages were kept constant throughout the study. In the second trial, with 75 patients, the design was identical to the first, except that the l-methylfolate dosage was 15 mg/day during both 30-day periods. RESULTS: In the first trial, no significant difference was observed in outcomes between the treatment groups. In the second trial, adjunctive L-methylfolate at 15 mg/day showed significantly greater efficacy compared with continued SSRI therapy plus placebo on both primary outcome measures (response rate and degree of change in depression symptom score) and two secondary outcome measures of symptom severity. The number needed to treat for response was approximately six in favor of adjunctive L-methylfolate at 15 mg/day. L-Methylfolate was well tolerated, with rates of adverse events no different from those reported with placebo. CONCLUSIONS: Adjunctive L-methylfolate at 15 mg/day may constitute an effective, safe, and relatively well tolerated treatment strategy for patients with major depressive disorder who have a partial response or no response to SSRIs.
[本文引用:1]
|
| [169] |
|
| [170] |
|
| [171] |
|
| [172] |
|
| [173] |
Background: Hyperhomocysteinemia (Hhcy) occurs in about 85% of chronic kidney disease (CKD) patients because of impaired renal metabolism and reduced renal excretion. Folic acid (FA), the synthetic form of vitamin B9, is critical in the conversion of homocysteine (Hcy) to methionine. If there is not enough intake of FA, there is not enough conversion, and Hcy levels are raised. Summary: Hhcy is regarded as an independent predictor of cardiovascular morbidity and mortality in end-stage renal disease. Hhcy exerts its pathogenic action on the main processes involved in the progression of vascular damage. Research has shown Hhcy suggests enhanced risks for inflammation and endothelial injury which lead to cardiovascular disease (CVD), stroke, and CKD. FA has also been shown to improve endothelial function without lowering Hcy, suggesting an alternative explanation for the effect of FA on endothelial function. Recently, the role of FA and Hhcy in CVD and in CKD progression was renewed in some randomized trials. Key Messages: In the general population and in CKD patients, it remains a topic of discussion whether any beneficial effects of FA therapy are to be referred to its direct effect or to a reduction of Hhcy. While waiting for the results of confirmatory trials, it is reasonable to consider FA with or without methylcobalamin supplementation as appropriate adjunctive therapy in patients with CKD.
[本文引用:1]
|
| [174] |
Importance: The efficacy of folic acid therapy on renal outcomes has not been previously investigated in populations without folic acid fortification. Objective: To test whether treatment with enalapril and folic acid is more effective in slowing renal function decline than enalapril alone across a spectrum of renal function at baseline from normal to moderate chronic kidney disease (CKD) among Chinese adults with hypertension. Design, Setting, and Participants: In this substudy of eligible China Stroke Primary Prevention Trial (CSPPT), 15104 participants with an estimated glomerular filtration rate (eGFR) 30 mL/min/1.73 m2 or greater, including 1671 patients with CKD, were recruited from 20 communities in Jiangsu province in China. Interventions: Participants were randomized to receive a single tablet daily containing 10 mg enalapril and 0.8 mg folic acid (n = 7545) or 10 mg enalapril alone (n = 7559). Main Outcomes and Measures: The primary outcome was the progression of CKD, defined as a decrease in eGFR of 30% or more and to a level of less than 60 mL/min/1.73 m2 if the baseline eGFR was 60 mL/min/1.73 m2 or more, or a decrease in eGFR of 50% or more if the baseline eGFR was less than 60 mL/min/1.73 m2; or end-stage renal disease. Secondary outcomes included a composite of the primary outcome and all-cause death, rapid decline in renal function, and rate of eGFR decline. Results: Overall, 15104 Chinese adults with a mean (range) age of 60 (45-75) years were recruited; median follow-up was 4.4 years. There were 164 and 132 primary events in the enalapril group and the enalapril-folic acid group, respectively. Compared with the enalapril group, the enalapril-folic acid group had a 21% reduction in the odds of the primary event (odds ratio [OR], 0.79; 95% CI, 0.62-1.00) and a slower rate of eGFR decline (1.28% vs 1.42% per year; P = .02). Among the participants with CKD at baseline, folic acid therapy resulted in a significant reduction in the risks for the primary event (OR, 0.44; 95% CI, 0.26-0.75), rapid decline in renal function (OR, 0.67; 95% CI, 0.47-0.96) and the composite event (OR, 0.62; 95% CI, 0.43-0.90), and a 44% slower decline in renal function (0.96% vs 1.72% per year, P < .001). Among those without CKD at baseline, there was no between-group difference in the primary end point. Conclusions and Relevance: Enalapril-folic acid therapy, compared with enalapril alone, can significantly delay the progression of CKD among patients with mild-to-moderate CKD. Trial Registration: clinicaltrials.gov Identifier: NCT00794885.
[本文引用:2]
|
| [175] |
|
| [176] |
|
| [177] |
CONTEXT: Hyperhomocysteinemia is frequently observed in patients with diabetic nephropathy. B-vitamin therapy (folic acid, vitamin B(6), and vitamin B(12)) has been shown to lower the plasma concentration of homocysteine. OBJECTIVE: To determine whether B-vitamin therapy can slow progression of diabetic nephropathy and prevent vascular complications. DESIGN, SETTING, AND PARTICIPANTS: A multicenter, randomized, double-blind, placebo-controlled trial (Diabetic Intervention with Vitamins to Improve Nephropathy [DIVINe]) at 5 university medical centers in Canada conducted between May 2001 and July 2007 of 238 participants who had type 1 or 2 diabetes and a clinical diagnosis of diabetic nephropathy. INTERVENTION: Single tablet of B vitamins containing folic acid (2.5 mg/d), vitamin B(6) (25 mg/d), and vitamin B(12) (1 mg/d), or matching placebo. MAIN OUTCOME MEASURES: Change in radionuclide glomerular filtration rate (GFR) between baseline and 36 months. Secondary outcomes were dialysis and a composite of myocardial infarction, stroke, revascularization, and all-cause mortality. Plasma total homocysteine was also measured. RESULTS: The mean (SD) follow-up during the trial was 31.9 (14.4) months. At 36 months, radionuclide GFR decreased by a mean (SE) of 16.5 (1.7) mL/min/1.73 m(2) in the B-vitamin group compared with 10.7 (1.7) mL/min/1.73 m(2) in the placebo group (mean difference, -5.8; 95% confidence interval [CI], -10.6 to -1.1; P = .02). There was no difference in requirement of dialysis (hazard ratio [HR], 1.1; 95% CI, 0.4-2.6; P = .88). The composite outcome occurred more often in the B-vitamin group (HR, 2.0; 95% CI, 1.0-4.0; P = .04). Plasma total homocysteine decreased by a mean (SE) of 2.2 (0.4) micromol/L at 36 months in the B-vitamin group compared with a mean (SE) increase of 2.6 (0.4) micromol/L in the placebo group (mean difference, -4.8; 95% CI, -6.1 to -3.7; P < .001, in favor of B vitamins). CONCLUSION: Among patients with diabetic nephropathy, high doses of B vitamins compared with placebo resulted in a greater decrease in GFR and an increase in vascular events. TRIAL REGISTRATION: isrctn.org Identifier: ISRCTN41332305.
[本文引用:2]
|
| [178] |
We aimed to test the hypothesis that treatment with enalapril and folic acid is more effective in preventing new-onset proteinuria than enalapril alone among hypertensive patients. This is a post hoc analysis of the renal substudy of the CSPPT (China Stroke Primary Prevention Trial). A total of 13 071 eligible participants without proteinuria were randomized to receive a double-blind daily treatment of a single tablet containing 10-mg enalapril and 0.8-mg folic acid (n=6511) or 10-mg enalapril alone (n=6560). The primary outcome was new-onset proteinuria, defined as a urine dipstick reading of >/=1+ at the exit visit. Secondary outcomes included a composite of the primary outcome and all-cause death and the annual rate of estimated glomerular filtration rate decline. After a median 4.4 years of treatment, the primary event occurred in 213 (3.9%) and 188 (3.5%) participants, respectively, in the enalapril and the enalapril-folic acid group (odds ratio, 0.90; 95% confidence interval, 0.74-1.11). However, among participants with diabetes mellitus at baseline, folic acid therapy resulted in a significant reduction in the risk for the primary event (3.7% in the enalapril-folic acid group versus 7.4% in the enalapril group; odds ratio, 0.48; 95% confidence interval, 0.29-0.81) and the composite event (odds ratio, 0.62; 95% confidence interval, 0.42-0.92) and a 55% slower annual rate of estimated glomerular filtration rate decline (0.5% versus 1.1% per year; P=0.002). Among those without diabetes mellitus at baseline, there were no between-group differences in all the outcomes. In conclusion, enalapril-folic acid therapy, compared with enalapril alone, significantly reduced the development of proteinuria in diabetic patients with hypertension. CLINICAL TRIAL REGISTRATION: URL: http://www.ClinicalTrials.gov. Unique identifier: NCT00794885.
[本文引用:1]
|
| [179] |
|
| [180] |
BACKGROUND & AIMS: The efficacy of homocysteine-lowering therapy with folic acid to lower homocysteine levels in an effort to reduce cardiovascular disease (CVD) risk in patients with kidney disease remains inconclusive. We conducted a meta-analysis of relevant randomized trials to further examine this issue. METHODS: This meta-analysis included 8234 patients with kidney disease from nine qualified randomized trials using folic acid therapy, and with CVD reported as one of the endpoints. Relative risk (RR) was used to measure the effect of folic acid supplementation on risk of CVD using a random effects model. RESULTS: When pooling the nine randomized trials, folic acid therapy reduced the risk of CVD by 10%RR = 0.90; 95% CI:0.81-1.00, P = 0.046). A greater beneficial effect was observed among those trials without a history of grain fortification with folic acid (0.82; 0.70-0.96, P = 0.01), with lower percent baseline diabetes (<30% (median), 0.80; 0.65-0.99, P = 0.04), and in patients with end-stage renal disease (ESRD) or advanced chronic kidney disease (ACKD) (0.85; 0.77-0.94, P = 0.002). Furthermore, a meta-regression analysis suggested a positive dose-response relationship between percent baseline diabetes and log-RR for CVD risk associated with folic acid supplementation (P = 0.007). Most importantly, even the inclusion of three subgroup results did not substantially affect the results (n = 11032, RR: 0.93; 95% CI:0.87-0.99, P = 0.03). CONCLUSIONS: Our meta-analysis indicates that folic acid supplementation may be effective for CVD prevention in patients with kidney disease, particularly in trials among patients without a history of grain fortification with folic acid, with lower percent baseline diabetes, and in patients with ESRD or ACKD.
[本文引用:1]
|
| [181] |
|
| [182] |
|
| [183] |
In this article, the 2010 European League against Rheumatism (EULAR) recommendations for the management of rheumatoid arthritis (RA) with synthetic and biological disease-modifying antirheumatic drugs (sDMARDs and bDMARDs, respectively) have been updated. The 2013 update has been developed by an international task force, which based its decisions mostly on evidence from three systematic literature reviews (one each on sDMARDs, including glucocorticoids, bDMARDs and safety aspects of DMARD therapy); treatment strategies were also covered by the searches. The evidence presented was discussed and summarised by the experts in the course of a consensus finding and voting process. Levels of evidence and grades of recommendations were derived and levels of agreement (strengths of recommendations) were determined. Fourteen recommendations were developed (instead of 15 in 2010). Some of the 2010 recommendations were deleted, and others were amended or split. The recommendations cover general aspects, such as attainment of remission or low disease activity using a treat-to-target approach, and the need for shared decision-making between rheumatologists and patients. The more specific items relate to starting DMARD therapy using a conventional sDMARD (csDMARD) strategy in combination with glucocorticoids, followed by the addition of a bDMARD or another csDMARD strategy (after stratification by presence or absence of adverse risk factors) if the treatment target is not reached within 6 months (or improvement not seen at 3 months). Tumour necrosis factor inhibitors (adalimumab, certolizumab pegol, etanercept, golimumab, infliximab, biosimilars), abatacept, tocilizumab and, under certain circumstances, rituximab are essentially considered to have similar efficacy and safety. If the first bDMARD strategy fails, any other bDMARD may be used. The recommendations also address tofacitinib as a targeted sDMARD (tsDMARD), which is recommended, where licensed, after use of at least one bDMARD. Biosimilars are also addressed. These recommendations are intended to inform rheumatologists, patients, national rheumatology societies and other stakeholders about EULAR's most recent consensus on the management of RA with sDMARDs, glucocorticoids and bDMARDs. They are based on evidence and expert opinion and intended to improve outcome in patients with RA.
[本文引用:1]
|
| [184] |
|
| [185] |
OBJECTIVE: To perform a systematic review of the benefits and harms of folic acid and folinic acid in reducing the mucosal, gastrointestinal, hepatic, and hematologic side effects of methotrexate (MTX); and to assess whether folic or folinic acid supplementation has any effect on MTX benefit. METHODS: We searched the Cochrane Library, MEDLINE, EMBASE, and US National Institutes of Health clinical trials registry from inception to March 2012. We selected all double-blind, randomized, placebo-controlled clinical trials in which adult patients with rheumatoid arthritis (RA) were treated with MTX (dose
[本文引用:1]
|
| [186] |
|
| [187] |
A double blind, placebo controlled trial examined the effects of folinic acid on the efficacy and toxicity of methotrexate in 27 patients with rheumatoid arthritis. Clinical and laboratory indices of disease activity worsened significantly in the 13 patients treated with folinic acid after four weeks of treatment, but not in the 14 patients treated with placebo. Exacerbation of rheumatoid arthritis led to withdrawal of the test drug in seven of the patients treated with folinic acid but in none of those treated with placebo. It is concluded that excerbation of rheumatoid arthritis is likely when folinic acid is given shortly after the weekly dose of methotrexate.
[本文引用:1]
|
| [188] |
|
| [189] |
|
| [190] |
|
| [191] |
|
| [192] |
|
| [193] |
|

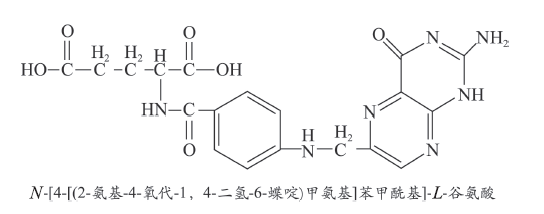
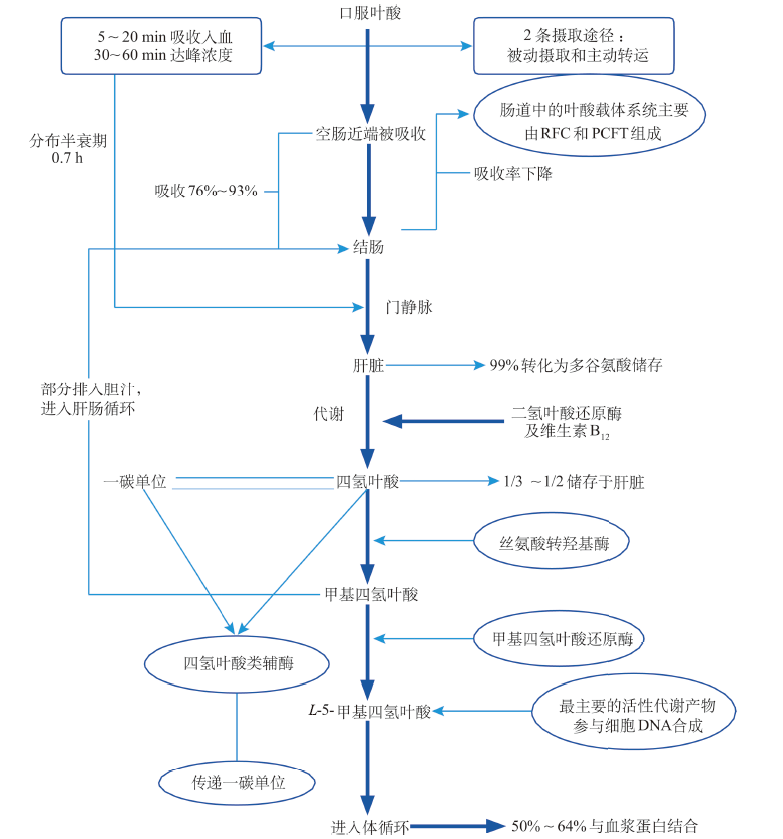
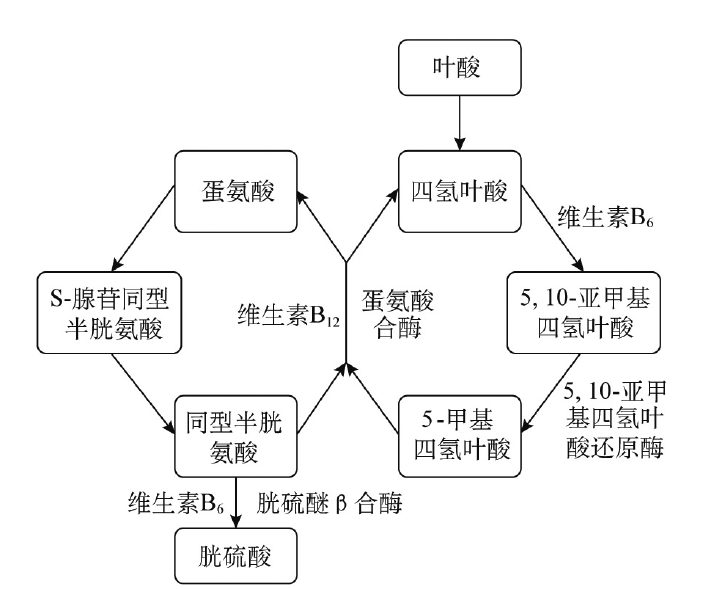
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}